Health Economics for the Busy Ophthalmologist
Andrew F. Smith
How should eyecare treatment and blindness prevention programs be organized? How much money should be spent on specific eyecare interventions and which are the most beneficial of these interventions? How does one measure the cost and effectiveness of various ophthalmic interventions? Which diagnostic eye tests are more useful to perform than others? How does one balance the efficacy of an ophthalmic intervention with its cost? As a practicing ophthalmologist, what is one’s role in the economic aspects of the delivery of eyecare and the prevention of blindness and vision loss? These are but a few of the myriad of difficult questions faced daily by those involved in the delivery of eyecare services, chief among them the ophthalmologist. Not surprisingly, there are, of course, a range of possible answers to such questions, most of which might seem rational and appropriate. More often than not, however, the answers, which are actually implemented, are made without having all the facts at one’s disposal. The decision-making process is further complicated by a seeming lack of knowledge as to what pieces of information are most helpful to the economic decision-making process. The goal of this chapter, therefore, is to provide a brief description of some of the main ideas and techniques used by professional health economists to enhance the decision-making process pursued by both health policymakers in general and the busy clinician ophthalmologist in particular. This said, one should be wary of the fact that although the dictates of economic science may appear to be generally applicable in certain situations, their rigid application to healthcare is not without potential problems.
EFFICIENCY, EQUITY, AND UTILITY
To begin, it is necessary to provide a grasp of the main economic concepts used to situate the reader in the “health economist’s mindset.” It is useful to provide a working definition of economics. Essentially, economics is concerned with the distribution and allocation of scarce resources throughout society. Fundamental to this process is the concept of resource scarcity, meaning that the ability to satisfy one’s wants and desires is not unlimited; even given all the money in the world, constraints always exist, whether we like them or not. As such, economists have defined the “real cost” of performing a given activity relative to other potential opportunities in which an individual might have been engaged. The concept of “opportunity cost” is of vital importance to economic thinking, since it forces one to think of the next best available use for a given set of resources. From a policy perspective, for example, should resources be spent on treatment x versus treatment y. Such a set of events imposes that a necessary “trade-off” be made between x and y. The goal of economics here is to evaluate both programs (x and y) in terms of efficiency, that is, how to get the most out of each program given a backdrop of limited or scarce resources, which are either directly viewed as healthcare inputs, inputs to sectors that have healthcare benefits (e.g., education or health insurance schemes), or inputs to society’s general well-being as a whole.
There are three main principles of efficiency:
Do not waste scarce resources.
Produce each output at the lowest possible cost.
Produce those goods and services that people value the most.
When some portion of those resources can be used to produce other goods and services, then the system is deemed to be operating at “technical efficiency.” When one has to increase the resources, one has to commit to a given venture, then one is said to be technically inefficient. “Allocative efficiency,” by contrast involves taking into account the concept of cost-effectiveness (CE), in which the decision taken is essentially an economically sound one. As such, allocative efficiency hinges on making appropriate value judgments about how to allocate resources. To assist us, the famous late-nineteenth century economist, Vilfredo Pareto, proposed that allocative efficiency is “attained when it is not possible to change the allocation of resources to make any one person better off without making at least one other person worse off.” Furthermore, one can identify two factors that modify or influence efficiency, namely (1) individual welfare, in which the individual decides which goods and services to consume, and (2) the available level and distribution of income in the economy. Hence, the Pareto criterion may be restated to read “that there is no unique allocation of resources such that there is only one allocatively efficient solution. Instead, there are a range of efficient allocations, one for each different combination of wealth and income.” Overall, the concept of the Pareto criterion is more theoretical than practical, since most changes in resource allocation have negative consequences and do, in fact, make certain segments of society worse off; that is, for any health policy change, there are both winners and losers.
Essentially, health economics is concerned with discovering the best or most efficient means of allocating scarce healthcare resources to yield a given healthcare policy objective, such as reducing infant mortality, and so forth. The concept of equity or fairness significantly affects the decision to pursue various healthcare strategies or interventions and often is at odds with the concept of allocative efficiency. At this point, it is worth introducing the concept of “distributive equity,” since it forces decision makers to be concerned with where the final healthcare resources end up rather than how the resources are apportioned. In this respect, it is further useful to consider the twin concepts of horizontal and vertical equity in our dissection of the concept of distributive equity.
Horizontal equity relates to the manner in which the scholars of the day believed that it was important to distribute an equal amount of goods and services to individuals who have similar economic circumstances. Under this view, the aim of efficiency is to achieve an equal distribution of healthcare resources to ensure that individuals with similar healthcare needs and costs obtain a similar amount on a per-capita basis. Vertical equity, by contrast, relates to the desire to distribute unequal amounts of healthcare resources among differently situated individuals in relation to the degree to which they are experiencing different healthcare situations. Thus, under this view, those segments of society with greater healthcare needs would receive a greater share of the total healthcare budget. The goal of health economics is to attempt to quantify the potential end users of such healthcare resources and so determine what sort of strategy is to be pursued, be it striving toward either horizontal or vertical equity.
Traditionally, health economists have been guided in their attempts to allocate scarce resources efficiently to maximize an individual’s human capital. However, the human capital approach, as it is known, is not without its detractors, since it fails to take into account a number of important factors. Sick and mentally or physically disabled persons are always undervalued in terms of economic productivity to the economy. In addition, the human capital approach fails to take into account such factors as the wage gap, especially between the genders and different ethnic groups. As a consequence, some economists have argued that days of healthy life gained through the introduction of a particular healthcare intervention or technique need to be weighted according to the, age, sex, and ethnic group wage rate for those persons who are affected.1
An equally fundamental principle of economics is the concept of “utility maximization,” in which each individual consumer seeks to derive as much satisfaction or happiness from the consumption of goods and services as possible. However, eventually, each consumer reaches a point at which he or she no longer derives the same degree of utility or satisfaction from the consumption of a given bundle of goods and services. The point beyond which individuals cease to derive increasing utility is called the law of diminishing marginal utility (Table 1 and Fig. 1). For example, consider the case of little Johnny eating an ice cream cone. After the first or second cone, Johnny’s utility probably is still quite high; however, by the ninth or tenth ice cream cone, Johnny probably is feeling quite sick. Alas the law of diminishing marginal utility has a real-life example.
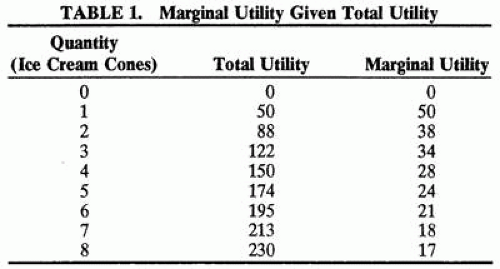 |
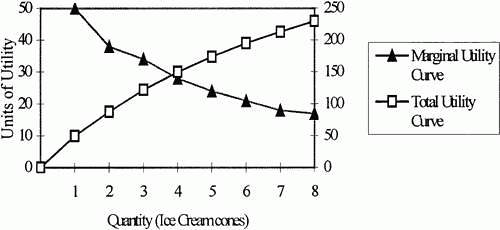 Fig. 1. Total and marginal utility. |
ANALYTIC TECHNIQUES OF HEALTH ECONOMIC EVALUATION
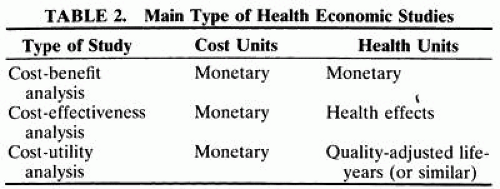
Any comprehensive economic evaluation of a healthcare intervention or proposed strategy requires two essential ingredients: (1) being able to precisely measure and (2) precisely value the cost and outcomes of the competing healthcare alternatives. Often, one is simply interested in comparing the existing technique with a proposed intervention or new technique. Overall, there are essentially three types of economic evaluation techniques: (1) cost-benefit analysis, (2) CE analysis (CEA), and (3) cost utility analysis (CUA) (Table 2).
 |
COST-BENEFIT ANALYSIS
Cost-benefit analysis (CBA) is used to evaluate the overall allocative efficiency of a healthcare intervention or program. Using this form of analysis, the goal is to determine whether it is appropriate to expend society’s resources on a given healthcare intervention or technique versus either the existing method or no available alternative. By examining each individual healthcare program or proposed intervention, the aim of CBA is to determine whether the benefits outweigh the opportunity costs associated with the healthcare intervention or strategy. To answer such a question, it is necessary to ensure that cost-benefit calculations are reported in the right units, namely, monetary units over monetary units. The challenge in using CBA is to be able to convert health benefits into monetary units.
Traditionally, the valuation of health benefits into monetary units was approximated using the human capital approach, in which the individual was solely measured for his or her economic productivity and all that mattered was how much income he or she was able to generate with a given health benefit. In this sense, productivity is normally measured in terms of labor costs, in this case, one’s future stream of economic earnings. Not surprisingly, with the human capital approach, rigidly applied, there is great difficulty in adequately gauging the economic “worth” or productivity of retirees, homemakers, and unemployed persons.
An alternative to the human capital approach is to ask patients themselves how much they would be willing to pay for improvements in their health status. This approach uses the “contingent valuation” approach to gauge the relative market price in circumstances for which there is no established price value as such. Although there is a certain amount of controversy surrounding the use of willingness-to-pay (WTP) methodologies, it is nevertheless one of the few means of directly translating health benefits into monetary terms. WTP is not, however, without its critics.
First, WTP is highly sensitive to income levels. Wealthier people have more ability to pay and, as such, may be more likely to pay for medical treatment. Second, under those healthcare systems that are government financed through the collection of taxes, the end user, or patient, of healthcare resources does not have to pay out of his or her pocket for the healthcare treatment that is received. This set of events is likely to influence the valuations for healthcare placed by persons living within such public healthcare systems. Furthermore, it often is exceedingly difficult for patients to translate the healthcare intervention they are receiving into corresponding increases in personal utility values and, hence, into monetary units. Despite the above-mentioned measurement problems inherent with the WTP methodology, WTP studies as a whole are becoming increasingly more refined and useful in assisting health economists and others in making informed healthcare allocation decisions. By calculating the costs and benefits associated with a variety of healthcare programs, it is possible to determine the various “tradeoffs” that would result from their possible implementation. Calculations of this type are especially useful against the backdrop of allocating scarce healthcare resources.
COST-EFFECTIVENESS ANALYSIS
Of the three main forms of economics analysis that are regularly used, CEA is perhaps the most often used. First, unlike CBA, CEA does not require healthcare benefits to be converted into monetary units. Overall, CEA deals with the technical efficiency of the healthcare intervention and questions relating to the best way to reach a certain defined healthcare goal or objective. Implicitly, therefore, CEA always involves a comparison between at least two options that have the same healthcare goal or objective in mind. Analytically, it is possible to compare competing healthcare objectives simply on the basis of examining the difference in the cost of attaining a fixed gain or increment in health benefit. The difficulty here arises from the fact that it may be very difficult to ensure that all of the competing healthcare interventions or strategies or both actually yield the same fixed gain in health benefit.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


