Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

12

Horizontal Strabismus
Horizontal strabismus forms the basis of strabismus in pediatric ophthalmology. The nuances of the condition are so subtle that the reader may need to read this chapter numerous times to understand it fully. The term strabismus has its origin in the Greek word strabismos, which means a squinting. Strabismus is defined as a misalignment of the visual axes and has a prevalence ranging from 1.31 to 7%.2 Strabismus may be subclassified in several ways with the most basic reflecting the direction of deviation: horizontal, vertical, or torsional. Horizontal strabismus may be divided into convergent (eso-) or divergent (exo-), with esodeviations being more common than exodeviations.3 The suffix phoria refers to a latent deviation whereby the deviation is controlled by fusion; under binocular viewing conditions, the eyes are aligned and only when fusion is disrupted is the deviation demonstrable. In contrast, the suffix tropia refers to a “manifest” deviation that is evident under binocular conditions and, presumably, beyond the control of fusion; the deviation is intermittent when it is controlled some of the time. All deviations occur on a spectrum related to fusional mechanisms and defined by control under binocular conditions and frequency, ranging from phoria to intermittent tropia to manifest deviation (tropia). Strabismus may also be classified as concomitant or incomitant. The term concomitant implies that the angle of deviation is the same in all fields of gaze; incomitant strabismus varies by the field of gaze and is usually associated with paralytic, restrictive, or special syndromes (i.e., Duane’s and Mobius’ syndromes).
 Esodeviations
Esodeviations
Esodeviations represent the most common type of strabismus and account for over 50% of ocular misalignment in childhood.4 Most esodeviations are manifest tropias. Esodeviations are broadly classified as infantile (congenital) or acquired (Table 12-1).
Pseudoesotropia
Often families are told that a “turn” will disappear or will be outgrown. This is incorrect. All children suspected of having a deviation must be examined. Many children aged less than 1 year have the optical illusion of crossing.
Pseudoesotropia refers to the appearance of esotropia when, in fact, the eyes are straight by cover test (see Chapter 11). These infants usually have prominent epicanthal folds and a broad flat nasal bridge; the epicanthal folds mask more of the sclera nasally and the appearance of crossing may be more evident in side gaze. Often the parents have an intermittent appearance of crossing When there is a history of crossing from the parents, it is important to ask if they think the child’s eyes are crossed at the time of the examination. Often the illusion created by the epicanthal folds “fools” the parents and primary care physicians. The ultimate determination of straight or crossed eyes is to use the Hirschberg (corneal light reflex test) or Krimsky (Hirschberg with prism) tests in conjunction with cover and alternate cover testing (see Chapter 11). Some children with pseudoesotropia may have an intermittent deviation or develop esotropia later; they should be monitored.
I. Infantile (congenital) A. Classic type B. Early onset with accommodative/refractive component C. Duane’s syndrome D. Abducens palsy E. Nystagmus blockage syndrome F. Mobius’ syndrome G. Ciancia syndrome II. Acquired A. Accommodative 1. Refractive 2. Nonrefractive 3. Combined B. Nonaccommodative 1. Cyclic 2. Idiopathic 3. Decompensated accommodative C. Sensory D. Divergence insufficiency E. Divergence paralysis F. Spasm of the near synkinetic reflex G. Medial rectus restriction H. Lateral rectus weakness |
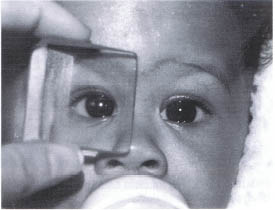
FIGURE 12-1. Baby with infantile esotropia. Angle of deviation is neutralized by prism.
Infantile (Congenital) Esotropia
The onset of infantile esotropia (Fig. 12-1) is by the age of 6 months and the incidence is probably less than 1%.1,2 Infantile esotropia is synonymous with congenital esotropia; the term congenital is inappropriate as the deviation is not present since birth. Large population studies have shown that the vast majority of neonates are either straight or exotropic and usually become aligned by 2 months of age.5,6 Although esotropia typically occurs in an otherwise healthy child, it is frequently associated with a positive family history. Developmental and motor delays such as cerebral palsy, Down syndrome (Fig. 12-2), and hydrocephalus often have an associated strabismus during infancy. There is no single gene inheritance pattern, but strabismus often clusters in families.7,8
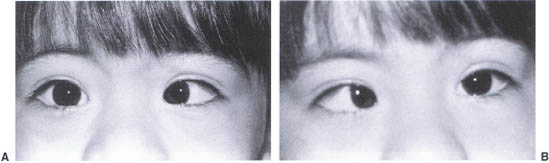
FIGURE 12-2. (A) Child with Down syndrome and esotropia: OD is fixating. (B) OS is fixating.
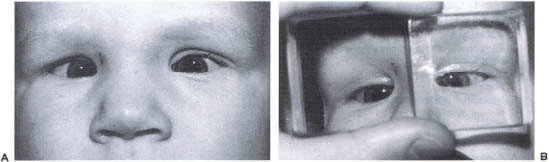
FIGURE 12-3. (A) Infantile esotrope exhibiting large angle of deviation. (B) Same child with prisms neutralizing angle of deviation.
Characteristic Features
The angle of deviation is usually very large, greater than 30 prism diopters (pd), and is approximately the same at distance and at near (Fig. 12-3). If the infant cross-fixates, he views targets by looking across his nose with the adducted eye toward the opposite field (Fig. 12-4).
Amblyopia
The equality of vision is of paramount importance and must be established before further treatment. However, the assessment of fixation preference in preverbal children is quite subjective, is difficult to establish, and requires judgment (see Chapter 2).
If there is a fixation preference, amblyopia treatment must be instituted. Generally, however, cross-fixators have equal vision because they use each eye half of the time. Patching is not usually necessary.
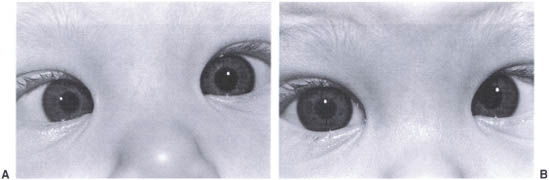
FIGURE 12-4. (A) Infantile exotrope who is cross-fixating. Note that the right eye is esotropic. (B) Left eye is now esotropic.
Deficient Abduction
As a result of cross-fixation, abduction may be difficult to demonstrate, and clinically the infant may appear to have bilateral sixth nerve palsies. Occlusion of one eye in the office for as little as 1 hour may demonstrate abduction. Other useful maneuvers include stimulating the vestibulocular reflex or performing a doll’s head maneuver. If these do not prove fruitful, patching at home for 1 to 2 days before the next visit will usually demonstrate abduction. A radiological scan should be obtained if abduction cannot be proven. Over time, abduction gradually improves so that by the age of 2 years the cross-fixator becomes a spontaneous alternator maintaining one eye straight at a time.
Refraction
Cycloplegic refraction usually reveals mild hyperopia of less than 2 diopters. Significant refractive errors should be optically corrected before surgery. Although preoperative glasses are usually not indicated, more than 50% of patients will need correction at some point after surgery.9 Although rare, accommodative esotropia may be evident as early as 4 months of age.10,11

FIGURE 12-5. (A) Child with inferior oblique overaction OS 1 +. (B) Inferior oblique overaction OS 2+.
Inferior Oblique Overaction
Over time, vertical deviations develop. Inferior oblique overaction (Fig. 12-5) is best identified by elevation in adduction; a vertical deviation in primary position is uncommon. The amount of overaction has been graded by the differences in elevation between the two eyes in upgaze and to the side; the scale ranges from 1 to 4+, with 4+ being the greatest. Inferior oblique overaction results in a “V pattern” esotropia, whereby the deviation decreases in upgaze secondary to the abducting effects of the inferior obliques. Significant inferior oblique overaction may be associated with superior oblique underaction.
Inferior oblique overaction often develops after the horizontal strabismus. Overall incidence ranges from 3613 to 78%,9 and the onset is usually after 1 year of age and most frequently between the ages of 2 and 4 years. Neither early surgical correction nor binocularity seems to change the rate of development of inferior oblique overaction.9,13,14 Inferior oblique overaction is most commonly associated with infantile esotropia but also can be seen with accommodative esotropes and intermittent exotropes.
Dissociated Vertical Deviation
Dissociated vertical deviation (DVD) is characterized by elevation, abduction, and excyclotorsion of the nonfixing eye without corresponding hypotropia of the contralateral eye; thus, DVD does not obey Hering’s law. On alternate cover test, the occluded eye will spontaneously “float up” and outward, and, when fixation recurs, there is no redress movement of the other eye. DVD is usually bilateral but asymmetrical; it is most noticeable in the nondominant eye during periods of visual inattentiveness. DVD usually is apparent by 18 months of age, although it may be seen as early as 8 months15; the prevalence seems to be unrelated to surgical alignment. It occurs most frequently with infantile esotropia.16,17 Stereopsis is generally poor, and the deviation is concomitant.17,18 The cause is not known but is believed to be central.19
DVD and inferior oblique overaction may occur simultaneously; differentiating between the two is clinically important and may be difficult. The deviation is greatest in adduction for overaction of the inferior oblique and concomitant for DVD. Another important distinguishing feature is the hypotropia of the nonfixing eye when the adducting eye of the overacting inferior oblique fixates; there is no corresponding hypotropia in DVD. Key differentiating features are summarized in Table 12-2.
Treatment
The goal in the management of infantile esotropia is ocular alignment with binocularity. However, affected children rarely achieve 40 seconds of stereoacuity regardless of the age of surgical alignment.20 Thus, the best outcome of treatment is the creation of a monofixation syndrome with alignment within 8 to 10 prism diopters of orthotropia.4,21,22 It is generally agreed that ocular alignment is rarely obtained without surgery. Prior to surgery, hyperopia greater than 2 diopters should be corrected; with higher amounts of hyperopia, some of the esotropia may be controlled with glasses. Amblyopia should be treated before surgery to optimize postoperative alignment and binocularity. The end point of patching should be spontaneous alternation or no fixation preference. Surgery should be performed for the residual esotropia.
| Features | Inferior Oblique Overaction | Dissociated Vertical Deviation |
|---|---|---|
| Elevation in adduction | X | X |
| Elevation in abduction and primary | X | |
| Concomitant deviation | X | |
| Associated V pattern | X | |
| Associated torsional movement | X | |
| Corresponding hypotropia of abducted eye | X | |
| Variable hyperdeviation | X |
Although the optimal timing of surgery remains controversial, evidence supports “early” surgery (before the age of 2 years).4,13,22–27 Historically, some surgeons prefer to wait until the age of 2 years so that they can better identify associated vertical deviations, diagnose and treat amblyopia, and obtain accurate distance measurements.20,28 The first choice of surgical methodology is usually bilateral medial rectus recession. If there is unilateral visual loss (more than two lines), surgery may be restricted to the nonfixing eye with a recession of the medial rectus and a resection of the lateral rectus.
Surgical correction is not a cosmetic procedure. The purpose is binocularity. In children with delayed motor development due to a central neurological process (e.g., prematurity, cerebral palsy, or nonspecific delayed maturation), postoperative alignment may aid their motor development.73
Final surgical alignment is assessed 6 weeks after surgery. A residual esotropia or exotropia of more than 15 diopters 6 weeks postoperatively warrants surgical reintervention. In the case of persistent esotropia, hyperopia (generally greater than 1.5 diopters) should be corrected. If the esotropia persists, repeat surgery should be undertaken. The same principles apply for persistent exotropia of more than 15 diopters; any myopia should be corrected. Surgical reintervention is warranted if the deviation persists.
As hyperopia increases during the first several years of life, cycloplegic refractions should be monitored.29,30 Recurrent esotropia usually responds well to correction of low levels of hyperopia. Hiles and colleagues9 reported that 65% of infantile esotropes that underwent surgery required hyperopic spectacles at some time postoperatively to control the deviation.
Accommodative Esotropia
The onset of accommodative esotropia is typically between the ages of 2 and 3 years; it has been described as occurring as early as 6 months and as late as 7 years of age.31 Affected children are presumed to have ocular alignment and some level of binocularity prior to the onset of the deviation. Amblyopia is more common in accommodative esotropia than in infantile esotropia. Accommodative esotropia is considered an “acquired” deviation. Acquired esotropia is a “daytime emergency” in visually immature children as suppression may develop rapidly; the onset is usually coincident with the child becoming more aware of the environment. The subset of children with an onset prior to 1 year of age is sometimes classified separately as early-onset accommodative esotropia; the infants tend to exhibit features of both the infantile and the accommodative forms.
Accommodative esotropia is caused by accommodative dysfunction and may be completely or partially controlled with spectacles. Accommodative esotropia is caused by significant hyperopia and/or a high accommodative convergence to accommodation ratio (AC/Aratio). Patients with a high AC/A ratio have a deviation that measures more at near than at distance, usually defined by 10 prism diopters or more. The AC/A ratio is defined as the amount of convergence in prism diopters per diopter change in accommodation; a normal ratio is 3. When the esotropia measures more at near than at distance by at least 10 prism diopters, this is a “clinical” (qualitative) AC/A ratio.
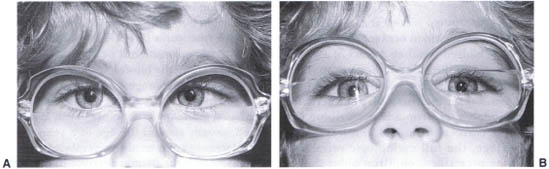
FIGURE 12-6. (A) Accommodative esotrope who is crossing at near. (B) Same child is straight with bifocals.
Accommodative Esotropia (Normal AC/A Ratio)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


