(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
In 1980, I first described the clinical entity of hemicentral retinal vein occlusion (hemi-CRVO) and its pathogenesis, clinical features, and natural history [1]. Since then there have been several reports about this type of retinal vein occlusion, though most did not distinguish it from “retinal vein occlusion” in general. Before 1980 it was described simply as a “major branch retinal vein occlusion” which involved half of the retina, and usually called “hemispheric retinal vein occlusion.” In major branch retinal vein occlusion, the site of blockage is at the arteriovenous crossing but not so in hemi-CRVO, and its pathogenesis is very different from that of branch retinal vein occlusion. I have further investigated various aspects of this disease in different studies [2–10]. The following account is based on those studies and review of relevant studies in the literature.
Pathogenesis of Hemicentral Retinal Vein Occlusion
Hemi-CRVO is a variant of central retinal vein occlusion (CRVO). To understand that, one has to consider the development of the central retinal vein. Mann [11] has given a definitive account of this. The hyaloid artery enters the optic stalk at an early age and runs through it to reach the cavity of the optic cup. At first it has no accompanying vein. During the third month of intrauterine life, two venous channels, one on either side of the artery, can be recognized. These run in the optic nerve parallel to the artery and are united to each other by numerous anastomoses. As the two venous channels travel toward the ocular end of the optic nerve, they approach one another and finally coalesce at a variable distance behind the optic disc, forming the main trunk of the central retinal vein in the optic nerve. One of the two venous channels in the anterior part of the optic disc usually disappears before birth, leaving the central retinal vein as one trunk. However, in a certain proportion of cases, the embryonic pattern may persist. In my anatomical studies on the central retinal artery in man [12], in three of six eyes, histological serial sectioning and reconstruction demonstrated (quite incidentally) the existence of two venous channels, lying on either side of the central retinal artery (Fig. 25.1). The two venous trunks were seen in the optic nerve head and retrolaminar part of the nerve only, and then they joined to form the classic central retinal vein. The two venous trunks in the anterior part of the optic nerve were connected to one another by an anastomotic channel, as described by Mann [11] during fetal life. A schematic representation of the two intraneural trunks of the central retinal vein is shown in Fig. 25.2. The length of the intraneural part of these trunks can vary widely, as suggested by the three eyes with this anomaly in my study [12]. In my original study of 41 eyes with hemi-CRVO [1], the arrangement of retinal vessels on the optic disc provided additional evidence of such an anomaly. This is extremely variable; generally the two veins are from the upper and lower halves of the retina, but in some the two veins have a different distribution – one covering more than half of the retina and consequently the second one a much smaller area, as little as one quarter of the retina, so that in such an eye, the smaller vein looks like a “branch retinal vein.” In such a case, occlusion may involve only the smaller vein, and that would earlier have been diagnosed as “branch retinal vein occlusion.” Angiography is usually most helpful in defining the pattern of the superior and inferior retinal veins on the optic disc and their separate entry into the optic disc (see below). Chopdar [13] in a clinical study reported a 20.5 % incidence of dual trunks of the central retinal vein in humans.
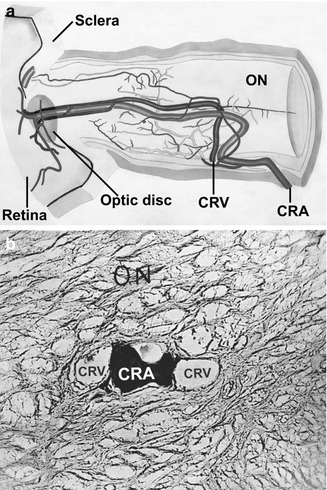
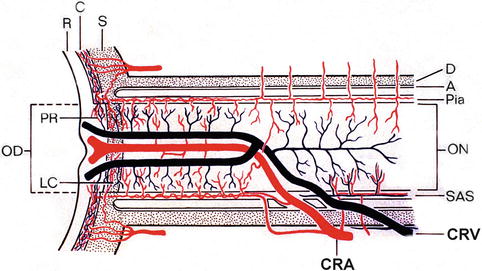
Fig. 25.1
Diagrammatic reconstruction from serial sections (10 μm thick) of the anterior part of the optic nerve. (a) It shows intraneural course of central retinal vessels. Note duplicate trunks of the central retinal vein anteriorly. (b) One of the transverse sections of the specimen shows, in the center of the optic nerve, two trunks of the central retinal vein on either side of the central retinal artery (filled with Prussian blue). CRA central retinal artery, CRV central retinal vein, ON optic nerve (Reproduced from Hayreh [12])
Fig. 25.2
Schematic representation of two trunks of the central retinal vein in the optic nerve. Abbreviations: A arachnoid, C choroid, CRA central artery of retina, CRV central retinal vein, D dural sheath, LC lamina cribrosa, OD optic disc, ON optic nerve, PR prelaminar region, SAS subarachnoid space, R retina, S sclera, P pia mater (Reproduced from Hayreh and Hayreh [1])
In eyes with two central retinal veins in the anterior part of the optic nerve, the superior vein drains the upper half of the retina and the inferior the lower half (Fig. 25.2). Venous occlusion can involve one of the two venous channels and consequently result in fundus changes in the corresponding half of the retina, and the pattern of such a venous occlusion is similar to that seen in CRVO and not the usual branch retinal vein occlusion. My clinical and experimental studies on CRVO (see Chap. 24) have shown that CRVO consists of two distinct clinical entities: nonischemic and ischemic. My studies on hemi-CRVO have also shown that it is also of nonischemic and ischemic types, as is evident from the discussion below.
Clinical Features
Demographic Characteristics
In my study [8] of 186 patients (190 eyes) with hemi-CRVO, there were 144 patients (147 eyes) with nonischemic hemi-CRVO and 42 patients (43 eyes) with ischemic hemi-CRVO. Table 25.1 summarizes their demographic characteristics.
Table 25.1
Demographic characteristics
Variable | Ischemic hemi-CRVO | Nonischemic hemi-CRVO |
|---|---|---|
n = 42 patients | n = 144 patients | |
(43 eyes) | (147 eyes) | |
Gender (male) | 28 (66.7 %) | 78 (54.2 %) |
Age | ||
Mean ± SD (range) | 69.1 ± 12.2 (38–87) | 67.2 ± 12.0 (36–90) |
Affected eye | ||
OD | 18 (42.9 %) | 64 (44.4 %) |
OS | 23 (54.8 %) | 77 (53.5 %) |
Both eyes | 1 (2.4 %) | 3 (2.0 %) |
Follow-up from onset (months) | ||
Median (25th–75th percentile) | 27.7 (9.6–45.7) | 30.5 (9.1–72.9) |
Diabetes | 9 (21.4 %) | 14 (9.7 %) |
Ischemic heart disease | 6 (14.3 %) | 16 (11.1 %) |
Stroke | 2 (4.8 %) | 7 (4.9 %) |
Hypertension | 27 (64.3 %) | 59 (41.0 %) |
Smoke (past or current) | (n = 36) | (n = 135) |
17 (47.2 %) | 48 (35.6 %) | |
POAG | (n = 39) | (n = 138) |
7 (18.0 %) | 26 (18.8 %) | |
OHT | (n = 39) | (n = 138) |
5 (12.8 %) | 13 (9.4 %) | |
Converted from nonischemic to ischemic | 3 eyes (6.9 %) | – |
Symptoms of Hemi-CRVO
The main symptom is blurred vision, which is either of sudden onset, usually noticed immediately on waking in the morning, or of gradual onset. As in CRVO, the vision in hemi-CRVO is frequently worse in the morning and improves to a variable extent later in the day. In my study 13 % of patients complained of a history of episode(s) of transient visual blurring from a few minutes to hours, before constant visual loss [10].
Area of the Retina Involved
This information was available in 177 hemi-CRVO eyes seen in my Ocular Vascular Clinic. Table 25.2 gives details. In some eyes, the occluded hemicentral retinal vein involved about two thirds to three quarters of the retina. In a few eyes the occluded hemicentral retinal vein involved only one sector of the retina. In some eyes with two hemicentral retinal veins, both the veins were occluded, as if their common parent trunk in the optic nerve was occluded. This shows that hemi-CRVO does not always involve only one half of the retina; there can be different patterns of retinal involvement, depending upon their area of retinal drainage.
Table 25.2
Area of the retina involved in hemi-CRVO
Area of the retina involved | Number of eyes |
|---|---|
Superior half | 37 % |
Superior half + inferior nasal sector | 4 % |
Superior half + inferior temporal sector | 2 % |
Inferior half | 41 % |
Inferior half + superior temporal sector | 2 % |
Inferior half + superior nasal sector | 1 % |
Superior temporal sector only | 3 % |
Superior nasal sector only | 1 % |
Inferior temporal sector only | 5 % |
The two hemicentral retinal veins were involved in the same eye | 3 % |
Total eyes | 177 |
Associated Systemic Disorders
I investigated this in 130 patients with hemi-CRVO (99 nonischemic and 31 ischemic hemi-CRVO). The findings of this study are discussed at length elsewhere [4]; the following are the salient findings: Table 25.3 gives the demographic characteristic of this group. Table 25.4 gives information on the prevalence of major systemic diseases (and selected subgroups), present before or at onset, of hemi-CRVO patients. A comparison of prevalence rates of various systemic diseases between the nonischemic and ischemic hemi-CRVO, after adjusting for age and gender in a logistic regression model, showed no significant difference except in chronic obstructive disease, which was more common in the ischemic than the nonischemic type (p = 0.055). Table 25.5 summarizes the prevalence of selected major categories of systemic conditions in hemi-CRVO and a comparison between the various retinal vein occlusion groups. No significant difference in prevalence rates was seen between CRVO (see Chap. 24) and hemi-CRVO; this is not surprising, because the two types are pathogenetically similar – that is, in CRVO the only trunk of the central retinal vein within the optic nerve is occluded, whereas, as discussed above, persons with hemi-CRVO have two trunks of central retinal vein within the optic nerve as a congenital abnormality and develop occlusion of only one of the two trunks. However, there was a significantly higher prevalence of arterial hypertension (p = 0.028) and smoking (past and current) (p = 0.010) in branch retinal vein occlusion than in hemi-CRVO. Comparison of ischemic versus nonischemic hemi-CRVO, however, showed no significant difference in systemic diseases between the two groups, which may be because the small sample size of ischemic hemi-CRVO masked any significant difference that may actually exist.
Table 25.3
Demographic characteristics for gender and age in hemi-CRVO
Age at onset | |||||||||
|---|---|---|---|---|---|---|---|---|---|
n | Gender | Descriptive statistics | Distribution by age (years) | ||||||
Male (%) | Female (%) | Mean (SD) | Median | Range | <45 | 45–64 | ≥65 | ||
Hemicentral RVO | 130 | 58 | 42 | 65.4 (13.9) | 68.1 | 14–98 | 12 % | 30 % | 58 % |
Nonischemic | 99 | 57 | 43 | 65.2 (12.9) | 68.3 | 32–87 | 12 % | 29 % | 59 % |
Ischemic | 31 | 61 | 39 | 65.9 (16.9) | 67.8 | 14–98 | 10 % | 32 % | 58 % |
Table 25.4
Major systemic diseases (and some selected subgroups) present before or at onset of HCRVO
Age groups (years) | ||||||||
|---|---|---|---|---|---|---|---|---|
<45 | 45–64 | >65 | Total | |||||
Nonischemic | Ischemic | Nonischemic | Ischemic | Nonischemic | Ischemic | Nonischemic | Ischemic | |
(n = 12) | (n = 3) | (n = 25) | (n = 11) | (n = 63) | (n = 17) | (n = 100) | (n = 31) | |
(%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) | |
Cardiovascular diseases: | ||||||||
Heart diseases | ||||||||
(a) Ischemic heart disease | 8.3 | 0 | 4.0 | 9.1 | 12.7 | 11.8 | 10.0 | 9.7 |
(b) Valvulara disease and atrial fibrillation or ventricular ectopy | 0 | 0 | 4.0 | 9.1 | 9.7 | 0 | 7.0 | 3.2 |
Arterial hypertension | 25.0 | 66.6 | 36.0 | 45.5 | 46.0 | 47.1 | 41.0 | 48.4 |
Endocrine diseases: | 0 | 0 | 4.0 | 0 | 11.1 | 35.3 | 8.0 | 19.4 |
Diabetes mellitus (DM): | 0 | 0 | 4.0 | 0 | 6.4 | 29.4 | 5.0 | 16.1 |
Adult onset | 0 | 0 | 4.0 | 0 | 6.4 | 29.4 | 5.0 | 16.1 |
Juvenile onset | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Thyroid disorders | 0 | 0 | 0 | 0 | 4.8 | 5.9 | 3.0 | 3.2 |
Hypertension + DM | 0 | 0 | 4.0 | 0 | 6.4 | 5.9 | 5.0 | 3.2 |
Cerebrovascular diseases | 0 | 0 | 0 | 0 | 4.8 | 5.9 | 3.0 | 3.2 |
Cerebrovascular disease | 0 | 0 | 0 | 0 | 3.2 | 5.9 | 2.0 | 3.2 |
Transient ischemic attack | 0 | 0 | 0 | 0 | 1.6 | 0 | 1.0 | 0 |
Amaurosis fugax | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Venous diseases | 0 | 0 | 0 | 0 | 1.6 | 11.8 | 1.0 | 6.5 |
Hypotensive episodes | 8.3 | 0 | 0 | 0 | 0 | 0 | 1.0 | 0 |
Pulmonary diseases: | 0 | 0 | 4.0 | 27.3 | 4.8 | 5.9 | 4.0 | 12.9 |
COPDb | 0 | 0 | 0 | 9.1 | 0 | 5.9 | 0 | 6.5 |
Hematologic diseases: | ||||||||
Anemia | 8.3 | 0 | 4.0 | 0 | 4.8 | 5.9 | 5.0 | 3.2 |
Gastrointestinal diseases: | 0 | 0 | 16.0 | 9.1 | 11.1 | 17.6 | 11.0 | 12.9 |
Ulcer | 0 | 0 | 16.0 | 0 | 4.8 | 5.9 | 7.0 | 3.2 |
GI bleed | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Renal diseases: | 0 | 0 | 4.0 | 9.1 | 3.2 | 5.9 | 3.0 | 6.5 |
Glomerulonephritis | 0 | 0 | 0 | 0 | 0 | 47.1 | 0 | 0 |
Chronic renal failure | 0 | 0 | 4.0 | 0 | 1.6 | 0 | 2.0 | 0 |
Diabetic nephropathy | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Renal transplant | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Dialysis | 0 | 0 | 0 | 0 | 1.6 | 0 | 1.0 | 0 |
Other | 0 | 0 | 0 | 9.1 | 1.6 | 5.9 | 1.0 | 6.5 |
Hyperlipidemia | 16.7 | 0 | 8.0 | 9.1 | 14.3 | 0 | 13.0 | 3.2 |
Rheumatologic conditions: | 8.3 | 0 | 4.0 | 18.2 | 9.5 | 11.8 | 8.0 | 12.9 |
Arthritis: | ||||||||
Rheumatoid | 8.3 | 0 | 0 | 0 | 0 | 0 | 1.0 | 0 |
Psoriatic | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Nonspecific | 0 | 0 | 0 | 9.1 | 0 | 0 | 0 | 3.2 |
Other | 0 | 0 | 0 | 0 | 1.6 | 0 | 1.0 | 0 |
Systemic lupus erythem. | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Gout | 0 | 0 | 4.0 | 9.1 | 4.8 | 5.9 | 4.0 | 6.5 |
Infections: | 0 | 0 | 8.0 | 0 | 4.8 | 11.8 | 5.0 | 6.5 |
Tuberculosis | 0 | 0 | 0 | 0 | 1.6 | 0 | 1.0 | 0 |
Syphilis | 0 | 0 | 8.0 | 0 | 3.2 | 0 | 4.0 | 0 |
Herpes zoster | 0 | 0 | 0 | 0 | 0 | 5.9 | 0 | 3.2 |
Sepsis | 0 | 0 | 0 | 0 | 1.6 | 0 | 1.0 | 0 |
Urinary tract infection | 0 | 0 | 4.0 | 0 | 1.6 | 0 | 2.0 | 0 |
Viral prodrome | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
URI/pneumonia | 0 | 0 | 0 | 0 | 0 | 5.9 | 0 | 3.2 |
Other | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Neurological diseases: | 8.3 | 0 | 4.0 | 0 | 3.2 | 5.9 | 4.0 | 3.2 |
Peripheral neuropathy | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Diabetic neuropathy | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Oncologic diseases: | 8.3 | 0 | 4.0 | 9.1 | 17.5 | 11.8 | 13.0 | 9.7 |
Colon | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Genitourinary tract | 0 | 0 | 4.0 | 9.1 | 3.2 | 0 | 3.0 | 3.2 |
Prostate | 0 | 0 | 0 | 0 | 1.6 | 5.9 | 1.0 | 3.2 |
Skin | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Breast | 0 | 0 | 0
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| |||||