Dimmers looked into improving over Nussbaum’s design by incorporating a 0.1-mm-thick celluloid piece without any significant success due to infection and extrusion [3, 4].
No significant progress was made in the early first half of the 1900s until encouraging attempts of lamellar transplantation were reported by von Hippel. Later during World War II with the observations by Sir Harold Riley about the tolerance of polymethyl methacrylate (PMMA) [5] in pilots with ocular injuries, the development of the intraocular lens and a resurgence of interest in keratoprosthesis and new biocompatible materials began. With this discovery, a new era of different designs and material for keratoprosthesis began.
Initial work by Hernando Cardona in the early 1960s presented the perforating keratoprosthesis with an optical cylinder and an intralamellar skirt [6] (Fig. 2.2). The Cardona device was adopted and modified by several other surgeons adding their own innovations (Castroviejo, DeVoe, Choyce) [7, 8]. While some surgeons adopted the stem and skirt design, others preferred the collar button design [9, 10]. In the mid-1960s, Claes Dohlman introduced a modified collar button design with modified back portion as well as having the option of going through the lid in one of the designs [11, 12]. Lacombe also adopted a similar design and tested posterior fixation [13]. Dolhman’s collar button design underwent several modifications and is currently the preferred device with favorable long-term outcomes (Fig. 2.3). As designs continue to evolve, so did the technology and the materials available. Materials widely ranging from inorganic materials such as silicone, Teflon, and Dacron to biological materials such as sclera, cornea, hydroxyapatite, and tooth were tested [12].
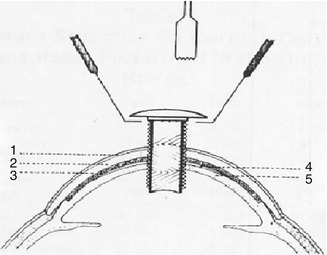
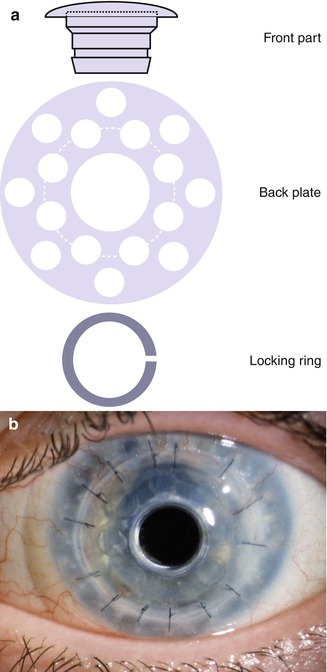
Fig. 2.2
Cardona keratoprosthesis. 1 Epithelium, 2 Fascia lata, 3 Dacron mesh, 4 Teflon skirt, 5 Recipient cornea (Refract Corneal Surg. 1991;7:470. Slack Inc.)
Fig. 2.3
Boston KPro Type I. (a) Three components: front part containing optics, back plate, and titanium locking ring. (b) Boston KPro Type I
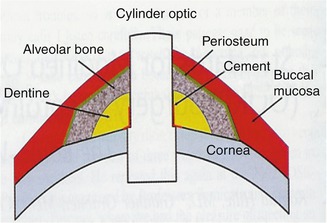
Efforts of biological substances, mainly tooth, were led by Strampelli in 1963 that gave birth to the osteo-odonto-keratoprosthesis showing improved outcomes in retention [12, 14–16] (Fig. 2.4).