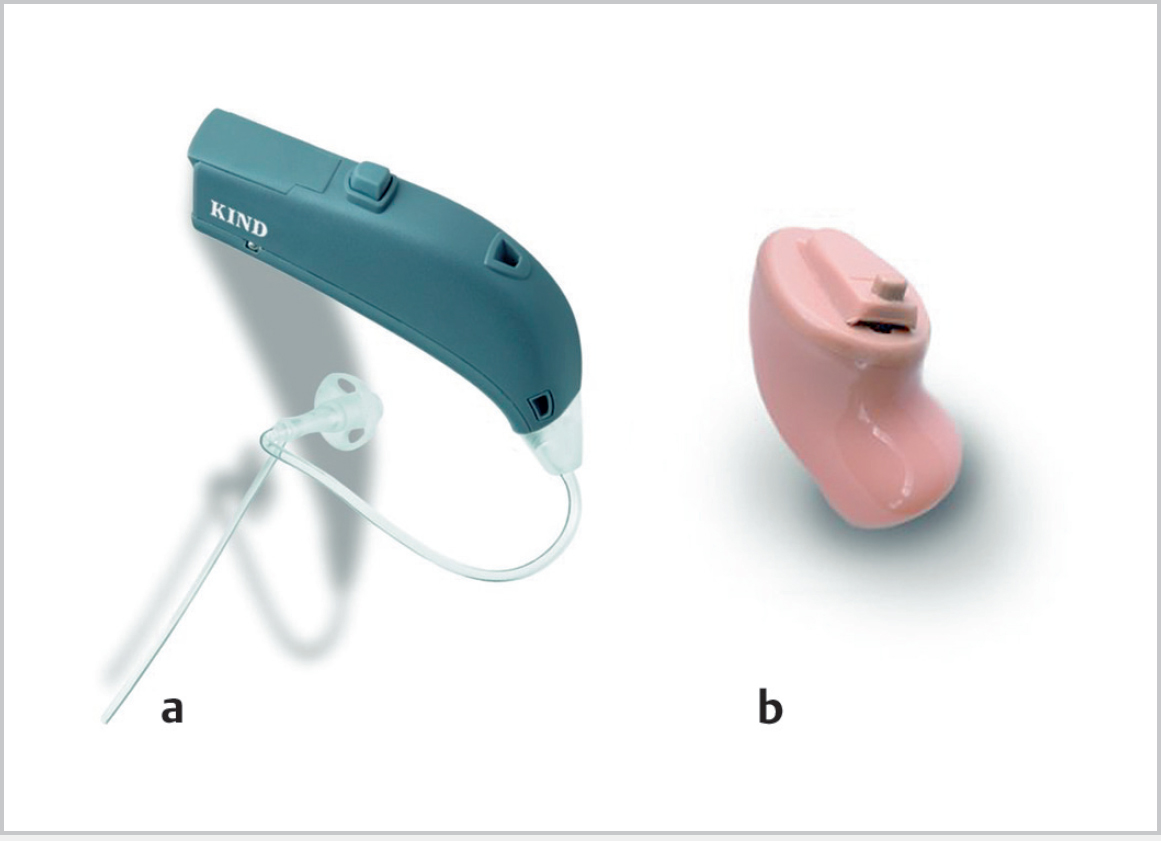
15 Hearing Aids • A hearing aid (HA) is any device that amplifies sound or assists the hearing-impaired individual (generally considered electroacoustic devices) • Consider when hearing loss (HL) ~≥30 dB, though may be suitable for minimal losses with tinnitus, or for listening in specific circumstances • For asymmetric HL generally fit poorer-hearing ear, although binaural fitting usually preferable • Glasgow benefit scale and Belfast rule of thumb can be considered for HA application as well as surgery • Microphone: converts acoustic energy to electrical energy • Amplifier: boosts the electrical signal • Receiver: transforms electrical signal back to acoustic signal and broadcasts it into the ear • Behind the ear (Fig. 15.1): most commonly available on NHS; best for more severe losses as less issues of feedback compared with in-the-ear aids • In the ear (Fig. 15.1): fills concha; suitable for mild, severe loss • In the canal: more difficult to insert (relevant if patient has arthritis, for example) • Completely in the canal • Bone conductor: suitable when no ear canal or pinna, or chronic discharge; body-worn and bone-anchored types • CROS: contralateral routing of signal • Implantable devices: middle ear transducers, cochlear implants, and auditory brainstem implants • Gain: amplification of sound sufficient for it to be heard, though not uncomfortable (acoustic gain = input–output dB) • Frequency response: can be varied in most aids to have low- or high-frequency emphasis • Compression: so that the output does not exceed the comfortable listening levels of the individual • Telecoil: allows aid to pick up sound by electromagnetic induction (e.g., telephones, cinema), excluding environmental sounds • Molds: – Feedback occurs when amplified sound leaks from receiver back into microphone • Binaural amplification: benefits include: • Acclimatization: it takes several weeks for central auditory compensation to allow patient to acclimatize to the new amplification of an HA; adjustments are often required after initial fitting, but can be automatically programmed • Data logging: some aids can be set to record timing and context of use • Suitable for patients who are hearing impaired but cannot wear conventional aids, with conductive or mixed loss:
15.1 Principles
15.2 Components
15.3 Types of HAs
 Open fit: avoids problems of occlusion caused by conventional aids, helping with low-frequency noise appreciation, quick fitting (no mold required), and allows better ear canal ventilation; generally good for high-tone losses (>1 kHz); better cosmetically
Open fit: avoids problems of occlusion caused by conventional aids, helping with low-frequency noise appreciation, quick fitting (no mold required), and allows better ear canal ventilation; generally good for high-tone losses (>1 kHz); better cosmetically
15.4 Principles
 Looser, more comfortable, and prevents occlusion effect, which makes patient’s voice sound louder because of the conductive loss a tight mold gives; however, greater potential for feedback; venting may help tighter molds
Looser, more comfortable, and prevents occlusion effect, which makes patient’s voice sound louder because of the conductive loss a tight mold gives; however, greater potential for feedback; venting may help tighter molds
 A mold blocks the external auditory canal, which traps low-frequency energy, making low-frequency internal sound (speaking, chewing) unpleasantly loud, especially if the HL is not >40 dB; vented molds help reduce this; even more if patient has “open fit” aid
A mold blocks the external auditory canal, which traps low-frequency energy, making low-frequency internal sound (speaking, chewing) unpleasantly loud, especially if the HL is not >40 dB; vented molds help reduce this; even more if patient has “open fit” aid
 Improved word identification and sound localization
Improved word identification and sound localization
 Sense of balanced hearing and elimination of head shadow effect
Sense of balanced hearing and elimination of head shadow effect
 Need for less gain
Need for less gain
15.5 Bone-Anchored HAs
15.5.1 Indications
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


