Purpose
To examine histomorphometrically the parapapillary region in highly myopic eyes.
Design
Retrospective laboratory investigation.
Methods
We examined a highly myopic glaucomatous group (36 human globes; axial length >26.5 mm) and a non–highly myopic group (28 globes with secondary angle-closure glaucoma; 17 eyes with malignant choroidal melanoma). Using light microscopy, pupil-optic nerve sections were assessed.
Results
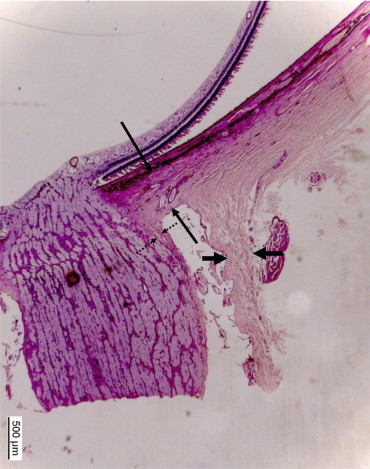
The length of the scleral flange (sclera between optic nerve border and optic nerve dura mater) increased with axial length ( P < .001; correlation coefficient r = 0.70) and decreased with its thickness ( P < .001; r = 0.75). In all highly myopic eyes (n = 15) with a distance of >0.5 mm between optic nerve border and beginning of Bruch membrane, the parapapillary region consisted of an elongated parapapillary scleral flange associated with a scleral flange thinning and a retrobulbar cerebrospinal fluid space extended into the retroparapapillary region. The parapapillary retina was composed of retinal nerve fiber layer (or its remnants) only, without elements of any other retinal layer, without underlying Bruch membrane or choroid. These histologic features were not detected in any of the non–highly myopic eyes.
Conclusions
Since parapapillary scleral thickness influences the lamina cribrosa biomechanics, the findings may partially explain the increased glaucoma susceptibility in highly myopic eyes. The implications of an absence of Bruch membrane and choroid in the highly myopic parapapillary region, and the implications of the retrobulbar parapapillary extension of the cerebrospinal spinal fluid space for the pathophysiology of the optic nerve head, have to be elucidated.
The optic nerve head shows a different appearance in highly myopic eyes than in non–highly myopic eyes. The features of highly myopic optic nerve heads include a secondary macrodisc with an abnormal, elongated disc shape; a shallow disc cupping; a decreased contrast between the color of the neuroretinal rim and the color of the optic cup; and a marked parapapillary atrophy, which is also called myopic crescent or “conus myopicus.” Additionally, recent population-based and hospital-based studies have shown an increased glaucoma prevalence, and presumably glaucoma susceptibility, in highly myopic eyes at a given intraocular pressure. In searching for anatomic reasons of the increased glaucoma susceptibility in highly myopic eyes, previous studies examined the intrapapillary region of highly myopic eyes and revealed a markedly thinner lamina cribrosa in addition to, and potentially attributable to, the enlargement of the optic nerve head in the highly myopic eyes. Since the parapapillary region is also of importance for the biomechanics of the optic nerve head in glaucoma, and since the parapapillary region in highly myopic eyes has not specifically been examined yet, we conducted the present investigation to histologically examine and compare the parapapillary region in highly myopic eyes and non–highly myopic human eyes.
Methods
The study included globes of white patients who had been enucleated because of painful absolute glaucoma or a malignant choroidal melanoma. In the glaucomatous group, vision was completely or almost completely lost. The whole study population was divided into globes with an axial length longer than 26.5 mm (highly myopic group) and globes with an axial length of equal to or less than 26.5 mm (non–highly myopic group). Enucleation became necessary usually because of intractable pain that could not be treated by medication. In the tumor group, the malignant choroidal melanomas did not infiltrate the trabecular meshwork, either directly or indirectly by migrating cells. The parapapillary region was free of tumor. Visual acuity depended on the degree of cataract, vitreous opacities, and foveal involvement by the tumor. At the time when the eyes were enucleated, other treatment modalities such as endoresection of the tumor or radiologic brachytherapy were not available or were thought not to be suitable for tumor removal with respect to its location and size.
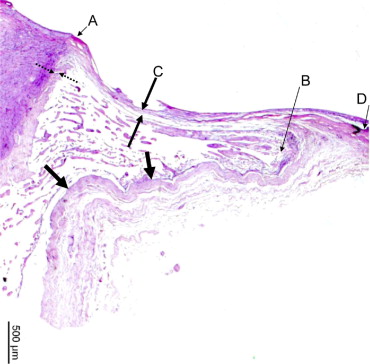
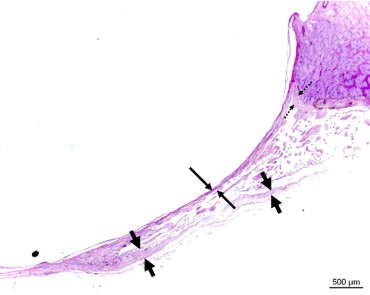
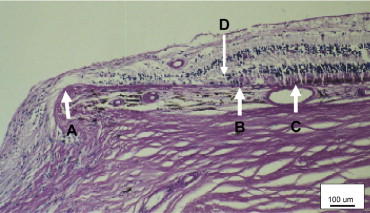
Immediately after enucleation, the globes were fixed in a solution of 4% formaldehyde and 1% glutaraldehyde and eventually processed for histologic sectioning. The preparation of the globes did not vary between the glaucomatous eyes and the nonglaucomatous eyes or between the highly myopic eyes and the non–highly myopic eyes. The globes were prepared in a routine manner for light microscopy. A pupil-optic nerve section was cut out of the fixed globes. The segments were dehydrated in alcohol, embedded in paraffin, sectioned for light microscopy, and stained by the periodic acid–Schiff method. For all eyes, 1 section running through the central part of the optic disc was selected for further evaluation. At the posterior pole of the globes, we assessed ( Figures 1−4 ): the length of the scleral flange (sclera between the border of the optic nerve [covered by pia mater] and the dura mater of the optic nerve); the thickness of the scleral flange; the distance between the outer margin of the optic nerve (covered by pia mater) and the beginning of the Bruch membrane; the distance between the outer margin of the optic nerve (covered by pia mater) and the beginning of the choriocapillaris; and the distance between the outer margin of the optic nerve (covered by pia mater) and the beginning of the retinal pigment epithelium lying on the Bruch membrane.
Statistical analysis was performed using a commercially available statistical software package (SPSS for Windows, version 17.0; SPSS Inc, Chicago, Illinois, USA). Means and standard deviations as well as medians and ranges are presented. For the comparison of the study groups, statistical tests for unpaired samples were applied. The level of significance was .05 (2-sided) in all statistical tests.
Results
The study included 36 human globes with an axial length longer than 26.5 mm (highly myopic group) that showed marked glaucomatous optic nerve damage, and 45 eyes with an axial length of equal to or less than 26.5 mm (non–highly myopic group). The non–highly myopic group included 28 globes that had been enucleated because of painful absolute secondary angle-closure glaucoma and 17 eyes that had been enucleated because of a malignant choroidal melanoma.
Within the non–highly myopic group, the length and thickness of the scleral flange and the distance between the optic nerve border and the beginning of Bruch membrane did not differ significantly between the glaucomatous subgroup and the nonglaucomatous subgroup ( Table ). The distances between the optic nerve border and the beginning of the choriocapillaris ( P = .02), the beginning of retinal photoreceptors on the Bruch membrane ( P = .008), and the beginning of the choriocapillaris beneath the Bruch membrane ( P = .003) were significantly longer in the glaucomatous group ( Table ). Comparing the highly myopic glaucomatous group with the glaucomatous non–highly myopic group showed significant differences for all parameters measured ( Table ). Including the whole study population into the statistical analysis correspondingly revealed significant differences for all parameters measured ( Table ).
| Glaucomatous Subgroup (Non–Highly Myopic) | Nonglaucomatous Subgroup (Non–Highly Myopic) | P -(1) Value a | Highly Myopic Group | P -(2) Value b | ANOVA | |
|---|---|---|---|---|---|---|
| n | 27 | 17 | 36 | |||
| Scleral flange length (mm) | 0.35 ± 0.17 (0.05, 0.81) | 0.35 ± 0.12 (0.14, 0.52) | .89 | 1.12 ± 0.78 (0.17, 3.21) | <.001 | <0.001 |
| Scleral flange thickness (mm) | 0.38 ± 0.06 (0.26, 0.52) | 0.39 ± 0.06 (0.26, 0.48) | .53 | 0.30 ± 0.14 (0.07, 0.67) | .002 | 0.002 |
| Distance optic nerve border to: | ||||||
| Beginning of Bruch membrane (mm) | −0.25 ± 0.21 (−0.60, 0.12) | −0.31 ± 0.17 (−0.57, 0.00) | .44 | 0.69 ± 1.31 (−0.76, 4.76) | .001 | 0.001 |
| Beginning of choriocapillaris (mm) | −0.06 ± 0.21 (−0.43, 0.29) | −0.25 ± 0.16 (−0.52, 0.00) | .02 | 0.90 ± 1.48 (−0.67, 4.87) | .009 | 0.002 |
| Beginning of retinal pigment epithelium (mm) | 0.11 ± 0.47 (−0.33, 1.74) | −0.22 ± 0.18 (−0.52, 0.00) | .008 | 0.94 ± 1.34 (−0.81, 4.76) | .004 | 0.002 |
| Beginning of retinal photoreceptors (mm) | 0.24 ± 0.62 (−0.29, 2.38) | −0.21 ± 0.16 (−0.48, 0.00) | .003 | 1.06 ± 1.38 (−0.52, 4.76) | .009 | 0.003 |
a Statistical significance of the difference between the non–highly myopic glaucomatous group and the non–highly myopic nonglaucomatous group.
b Statistical significance of the difference between the highly myopic group and both non–highly myopic groups.
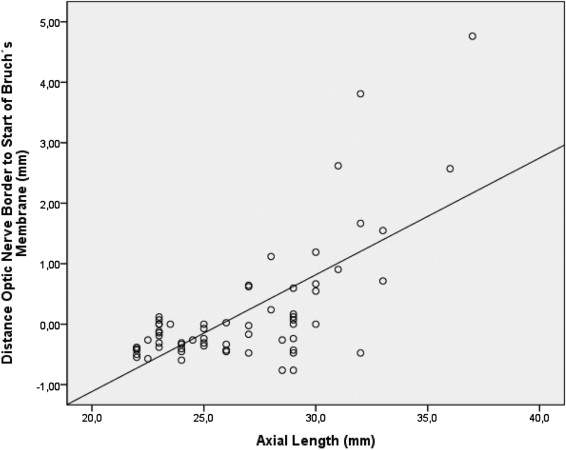
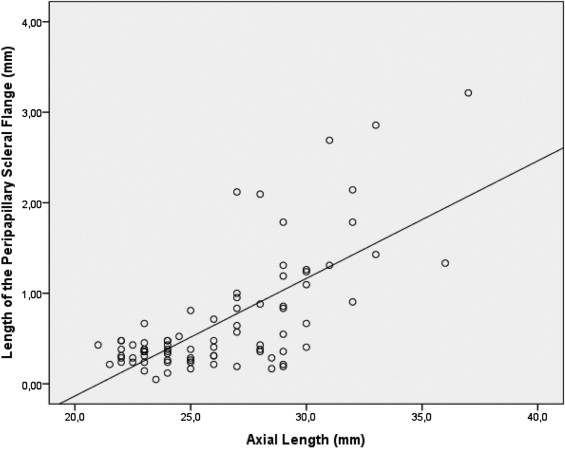
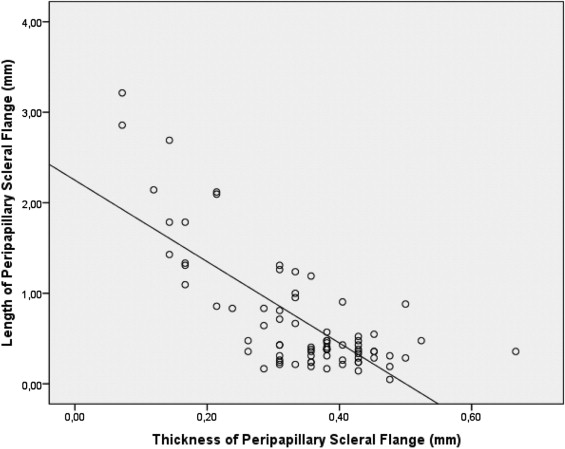
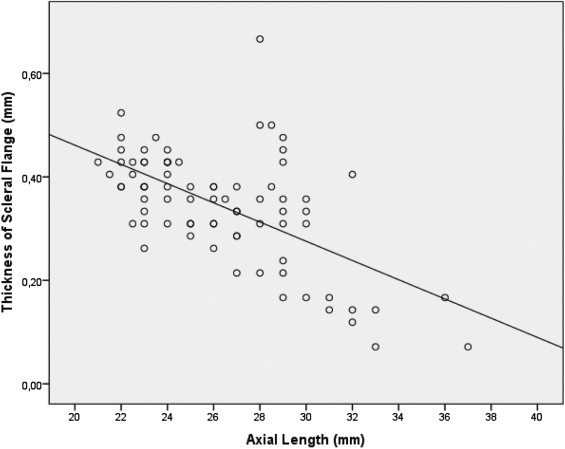
Taking all eyes together, the length of the scleral flange increased significantly with axial length ( P < .001; correlation coefficient r = 0.70) ( Figure 5 ) and decreased significantly with the thickness of the scleral flange ( P < .001) ( Figure 6 ). Consequently, the scleral flange thickness decreased with increasing axial length ( P < .001; r = 0.60) ( Figure 7 ). In a multivariate analysis, the length of the scleral flange was significantly associated with axial length ( P < .001) and scleral flange thickness ( P < .001); it was not associated with the presence of glaucoma ( P = .55).
The length of the scleral flange was significantly associated with the distance between the optic nerve border and the beginning of the Bruch membrane ( P < .001; r = 0.83), the beginning of the retinal pigment epithelium ( P < .001; r = 0.78), the beginning of the retinal photoreceptors ( P < .001; r = 0.75), and the beginning of the choriocapillaris ( P < .001; r = 0.90). Consequently, all these parameters were significantly associated with axial length (distance between the optic nerve border and beginning of Bruch membrane: P < .001; r = 0.69; Figure 8 ), the beginning of the retinal pigment epithelium ( P < .001; r = 0.62), the beginning of the retinal photoreceptors ( P < .001; r = 0.59), and the beginning of the choriocapillaris ( P < .001; r = 0.70).