Chapter 91 I think my baby can’t see!
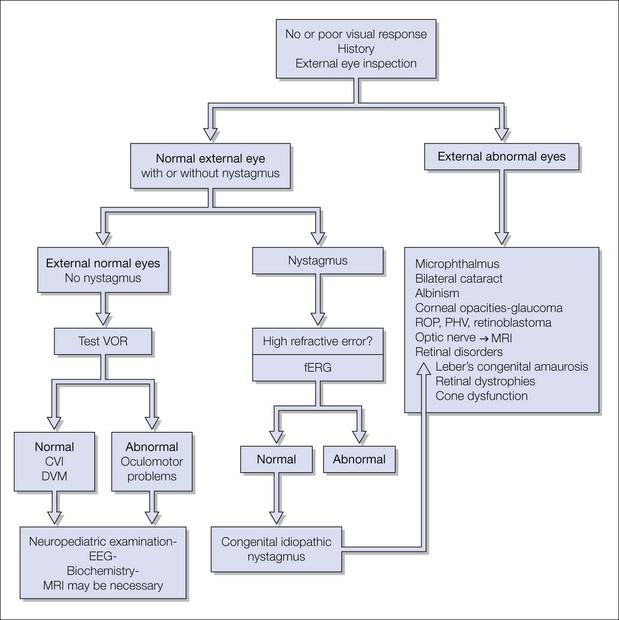
Normally, a full-term baby shows visual fixation at birth or shortly afterward. Absent, poor, or delayed visual contact is a common reason parents bring their baby to their ophthalmologist. They are anxious to understand why the baby seems not to see, and want to know the cause and prognosis. Although this is not usually a medical emergency, parents need to have their baby diagnosed soon. This is a challenge. In some babies the underlying cause is evident on clinical examination; in others, additional investigation will be necessary. The diagnosis depends on a thorough birth, family and clinical history and a systematic clinical examination (Fig. 91.1). The clinician should verify the cause and degree of visual impairment, give a prognosis, and make a plan of management and counseling for the family.
History
Was the baby premature? Visual development depends on the postmenstrual age at birth. Premature infants with intraventricular hemorrhage are at risk of optic atrophy (see Chapter 53), hydrocephalus, and cerebral visual impairment (CVI) (see Chapters 56 and 57). Visual development in premature babies can also be delayed due to associated retinal or neurological problems. The presence of seizures, developmental delay, and dysmorphic features may suggest a brain problem. Maternal infections, medication during pregnancy, trauma, and hypoxia can have significant visual consequences.
A positive family history, or a history of consanguinity, makes certain diseases more likely. For instance, a baby born to first cousin parents with searching eye movements and hypermetropia is very likely to have a congenital retinal dystrophy (see Chapter 44). The pediatric ophthalmologist should inquire about other family members, examine them and the first-degree relatives. Specific questions to parents or caregivers on the visual behavior in dark or bright light can give a clue to the diagnosis. Some congenital retinal disorders, especially achromatopsia, cone–rod dystrophy, and Leber’s congenital amaurosis, may present with photophobia or day-blindness (see Chapter 44). Babies with CVI can show reluctance to look at a light, or, in contrast, will develop lightgazing1 (see Chapter 56). Lens (see Chapter 36) and corneal opacities (see Chapters 33 and 34), i.e. congenital glaucoma (see Chapter 37), albinism (see Chapter 40), and aniridia (see Chapter 38), can cause photophobia.
Are there any specific hand movements? Blind babies tend to press or poke their eyes (Fig. 91.2). Babies with limited vision due to retinal disorders may wave their hands between their eyes and a light source (Fig. 91.3).




