History of Photocoagulation
Kenneth R. Jaegers
James F. Vander
The effect of solar light on the retina has been known for centuries. After observing burns of the retina caused by watching an eclipse, Socrates warned against the danger of viewing the sun during an eclipse and suggested instead viewing its reflection in water. The first description of a central scotoma following solar burn of the retina dates back to Theophilus Bonetus, who practiced in Geneva during the 17th century.1 The French painter Degas may have sustained a solar retinal burn because he dated his visual impairment from a sunny day when he stood guard duty near a moat during the Franco-Prussian War in the 1860s.
Although we now think that solar maculopathy probably results from a photochemical effect, not a thermal or photocoagulative effect, it was the observation of this phenomenon that inspired the earliest experimental research on fundus photocoagulation. Both Czerny in 1867 and Deutschmann in 1882 used a concave mirror and a convex lens to focus sunlight through dilated pupils onto the retina of rabbits. After a few seconds of exposure, grayish burns of various sizes developed that gradually turned into pigmented scars.2,3 Maggiore performed the first experimental photocoagulation of the human retina in 1927.4 He focused sunlight for 10 minutes into an eye that was to be enucleated because of a malignant tumor.
In 1945, several patients sought medical attention after viewing a solar eclipse. Meyer-Schwickerath, after observing macular damage in these patients, theorized that focused sunlight might be used intentionally to create a potentially therapeutic chorio-retinal lesion.5 Clinical experience led him to the carbon-arc lamp and, eventually, to the xenon-arc lamp.
The xenon-arc lamp, which became available commercially in 1958, produces an emission spectrum similar to that of sunlight, emitting all wavelengths between 400 and 1600 nm. Hence, it produces a full-thickness burn without selective tissue targeting. The xenon-arc lamp burns steadily, and no adjustments are necessary during treatment. These were advances over earlier sources. Over the years, xenon has proved to be an extremely useful light source and has promoted the clinical application of light coagulation as an accepted therapeutic tool. However, it has been superseded by the argon blue-green laser, argon green laser, krypton red laser, dye lasers and, more recently, the diode laser.
In 1960, Theodore Maiman used a ruby crystal in the first ophthalmic laser.6 Flocks and Zweng used this laser in their clinical investigations.7,8,9 Although the ruby laser produces a pure wavelength of 694 nm and is highly coherent, its red wavelength makes adequate treatment of retinal vascular abnormalities difficult. This difficulty was overcome with the introduction of the argon blue-green laser in 1968.10,11 These wavelengths are fairly well absorbed by hemoglobin and therefore permit direct closure of vascular anomalies. The advent of the argon green laser, with less xanthophyll absorption, made macular photocoagulation safer. These were followed by the development of the krypton red laser.12,13,14 The tunable organic dye laser, developed during the early 1980s, offers a continuous spectrum of wavelengths from 560 to 640 nm.15,16 The practical introduction of the semiconductor diode laser to the field of ophthalmology occurred in the late 1980s. This is a compact, portable laser with emissions in the near-infrared range with wavelengths between 805 and 810nm.
All these lasers produce a photocoagulative tissue effect by transforming light energy into thermal energy, which produces the desired tissue effect in the photocoagulated tissue or, sometimes, in neighboring tissues by thermal conduction. An alternative method of inducing a laser effect on ocular tissues uses ionizing photodisruption. This is the method used by the neodymium:yttrium-aluminum-garnet (Nd:YAG) laser, and it has its principal applications in treating the tissues of the anterior segment. The excimer laser is photoablative, making use of ultraviolet radiation to produce tissue disruption in the absence of a thermal effect.
PRINCIPLES OF RETINAL PHOTOCOAGULATION
Lasers are grouped according to their active medium, which can reside in solid, liquid, gaseous, or semiconductor states. Argon and krypton lasers are examples of gas-ion lasers in which the active medium is an ionized rare gas. The ruby and Nd:YAG lasers are solid-state lasers. Semiconductor crystals of gallium arsenide (GaAs) or indium phosphide comprise the active media of diode lasers.
Although the technical aspects concerning the production of a laser beam depend on the type of laser being considered, the instruments routinely used in the treatment of retinal disorders all produce a collimated beam of monochromatic light that creates a specific tissue reaction in the photocoagulated retina or choroid. Light energy is absorbed to a variable degree, depending on its wavelength, by the pigments found in the fundus. These are melanin, hemoglobin, and macular xanthophyll. Intensity of any given photocoagulation burn is directly proportional to the duration and magnitude of the temperature increase.
Melanin, found in the retinal pigment epithelium (RPE) and the choroid, absorbs light best. Hemoglobin absorbs yellow, blue, and green wavelengths well. Red and infrared, however, are absorbed poorly. Xanthophyll is located primarily in the macula and resides largely in the inner and outer plexiform layers of the neurosensory retina. Blue light is well absorbed, whereas green, yellow, and red wavelengths are poorly absorbed. Some clinical implications of these findings include decreased absorption and therefore the need for increased power in lightly pigmented fundi, the advantage of krypton red and diode lasers in the presence of vitreous hemorrhage and cataract, and the contraindicated use of blue or argon blue-green laser when treating macular disorders.
The histopathologic characteristics after fundus photocoagulation have been studied extensively. Geeraets and colleagues and then Curtin and Norton showed that high-intensity light energy produces tissue damage involving all layers of the choroid, RPE, and sensory retina, whereas very low energy light intensity involves primarily the pigment epithelium and photoreceptor elements with sparing of the inner retinal layers.17,18 Zweng and different groups of coworkers in several studies noted that ruby laser photocoagulation burns cause early adhesion of the sensory retina to the pigment epithelium and choroid.7,8,9 In addition, after mild burns, they detected marked destruction and clumping of RPE and marked disruption of the outer half of the sensory retina. The histopathologic effects of argon, krypton and tunable dye lasers have been shown to vary depending to a large extent on the intensity of the burn created.19,20 In general, with longer wavelengths, deeper choroidal penetration and greater sparing of the inner retinal layers are achieved.
VARIABLES OF LASER TREATMENT
DELIVERY SYSTEMS AND INSTRUMENT SETTINGS
After the decision has been made in favor of laser treatment, the ophthalmologist is faced with multiple options including which type of laser to use, how to deliver the laser treatment, and which settings to employ. At present, there are three main delivery systems from which to choose: the slit-lamp biomicroscope, the laser indirect ophthalmoscope (LIO), and the endolaser probe.
The slit-lamp remains the delivery method of choice for most cases, especially those requiring precise laser burn application such as macular photocoagulation. If a slit-lamp system is selected, a contact lens is used. The specific lens chosen depends on the location of the treatment area within the fundus and the surgeon’s preference. For panretinal photocoagulation (PRP), the wide-field view provided by a panfunduscopic lens is often helpful. The laser spot size produced with this lens is significantly magnified compared with a more traditional contact lens.
The LIO facilitates peripheral retinal photocoagulation and allows for treatment of patients who previously could not be treated with a slit-lamp system (e.g., pediatric or mentally retarded patients). It can be used to treat with argon, krypton, or diode systems. Using the LIO has become increasingly popular since its introduction in 1981.21 Coupled with the diode laser’s portability and studies demonstrating its effectiveness,22 the LIO has largely replaced cryotherapy in the treatment of retinopathy of prematurity.
Laser treatment may also be delivered during vitrectomy surgery using endolaser probes. Newer probes combine laser capability with illumination alone or combined with aspiration functions.
After the type of delivery system has been chosen, variables such as the wavelength, power, spot size, and duration must be considered. The wavelength used is determined primarily by the disease being treated, although for many conditions more than one type of laser may be appropriate. In the past, the argon laser was a blue-green laser. Blue light, however, is scattered by cataractous lenses and absorbed by macular xanthophyll, characteristics that make it an undesirable choice for photocoagulation. Hence, the advent of the argon green laser that emits light that is well absorbed by melanin and hemoglobin but poorly absorbed by macular xanthophyll. Longer wavelengths such as krypton red or diode penetrate deeper into the choroid than green lasers and may therefore be more painful. However, these wavelengths are poorly absorbed by hemoglobin and are more effective in the presence of vitreous hemorrhage. These lasers are also better able to penetrate cataractous lenses.
Other parameters to be considered include the laser power, duration of each exposure, and the spot size. These are interrelated variables that are adjusted during treatment by the ophthalmologist when necessary. Settings depend on the condition being treated, the clarity of the media, and the background pigmentation of the fundus.
In general, topical anesthesia is adequate for most laser treatments. Periocular anesthetic injection may be necessary in cases in which extensive PRP is planned, in particularly sensitive patients, or in cases in which absolute akinesia is necessary, such as with juxtafoveal lesions.
TREATMENT OF RETINAL VASCULAR DISEASES
DIABETIC RETINOPATHY
Diabetic retinopathy is the leading cause of blindness in people 20 to 55 years of age. The most common cause of decreased vision in patients with diabetes is macular edema. Over the past 2 decades, multicenter randomized clinical trials evaluating laser treatment in the setting of diabetic retinopathy have been undertaken. These trials and the practical application of their recommendations are discussed in this chapter.
In 1976, the National Eye Institute completed the Diabetic Retinopathy Study (DRS), a collaborative study to evaluate the effectiveness of scatter PRP for proliferative diabetic retinopathy (PDR).23 More than 1700 patients with advanced retinopathy were enrolled in the study. One eye was arbitrarily assigned to treatment using either xenon arc or argon laser photocoagulation while the other eye was observed. This study showed that both argon and xenon scatter photocoagulation reduced the risk of severe vision loss by 50%.24,25 In this study, “severe vision loss” was defined as visual acuity worse than 5/200 at two consecutive follow-up visits 4 months apart. Because of fewer harmful side effects compared with those associated with xenon, argon is the preferred treatment modality.
In the DRS, certain high-risk characteristics (HRCs) were identified as being the most accurate prognostic indicators of visual loss. HRCs include neovascularization on or within one disc diameter of the disc (NVD) that is equal to or greater than one fourth to one third of the disc area in extent or any NVD or retinal neovascularization else-where (NVE) associated with preretinal or vitreoushemorrhage (Fig. 1B). For eyes with these clinicalcharacteristics, prompt PRP is recommended. Forpatients with severe or severe nonproliferativediabetic retinopathy (NPDR), as well as for patientsin whom adequate follow-up cannot be ensured, early scatter therapy may be considered.26 The presence of rubeosis iridis or neovascular glaucoma in the setting of PDR, even without HRCs, may warrant PRP.27,28,29
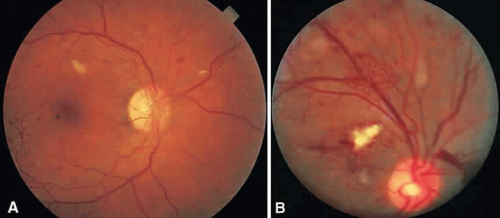 Fig. 1. A. Florid neovascularization of the disc. Any such neovascularization that covers more than one fourth of the disc area meets high-risk characteristics and warrants prompt panretinal photocoagulation. B. Neovascularization elsewhere and preretinal hemorrhage. Panretinal photocoagulation is indicated. |
The precise mechanism of formation of neovascular tissue remains uncertain, as does the mechanism by which PRP induces regression of this tissue. Traditionally, new vessel formation was thought to be a response to a possible angiogenic factor that may be produced by zones of ischemic retina.30 Destruction of these zones by PRP might then eliminate the source of this angiogenic stimulus. Although this approach may not accurately reflect the true pathophysiology involved, it does serve as a helpful model for understanding the proper methods of treatment for this condition. These concepts apply to other proliferative retinopathies as well including central retinal vein occlusion, branch retinal vein occlusion, SC sickle disease, sickle thalassemia, retinopathy of prematurity, Eales’ disease, dominant familial exudative retinopathy, and X-linked dominant incontinentia pigmenti. Of note, pregnancy can exacerbate and accelerate all aspects of diabetic retinopathy. It is unusual for pregnant patients without retinopathy at the onset of pregnancy to pro-gress to PDR during their pregnancy. However, patients with preexisting PDR are at greatest risk of visual loss and need to be observed closely and treated aggressively.
Methods
To complete scatter treatment, burns should be applied to the retina beginning at points on an oval defined as two disc diameters above, below, and temporal to the center of the macula, and one disc diameter nasal to the disc, and should extend peripherally at least to the equator (Fig. 2). This approach may help avoid inadvertent macular burns. A report by Blankenship suggests that sparing of the posterior aspect of the fundus may be possible without diminishing the beneficial effects of treatment.31 With the Goldmann lens, a 500-μm spot size is used, whereas with the panfunduscopic lens, a 200-μm spot is used. When vitreous hemorrhage is present, it may be necessary to reduce the size of the spot to 200 μm or to use a krypton or diode laser rather than an argon laser. The Krypton Argon Regression of Neovascularization Study found that krypton and argon were equally effective in inducing regression of NVD.32
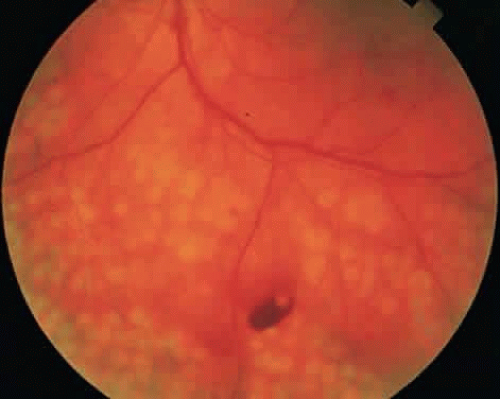 Fig. 2. Panretinal photocoagulation. Initial burns surround the disc and macula to outline the most posterior extent of intended treatment. Subsequent treatment is placed only peripheral to this ring, thereby reducing the risk of inadvertent macular photocoagulation. |
Care should be taken to avoid hitting any visible retinal vessels. The power setting should be such that a moderate white retinal coagulation is apparent. The power setting required to achieve this endpoint is recorded for future reference and is defined as the baseline power setting for the treatment session. It frequently needs to be higher for a panfunduscopic lens than for a three-mirror lens.
In general, application should be scattered uniformly, with the distance between burns being one burn diameter. It may be wise to treat inferiorly during the first session because vitreous hemorrhage, should it occur, tends to settle inferiorly. To minimize impairment of the temporal visual field, burns within four to five disc diameters of the disc on the nasal side should be arranged in rows parallel to the nerve fibers. Exposure time should be set at 0.1 or 0.05 second. In general, at least 1600 to 1800 burns should be applied. We usually treat over multiple sessions.
Occasionally PRP fails to induce regression of neovascularization and vision decreases. This can be a result of increased macular edema, focal bleeding from persistent neovascular fronds, retinal detachment, or neovascular glaucoma. Regression of HRCs occurs in 70% of cases within 3 weeks of treatment.33 Not surprisingly, patients who demonstrate a favorable early objective response to laser therapy have a significantly better visual prognosis than those who do not.34 In the case of increasing NVD or persistent NVD with bleeding, supplemen-tal treatment may be helpful. Peripheral retinal cryo-ablation may also be effective in causing regression of NVD or NVE. Cryotherapy is especially helpful in the setting of significant media opacities. About six applications are necessary in each quadrant. If vitreous hemorrhage has occurred and appears to be nonclearing, vitrectomy surgery may be indicated.
DIABETIC MACULAR EDEMA
Diabetic macular edema (DME) is a clinical diagnosis made with the slit-lamp biomicroscope. Intraretinal thickening is divided into focal and diffuse forms. Focal retinal edema is usually caused by specific leaking microaneurysms visible as pinpoint areas of leakage on fluorescein angiography (FA). The diffuse form of macular edema, conversely, usually represents a more widespread disruption of the inner blood-retina barrier. FA typically depicts large areas of leakage. It is important to remember that leakage of dye on FA does not always mean intraretinal thickening is present. Diagnosis of macular edema is based on the clinical examination of the retina.
The Early Treatment of Diabetic Retinopathy Study (ETDRS) was a multicenter, randomized, prospective clinical trial designed to address three main questions: Is laser photocoagulation effective in the treatment of DME? When in the course of diabetic retinopathy is it most effective to initiate PRP? Is aspirin effective in altering the course of diabetic retinopathy? The ETDRS demonstrated that laser photocoagulation for macular edema decreased the risk of moderate visual loss (defined as a doubling of the visual angle) by more than 50% especially in eyes with patterns of macular edema now known as clinically significant macular edema (CSME).35 Focal treatment also increased the chance of moderate visual gain.
CSME was defined as retinal thickening within 500 μm of the center of the macula, intraretinal hard exudate within 500 μm of the center of the macula associated with adjacent retinal thickening, or retinal thickening greater than one disc area any part of which is within one disc diameter of the center of the macula (Fig. 3A). The beneficial effects of treatment demonstrated in this trial suggest that all eyes with CSME should be considered for focal photocoagulation (see Fig. 3B). Visual acuity was not a factor in determining the presence or absence of CSME and some eyes in the treated group had20/20 visual acuity. Many retinal specialists, how-ever, defer treatment in asymptomatic patients with20/20 visual acuity except when hard exudate is encroaching on the fovea.
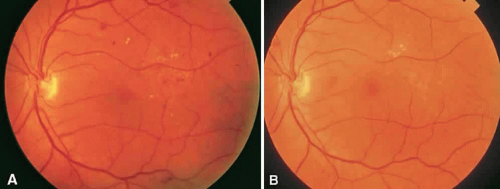 Fig. 3. A. Microaneurysms, hard exudate, and clinically significant macular edema temporal to the fovea. B. Three years after laser photocoagulation, the edema has resolved and the laser burns are barely visible. |
When CSME is present, fluorescein angiography is helpful in ruling out macular ischemia as a cause for decreased vision. If significant perifoveal capillary nonperfusion is present, then macular photocoagulation is associated with a higher risk of producing an immediate and permanent reduction in visual acuity. If photocoagulation is performed in such cases, care should be taken to avoid directly treating the few remaining perifoveal capillaries.
Methods
Various treatment strategies have been devised for photocoagulation of DME. Although the optimal method remains uncertain, most adhere to the basic principles described in the ETDRS. The argon green laser is widely used, although evidence now suggests that other wavelengths, such as dye yellow and orange, krypton red, and the diode, are comparable.36,37,38,39 A pretreatment fluorescein angiogram is generally used during photocoagulation to identify treatable lesions. Focal laser treatment involves direct laser treatment to all leaking microaneurysms.
When directly treating a microaneurysm, a 50- or 100-μm burn with 0.1-second duration is used, and one usually attempts to induce a slight change in the color of the lesion. Use of the 50-μm spot size may be associated with a higher risk of rupturing Bruch’s membrane and resultant choroidal neovascularization (CNV), so very low energy levels should be used initially.40 Initial treatment is directed at lesions located within two disc diameters of the center of the macula, but not closer than500 μm from its center. However, if vision is lessthan 20/40 and follow-up examination reveals persistent CSME, additional treatment of lesions up to 300 μm from the center is recommended.
Areas of diffuse leakage or nonperfusion within two disc diameters of the center of the macula are treated with a grid pattern. Diode laser has been shown to be as effective as argon laser in the treatment of diffuse DME.41 The goal of treatment in such cases is to produce a burn of light to moderate intensity. A 100- to 200-μm spot size is used, and burns are typically spaced one burn-width apart. Burns may be placed in the papillomacular bundle but, again, not closer than 500 μm from the center of the macula at the first treatment. For patients with a combination of focal and diffuse edema, a modified grid technique may be employed.42
In addition to the development of CNV mentioned earlier, other complications can occur after focal macular photocoagulation. Permanent visual loss may ensue after treatment. Causes includehemorrhage, perifoveal capillary occlusion, enlargement of photocoagulation scars to involve the fovea, marked lipid exudation as edema resolves, or in-advertent foveal burns. Paracentral scotomataare a frequent side effect, especially after heavy treatment.
Some patients present with CSME in the presence of PDR with HRC. Because PRP can exacerbate preexisting macular edema, it is generally advisable to initiate focal or grid treatment prior to or along with PRP. Performing nasal PRP first and completing the PRP is additional sessions may help prevent a worsening of the macular edema.
Regarding the use of aspirin, the ETDRS found that aspirin use did not affect the progression of retinopathy. Aspirin did not increase the risk for vitreous hemorrhage, the duration of or severity of vitreous hemorrhage, nor the rate of pars plana vitrectomy. Visual outcomes were not affected by aspirin use.43 Therefore, there is no ocular contradiction to the use of aspirin in patients with diabetic retinopathy.
RETINAL VENOUS OCCLUSIONS
BRANCH RETINAL VEIN OCCLUSION
Branch retinal vein occlusions (BRVOs) usually occur at arteriovenous crossings, with the arteriole typically crossing anterior to the vein.44 Visual loss may be a result of macular hemorrhage or edema, capillary nonperfusion, RPE changes or vitreous hemorrhage (Fig. 4). The Branch Vein Occlusion Study (BVOS) was a prospective, randomized multicenter clinical trial designed to address the following questions: Is macular argon laser photocoagulation beneficial in preserving or improving central visual acuity in eyes with 20/40 or worse vision secondary to macular edema related to a branch vein occlusion? Can peripheral scatter argon laser photocoagulation prevent the development of retinal neovascularization? Can peripheral scatter laser treatment prevent vitreous hemorrhage from retinal neovascularization? This study demonstrated conclusively the effectiveness of argon laser photocoagulation for the treatment of macular edema and retinal neovascularization (Fig. 5).45,46 After 3 years of follow-up, the gain of at least two lines of visual acuity from baseline maintained for two consecutive visits was significantly greater in treated eyes. As a result, laser photocoagulation is now recommended for patients with macular edema from branch vein occlusion. In addition, Roseman and Olk have shown that krypton red is effective for treating macular edema and neovascularization from BRVO in eyes with cataracts, vitreous hemorrhage, or extensive intraretinal hemorrhage.47 Visual improvement, however, is unlikely in cases with marked capillary nonperfusion and severe visual loss.
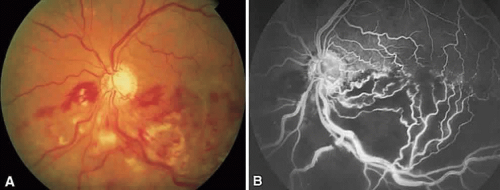 Fig. 4. A. Hemiretinal vein occlusion. B. Fluorescein angiogram reveals severe capillary nonperfusion. |
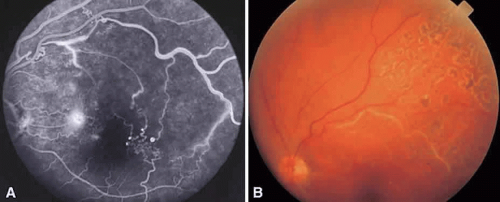 Fig. 5. A. Fluorescein angiogram of a superotemporal branch retinal vein occlusion with marked retinal ischemia. The localized hyperfluorescence in the papillomacular bundle represents retinal neovascularization. B. Three years after sector laser photocoagulation to area of retinal nonperfusion. |
If, after 3 months, visual acuity is 20/40 or worse, laser treatment is indicated. Grid treatment with a spot size of 100 to 200 μm and 0.1-second duration is placed in areas of leakage as shown on FA. There should be sufficient clearing of retinal hemorrhage before FA or laser because visual acuity may increase and FA may be more useful in terms of evaluating the macula for evidence of capillary nonperfusion. Recommendations concerning intensity of burns, spacing between laser burns, and treating near the fovea as well as potential complications are similar to those for laser treatment of DME. Eyes are reevaluated in 4 months and retreated if persistent macular edema accounts for the decrease in visual acuity.
The BVOS also assessed the role of scatter photocoagulation in preventing formation of retinal neovascularization and subsequent vitreous hemorrhage in patients with ischemic occlusions.47 It was noted that scatter argon laser photocoagulation to the affected segments, as determined by color photography and FA, extending no closer than two disc diameters to the center of the fovea, significantly decreased the risk of developing retinal neovascularization and lessened the occurrence of vitreous hemorrhage. Eyes at greatest risk for the development of retinal neovascularization were those with ischemic branch vein occlusions defined as eyes having more than five disc areas of capillary nonperfusion on FA. The risk of hemorrhage impairing vision in untreated patients is fairly low, however, and as a result no difference was found in terms of final visual acuity between treated and untreated groups. The study therefore recommends that scatter laser treatment be deferred until retinal neovascularization is present. The methods, as well as risks, of treatment are similar to those relating to PRP in patients with diabetes, except that treatment is limited to the affected area.
CENTRAL RETINAL VEIN OCCLUSION
Central retinal vein occlusions (CRVOs) are caused by thrombosis formation within the vein at the level of the lamina cribrosa. Clinical findings in the setting of a CRVO include intraretinal hemorrhages in all four quadrants, increased dilation and tortuosity of the retinal veins, macular edema, nerve fiber layer infarcts, and disc edema. Acutely, the decrease in visual acuity is secondary to macular changes such as macular edema, hemorrhage and capillary nonperfusion. Long-term visual loss may be secondary to macular capillary nonperfusion, chronic macular edema, arteriole occlusion, tractional or exudative retinal detachment and neovascular glaucoma.48,49 Anterior segment neovascularization is much more common with CRVOs than BRVOs.
CRVOs are usually described as “ischemic” or “nonischemic” based on clinical examination and FA findings (Fig. 6). Roughly 75% to 80% of CRVOs are nonischemic. However, up to 34% of these will progress to the ischemic type usually within 1 year.46,47,50,51 An eye with a nonischemic CRVO typically has minimal capillary nonperfusion on FA, relatively few intraretinal hemorrhages, and a better visual prognosis than the ischemic variety. Ischemic CRVOs, conversely, have widespread capillary nonperfusion and are associated with a worse visual prognosis with increased risk of rubeosis iridis and neovascular glaucoma.52
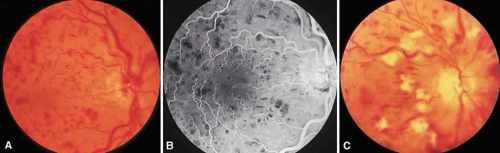 Fig. 6. Nonischemic (A and B) and ischemic (C) central retinal vein occlusion. |
The Central Vein Occlusion Study (CVOS) was a prospective, randomized, multicenter clinical trial designed to evaluate the role of PRP in promoting regression of anterior segment neovascularization resulting from ischemic CRVO, to determine the efficacy of macular grid laser photocoagulation for treating CRVO-related macular edema associated with visual acuity of 20/50 or worse, and to define the natural history of CRVO.53
The CVOS demonstrated that, although prophylactic PRP does decrease the risk of developing anterior segment neovascularization, prompt regression of neovascularization was more likely in eyes that had not received prior laser photocoagulation.54 Therefore, the study recommends observing ischemic CRVOs closely and treating with PRP at the first sign of iris or angle neovascularization rather than treating prophylactically. PRP may be warranted in the setting of acute ischemic CRVO if there is a high likelihood of poor patient compliance with follow-up. Unlike the BVOS, the CVOS did not demonstrate any benefit to laser photocoagulation for macular edema.55 Although laser therapy did decrease the amount of leakage on FA, there was no difference in visual acuity between treated and untreated eyes at any point in follow-up.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


