(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
In my anatomical study of 106 human central retinal arteries (CRAOs) [1, 2], I found two specimens with two CRAs, each arising independently from the ophthalmic artery (Fig. 14.1). In one of these specimens, the two CRAs pierced the sheath of the optic nerve 12 mm and 5 mm behind the eyeball on its inferolateral aspect and then ran independently in the optic nerve up to the optic disc. At the optic disc, the two joined to form a loop, from the summit of which arose terminal branches which followed the usual course. In the second specimen, the two CRAs arose independently from the ophthalmic artery, and they united to form one trunk at the point of entry into the sheath of the optic nerve. As far as I know, there has not been any other report with anatomical proof of the presence of two CRAs in the same eye.
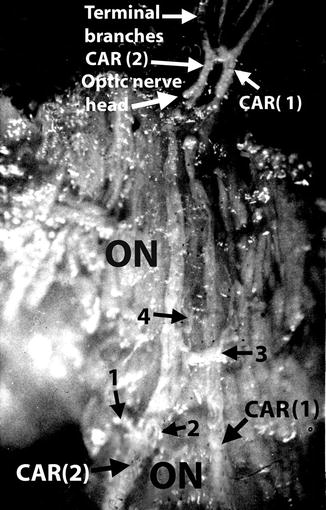
Fig. 14.1
Two central arteries of the retina, CAR (1) and (2), of independent origin. The intraneural course and termination of the two arteries are shown, as seen on splitting open the optic nerve and eyeball. Branches (1, 2, 3, 4) from the intraneural course of CAR (2) are also seen. CAR central artery of the retina, ON optic nerve (Reproduced from Hayreh [1])
Over the recent years several cases of the clinical entity “hemicentral retinal artery occlusion” (hemi-CRAO) have been described, where one half of the retina is involved by acute ischemia [3–11]. The reports were of only one case each, except Schmidt et al. [5], who had 29 patients, and Rishi et al. [8] who had 4.
The question arises: do these cases of “hemi-CRAO” represent the occlusion of one of two separate trunks arising from the ophthalmic artery, as seen in my anatomical study [1, 2], or is there another cause?
1.
There has been no clinically confirmed report where an eye having two CRAs developed occlusion of only one.
2.
Hemi-CRAO is more probably due to the occlusion of one of the two main divisions of the CRA at the optic disc as soon as it emerges from the optic nerve. When an embolus is seen in the optic disc in these cases, that is definite proof that there is simply occlusion of one of those two main divisions of the CRA on the optic disc; thus, it simply represents a variant of branch retinal arteriolar occlusion (BRAO). Most of the cases described seem to fall into this category. In my study [12] of 133 eyes with BRAO, this was the case in 20 % – involving the upper half of the retina in 11 % (Figs. 14.2 and 14.3) and lower half in 9 % (Figs. 14.4 and 14.5).
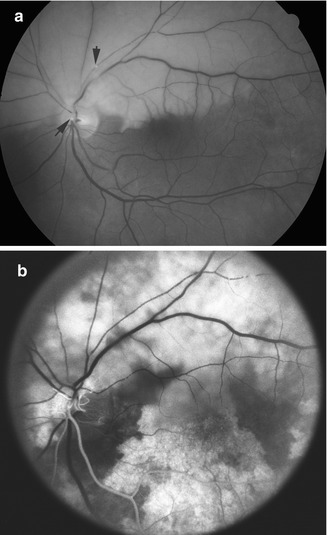
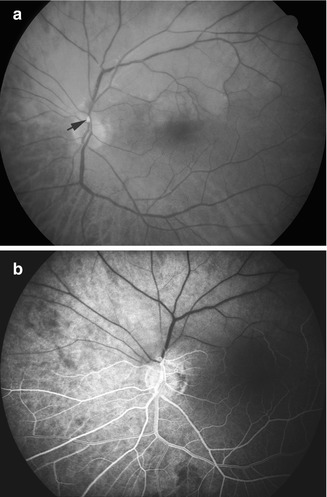
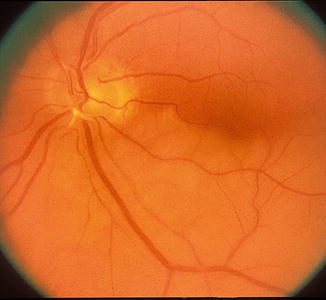
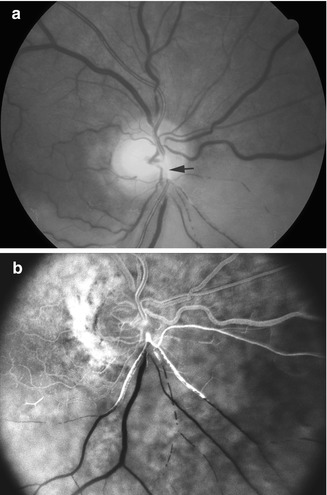
Fig. 14.2
(a) Fundus photograph of the left eye, on the day of onset of superior branch retinal artery occlusion, shows regional retinal infarct. There are two calcific emboli (arrows) – one blocking the superior division of the central retinal artery and the second small one in the superior temporal arteriole, with boxcarring of the blood column in that arteriole. (b) Fluorescein fundus angiogram, during the retinal arterial phase, shows no filling of the superior division of the central retinal artery and also absence of filling of the inferior temporal peripapillary choroid, indicating embolic occlusion of the choroidal arteries in that region as well
Fig. 14.3
(a) Fundus photograph of the left eye, 1 day after onset of superior BRAO, shows regional retinal infarct. A calcific embolus (arrow) is blocking the superior division of the central retinal artery. (b) Fluorescein fundus angiogram, during the retinal arteriovenous phase, shows no filling of the superior division of the central retinal artery
Fig. 14.4
Fundus photograph of the left eye, 1 day after onset of occlusion of the inferior division of the central retinal artery, with regional retinal infarct, and a platelet embolus at the site of occlusion (Reproduced from Hayreh [13])
Fig. 14.5
(a) Fundus photograph of the right eye, 1 day after occlusion of the inferior division of the central retinal artery by a large platelet embolus (arrow), shows retinal infarction and boxcarring of blood column in the involved retina. (b) Fluorescein fundus angiogram, during the late retinal arteriovenous phase, shows occlusion of the inferior division of the central retinal artery
3.
It is known that occasionally one large branch of the CRA in the optic nerve emerges at the optic disc as a separate artery, and that may be considered as representing two CRAs, as shown in one of the specimens in my anatomical study on the CRA [1, 2] (Fig. 14.6).
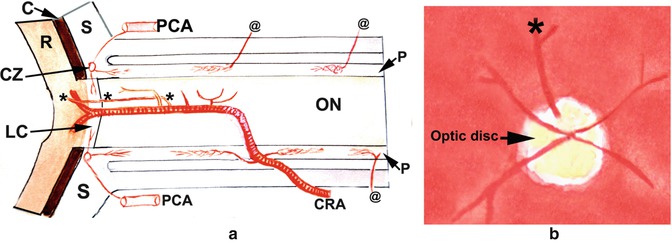
Fig. 14.6
Diagrammatic representation of an intraneural branch of the central retinal artery emerging at the optic disc to supply the superior part of the retina (indicated by asterisk) (Reproduced from Hayreh [1]). (a) Diagram showing the entire course of the central retinal artery and its branches from various parts. Intraneural branch indicated by asterisk emerges at the optic disc to supply the superior part, as shown in (b). C choroid, CRA central retinal artery, CZ circle of Haller and Zinn, LC lamina cribrosa, ON optic nerve, P pia mater, PCA posterior ciliary artery, R retina, S sclera, asterisk intraneural branch emerging at the optic disc and supplies the superior retina, @ pial arterial branches arising from the ophthalmic artery and its various branches
4.




Instead of dividing into its two branches at the optic disc, the CRA may do so in the optic nerve, before it emerges from the optic nerve. Rishi et al. [8] in their 4 cases on Color Doppler examination showed bifurcation of the CRA behind the lamina cribrosa.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
