OVERVIEW
- Hearing loss in children has a significant impact on quality of life
- Hearing loss in children can be conductive (most commonly glue ear), sensorineural (1 in 1000 at birth, many causes genetic/ syndromic), or mixed
- In the UK, newborn hearing screening is universal. Other hearing tests in children can be subjective or objective, depending on the child’s age
- Treatment of hearing loss in children can be non-surgical (e.g. provision of hearing aids) or surgical (e.g. grommet insertion, auditory implants)
- Cochlear implants have revolutionised the treatment of profound hearing loss in children
In children, the effects of hearing loss can be wide-ranging, affecting the development of spoken language and the quality of speech, as well as impacting on social interactions, educational achievement, behaviour, balance and safety.
Accurate diagnosis and treatment of hearing loss in children is therefore very important and relies upon close cooperation between health professionals, including audiologists, otolaryngologists, paediatricians, speech and language therapists, general practitioners, teachers (including teachers of the deaf) and health visitors.
Types of hearing loss
Hearing loss can be congenital (present at birth) or acquired (developing after birth). In either case, the hearing loss can be an isolated finding or can occur as a part of a wider neurological or developmental disorder or syndrome. Hearing loss can be conductive (related to a problem of the transmission of sound to the inner ear), sensorineural (related to a problem with the inner ear or auditory pathway) or mixed (components of both conductive and sensorineural hearing loss) (Figure 5.1). Common causes of conductive hearing loss in children are listed in Table 5.1.
Figure 5.1 Audiograms showing (a) conductive and (b) sensorineural hearing loss. Key: Right ear: o—air conduction, [—masked bone conduction. Left ear: x—air conduction, Δ—unmasked bone conduction.
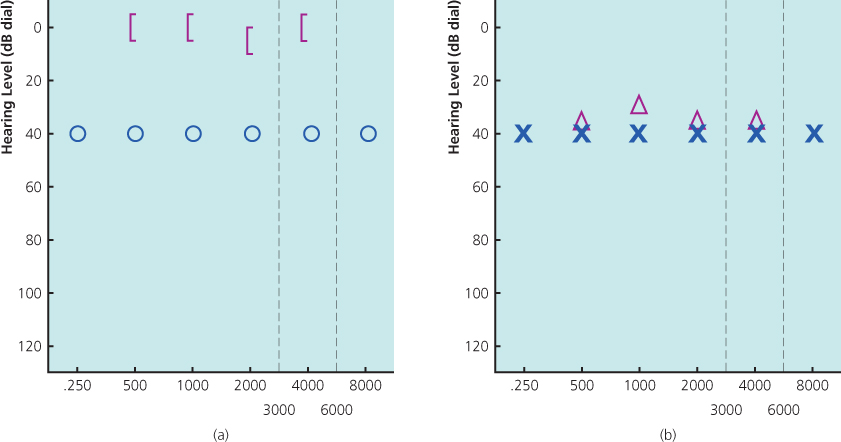
Table 5.1 Causes of conductive hearing loss in children, and risk factors.
| External ear | |
| Acquired obstruction | Wax impaction Foreign body |
| Congenital atresia | Treacher Collins syndrome Goldenhar syndrome Craniosynostoses |
| Middle ear | |
| Glue ear | Parental smoking, older siblings, day care Down syndrome Cleft palate |
| Ossicular abnormality | Treacher Collins syndrome Branchio-oto-renal syndrome CHARGE syndrome Trauma Cholesteatoma Tumours (rare) |
CHARGE: Coloboma, Heart defects, choanal Atresia, Retardation of growth, Genital defects, Ear abnormalities.
Assessment of a child with hearing loss
As with other conditions, the history is vital to the assessment of the child with suspected hearing loss. In particular, enquiry should be made about risk factors for both congenital and acquired hearing loss (Tables 5.1 and 5.2). Otoscopy is the mainstay of examination, and particularly helpful in diagnosing conductive hearing loss (see later).
Table 5.2 Risk factors for sensorineural hearing loss in infants.
| Prenatal | Family history Maternal alcohol/ drug use Infections (TORCHS) Ototoxic medications |
| Perinatal | Extreme prematurity Low birth weight Hypoxia Prolonged ventilation Sepsis |
| Postnatal | Infections Meningitis Other: CMV, measles, mumps Jaundice Ototoxic medications Head injury |
TORCHS: toxoplasmosis, rubella, cytomegalovirus, Herpes simplex, HIV, syphilis; CMV: cytomegalovirus.
Diagnosis of hearing loss in children
Newborn hearing screening
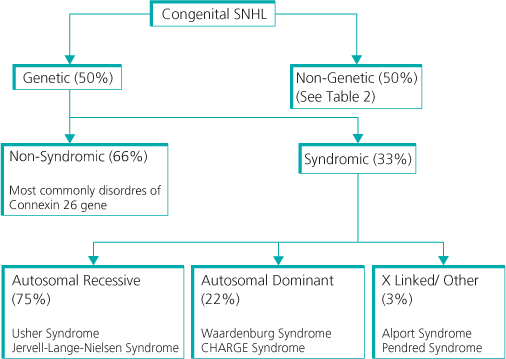
In the UK, approximately 1 in 1000 children is born with severe to profound permanent hearing loss. Half of these cases have a genetic cause, with one-third of these related to a recognised syndrome (Figure 5.2).
Applied universally since 2005, the Newborn Hearing Screening Programme (NHSP) now ensures that all newborn babies have a hearing assessment performed shortly after birth. Two techniques are used:
Otoacoustic emissions (OAEs): These are sounds generated by the outer hair cells of the cochlea in response to a sound and are measured by a sensitive microphone placed in the ear canal. The test is quick and easily performed by dedicated trained screeners (Figure 5.3).

Automated auditory brainstem response (AABR): In this test, surface electrodes measure the electrical activity of the brainstem in response to an auditory stimulus. These are more accurate but also take longer than OAEs. A general anaesthetic is not required but the child must be settled, e.g. asleep or feeding.
AABR is carried out in any child who fails the OAEs test on two occasions. In addition, any baby who required admission to the special care baby unit (SCBU) or neonatal intensive care unit (NICU) has both OAEs and AABR performed, as they frequently have risk factors for hearing loss (Table 5.2).
Any baby who fails the AABR twice is referred for further assessment and early intervention.
Continued vigilance is required to ensure that no child with significant hearing loss is missed. Further screening of children in school is targeted to detect those who were missed by the NHSP or developed a progressive hearing loss.
Hearing tests in children
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


