OVERVIEW
- In the UK, 6% of adults have significant hearing impairment
- Hearing impairment in adults usually occurs gradually
- Progressive loss of hearing, especially in one ear, may not be noticed by the patient
- The degree of disability depends upon the severity of the hearing loss and if it is bilateral
- Profound deafness, in one ear only, allows normal communication except when someone is speaking on that side
- A moderate bilateral high-frequency hearing impairment causes substantial problems in discriminating voices over a noisy environment
- Commonly the diagnosis can be established from a simple history and a few clinical findings: a clear view of the tympanic membranes and use of tuning fork tests
History
Important characteristics of hearing loss are whether the onset was gradual and over what time period, whether it fluctuates, whether it is in one or both ears and how it affects the patient’s quality of life. Associated symptoms might be tinnitus, dizziness or vertigo, ear ache and discharge from the ear.
Classification
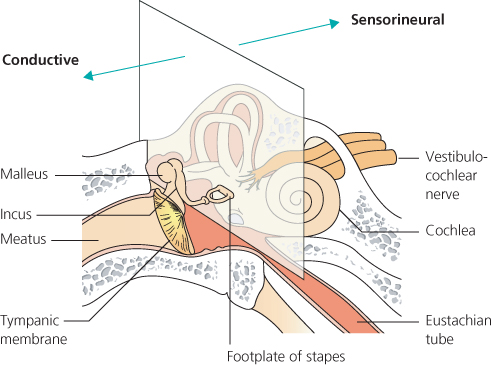
Hearing loss may be categorised as conductive or sensorineural based upon the anatomical location of the problem (Figure 4.1). In conductive deafness, there is obstruction to the passage of the sound waves at any point between the outer ear and the foot plate of the stapes in the middle ear. This is the path of sound waves through the eardrum and ossicles to the cochlea. In a normally hearing ear, vibrations of the footplate of the stapes are transduced into a travelling wave within the fluids and along the basilar membrane of the cochlea. Malfunction or disease within the cochlea or auditory nerve is termed sensorineural. In some conditions there may be a mixed hearing loss, a combination of both forms of deafness.
Conductive hearing causes
These are given in Box 4.1.
- Wax impaction
- Otitis media with effusion (OME)
- Eustachian tube dysfunction
- Ear infections
- Perforations of the tympanic membranes
- Chronic Suppurative Otitis Media
Wax impaction
This is probably the most common cause. Frequently the patient has used cotton buds and wax becomes more deeply impacted down the ear canal. The Weber test is referred to the blocked ear. Management entails removal of the wax, by syringing in general practice or by microsuction in a specialist clinic. The use of proprietary ear drops to soften wax for a few days beforehand is helpful. An eardrum which is known or suspected to be perforated or particularly weak should not be syringed.
Otitis externa
Inflammation of the external ear canal (otitis externa) may cause mild conductive hearing loss (Chapter 2).
Keratosis obturans
This is a condition in which there is an abnormality of normal migration of epithelium (skin) outwards along the ear canal resulting in an accumulation of desquamated keratin in the ear canal, causing blockage which needs treating by repeated microsuction and instrument clearance.
Acquired obliterative otitis externa
This follows prolonged and unsuccessful treatment of otitis externa; the ear canal scars and then the deep bony ear canal is blocked by fibrous tissue. The patient is left with a substantial conductive deafness, but a dry ear. Surgery to excise the scar and reopen and widen the meatus is possible but long-term results can be disappointing.
Tumours of the outer or middle ear
Tumours of the external or middle ear are uncommon but can present with conductive hearing loss. Any unusual looking area or non-healing ulcer of the meatal skin should be biopsied. Treatment is likely to be surgical, but malignant tumours may also require chemoradiation.
The most common middle ear neoplasm is a glomus tumour or paraganglioma. These vascular lesions present as a red swelling behind the tympanic membrane. Investigation entails specialist imaging to show the extent and probable nature of the lesion. Treatment is usually by surgical excision.
Otitis media with effusion (OME)
Persistent middle ear effusions can develop in adults with poorly functioning Eustachian tubes following upper respiratory tract infections, in the elderly, and in patients after radiotherapy to the head or skull base. Effusions are typically clear yellow. Conservative treatment includes broad-spectrum antibiotics, a short course of systemic steroids, or montelukast (leukotriene antagonist), and nasal decongestants together with attempted autoventilation of the middle ear by Valsalva manoeuvres. The nasopharynx must be examined endoscopically, to exclude Eustachian tube obstruction from a postnasal space lesion such as nasopharyngeal carcinoma. Non-resolving middle ear effusions can be treated surgically by insertion of ventilation tubes (grommets) in the eardrum.
Adhesive otitis media and retraction pockets
Chronic Eustachian tube dysfunction can lead to a thin (atelectatic) eardrum with retraction pockets. These may erode the ossicular chain causing hearing loss. Surgery can be helpful. Chronic inflammation of the middle ear cleft can leave a poorly aerated middle ear with scarring and adhesions (adhesive otitis media).
Myringosclerosis and tympanosclerosis
Any ear in which there has been previous infection or insertion of ventilation tubes can show white or yellow scarring within the tympanic membrane known as myringosclerosis or tympanosclerosis. It does not usually cause a significant reduction in hearing (Figure 4.2). Rarely tympanosclerosis within the middle ear cleft causes scarring and fixation of the ossicles, with a conductive hearing loss.
Figure 4.2 Right eardrum showing myringosclerosis anterior to handle of malleus and transparent atrophic regions.

Acute suppurative otitis media (ASOM) and chronic suppurative otitis media (CSOM)
Cases of ASOM (Chapter 2) and CSOM of either form (Chapter 3) are usually associated with conductive hearing loss. The severity will depend upon whether there is an aerated segment of middle ear and continuity of the ossicular chain. Sometimes a patient with cholesteatoma retains good hearing pre-operatively because the sound is transmitted through the cholesteatoma, after the incus has been eroded.
Surgical treatment of CSOM
Surgical treatment of CSOM is covered in Chapter 3. Among its sequelae, persistent central perforations of the tympanic membrane (Figure 4.3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


