OVERVIEW
- Traumatic injury to nasal or septum causing haematoma should be drained to prevent cartilage destruction and subsequent deformity
- Nasal fractures can be manipulated back into position within 3 weeks of an injury. A delay of treatment beyond this time will allow the fracture to heal and any correction of deformity will require a rhinoplasty
- Traumatic perforations of the tympanic membrane should be managed conservatively, but all cases of middle or inner ear injury should undergo audiological and neurological assessment
- An injury to the facial area, blunt or penetrating, that results in a facial nerve weakness requires urgent specialist evaluation
- Major trauma to the head and neck requires stabilisation of airway and cervical spine as a priority
- Vascular injuries in the head and neck may be occult and a high index of suspicion will guide investigation
- Aphonia after neck injury may indicate severe laryngeal injury and impending loss of airway
A patient presenting with trauma to the head and neck region should undergo a thorough and complete examination with assessment and stabilisation of airway, breathing and circulation as a first priority.
The most common injuries to the head and neck involve blunt trauma. Motor vehicle accidents, assaults and sporting injuries commonly cause blunt trauma. However lacerations to soft tissues and penetrating injuries may also occur. A penetrating injury may initially seem trivial but the trauma could be significant with injury to the brain, orbital contents, facial nerve, aerodigestive tract, neurological or vascular structures.
Nasal injury
Nasal injury is commonly due to blunt trauma. A deviation of the nasal bones and septum can give rise to symptoms of nasal blockage and give rise to a significant cosmetic deformity (Figure 21.1). An injury to the cartilaginous and bony septum should be assessed to exclude a septal haematoma. This injury is more common in children as the mucoperichondrium is less well bound to the cartilage. If left untreated, the haematoma may become infected leading to abscess formation or a septal perforation.

An initial evaluation of the extent of a nasal injury may not be possible due to swelling. The patient is commonly seen 5 days after injury, so a full functional and cosmetic assessment may take place. A deviated and impacted nasal bone may be elevated back into position provided the manipulation is performed within 14–21 days after injury. If treatment is delayed beyond this time, fixation of the bones will occur and corrective surgery by nasal osteotomies will be needed in the form of a rhinoplasty. Uncomplicated septal deviations may be treated by a septoplasty operation.
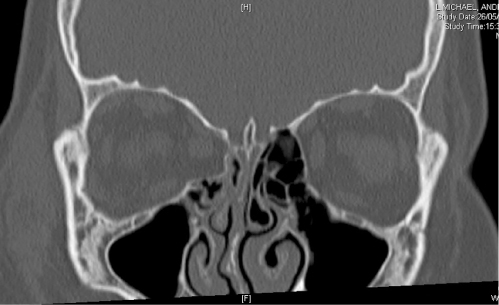
Any patient presenting with a nasal injury should be assessed for the possibility of a facial fracture. Oedema may make examination difficult but palpation of the orbital rims and zygomatic arches should be undertaken with note taken of any tenderness, irregularities or steps. The eyes should be examined to exclude any evidence of injury to the globe, optic nerve or ocular movement. Fractures involving the orbital floor can trap orbital fat or extra ocular muscles, a classical blow-out fracture (Figure 21.2). If fat is trapped then enopthalmus may be noted but entrapment of muscles can lead to diplopia.
Plain X-rays are rarely needed for the assessment of nasal fractures. However, radiological assessment of facial injury should involve CT scanning if there is any suspicion of a fracture involving the zygoma or orbital floor.
Ear trauma
All patients who are suspected of sustaining a significant trauma to the middle or inner ear or temporal bone should have a hearing assessment and undergo otoscopy. Cranial nerve assessment and a more complete neurological examination may also be indicated.
External ear
The external ear may easily be damaged by blunt trauma. If bleeding occurs within the subperichondrial space then a haematoma may form. An auricular haematoma should be drained under sterile conditions to prevent infection or fibrosis (Figure 21.3). After aspiration, a compressive dressing is applied to prevent reaccumulation of the haematoma or a seroma. If a haematoma is left untreated then the resulting deformity of the pinna due to loss of cartilage or fibrosis is cosmetically very unsightly forming the classic ‘cauliflower ear’.
Figure 21.3 Pinna haematoma.
(With thanks to my colleague Daniel Hajioff for the use of his clinical photograph of an auricular haematoma.)

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


