Fig. 15.1
Imaging in a 30-year-old female patient with multifocal head and neck paraganglioma. 18 F-DOPA PET maximum intensity projection (a), axial MRI (b), contrast-enhanced CT (c), and fused PET/MRI (d) and PET/CT images (e) showed multiple areas of increased radiopharmaceutical uptake corresponding to multiple paragangliomas of right (red arrows) and left (blue arrows) head and neck regions (Courtesy of Nuclear Medicine Department of the Oncology Institute of Southern Switzerland, Bellinzona and Lugano, Switzerland)
The introduction of SST analogues (DOTATOC, DOTATATE, DOTANOC) labeled with 68gallium (68Ga) as radiopharmaceuticals for PET has been used successfully for the diagnosis and therapy management of SST-expressing tumors, emphasizing the high sensitivity and specificity of NETs compared to SSTR scintigraphy and diagnostic CT [14].
A recent publication of our group compared both 68Ga-DOTATOC PET and18F-DOPA PET with diagnostic CT, observing a detection rate of 100 % for both functional imaging modalities in nonmetastatic glomus tumors [15]. However, in metastatic disease the per-lesion rate of 18F-DOPA PET was lower compared to 68Ga-DOTATOC PET (56 % versus 100 %, respectively), taking into account that foremost bone lesions, verified by both 68Ga-DOTATOC PET and diagnostic CT, were 18F-DOPA negative [15] (Figs. 15.2 and 15.3).
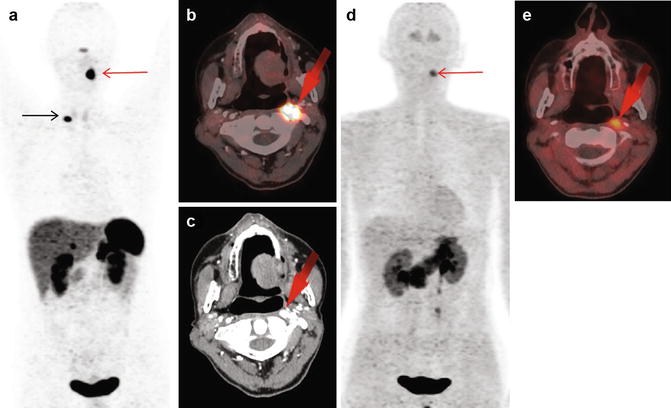
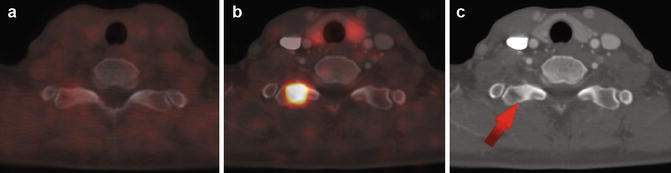
Fig. 15.2
Imaging in a 49-year-old woman with malignant head and neck paraganglioma. 68Ga-DOTATOC-PET maximum intensity projection (MIP) image (a) and PET/CT transverse image (b) showed an area of intense focal 68Ga-DOTATOC uptake (SUVmax 42.3) in the left head and neck region (red arrow). The diagnostic CT image (c) showed an area of strong contrast enhancement consistent with head and neck paraganglioma (red arrow). 18 F-DOPA PET MIP image (d) and PET/CT transverse image (e) were concordant (SUVmax 3.3). Another somatostatin receptor expressing lesion (a, black arrow) was identified as a small area of sclerosis in the transverse processes of the first thoracic vertebra (see Fig. 15.3)
Fig. 15.3
Transverse thoracic images in the same patient as shown in Fig. 15.2 18F-DOPA PET/CT image (a) showed no abnormal uptake in the bone. 68Ga-DOTATOC PET/CT image (b), in contrast, showed an area of intense focal uptake (SUVmax 19.8), corresponding to a small area of sclerosis at CT (c) in the right transverse process of the first thoracic vertebra (arrow), which was confirmed as osteoblastic metastasis. Considering both Figs. 15.2 and 15.3, 68Ga-DOTATOC PET/CT fusion changed the tumor staging from primary tumor to metastatic disease in this patient
Recent publications and case reports confirmed the high detection rate of somatostatin receptor PET/CT in HNPGL, demonstrating the high diagnostic accuracy of 68Ga-DOTANOC PET/CT compared to 131I-MIBG scintigraphy and even to conventional imaging (CT or MRI), including distant metastases [16, 17]. This is in line with previous publication of our group, comparing 123I-MIBG scintigraphy including SPECT/CT to 68Ga-DOTATOC PET/CT in patients with glomus tumors [18] (Figs. 15.4 and 15.5). Thereby, all head and neck manifestations were verified by both diagnostic CT and 68Ga-DOTATOC PET compared to 123I-MIBG SPECT/CT, which detected only one out of 17 positive 68Ga-DOTATOC PET/CT lesions. Additionally, all distant metastases (e.g., the abdomen, bone) were verified by 68Ga-DOTATOC PET/CT, providing the accurate tumor extent of patients with extra-adrenal PGL, compared to 123I-MIBG scintigraphy, including SPECT/CT [18] (Figs. 15.4 and 15.5). To explain this on a molecular level, it has been suggested that extra-adrenal PGL could undergo dedifferentiation, leading to a loss of norepinephrine transporter or vesicular monoamine transporter (VMAT), which could then lead to false-negative 123I-MIBG scintigraphy findings in metastatic disease [19]. In contrast to the excellence of 123I-MIBG imaging in the detection of primary sympathetic PGL, its sensitivity is low in parasympathetic HNPGL [20]. Fottner et al. suggested that this could result from the under-expression of VMAT-1 in HNPGL [21]. Although 111In-pentetreotide scintigraphy shows high sensitivity in HNPGL [8], as mentioned above, it is limited in detecting PGL lesions of sympathetic origin and – additionally – limited by its lower spatial resolution compared to PET [10].
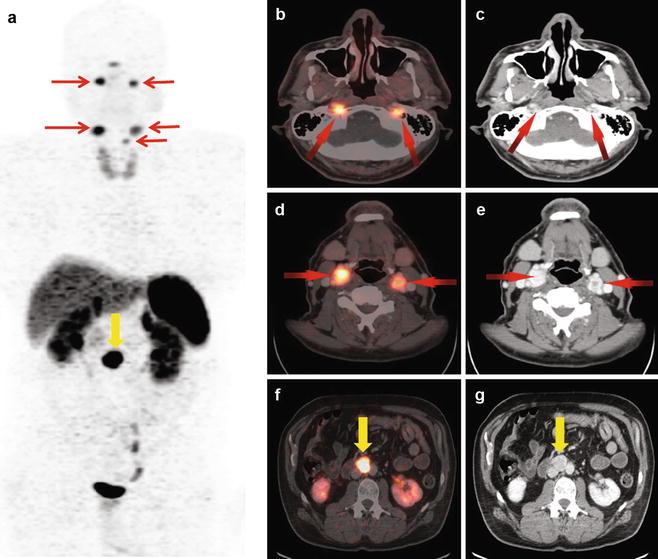
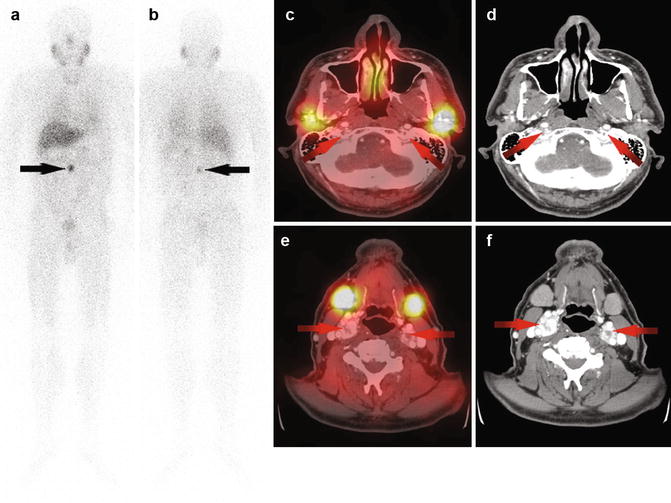




Fig. 15.4
Imaging in a 58-year-old man with multifocal extra-adrenal paraganglioma. 68Ga-DOTATOC PET maximum intensity projection (MIP) image (a) and transverse PET/CT images (b, d) show some areas of intense focal 68Ga-DOTATOC uptake in the head and neck region (red arrows). The diagnostic CT images (c, e) show strong contrast-enhanced lesions consistent with head and neck paragangliomas (red arrows). The intense focal uptake evident at 68Ga-DOTATOC-PET in the abdomen (a, f, yellow arrow) is confirmed on diagnostic CT images (g, yellow arrow) as being an extra-adrenal paraganglioma
Fig. 15.5
Additional imaging in the patient seen in Fig. 15.4. 123I-MIBG planar scintigraphy in anterior (a) and posterior (b) views shows a focal area of increased 123I-MIBG uptake in the abdomen (arrows) confirmed by 68Ga-DOTATOC PET/CT as being an extra-adrenal paraganglioma (see Fig. 15.4). After software-based image fusion of SPECT images with diagnostic CT images (c, e), symmetrical physiological 123I-MIBG uptake was observed in the parotid (c) and submandibular (e) glands. All verified head and neck lesions evident at contrast-enhanced CT (d, f, red arrows) were 123I-MIBG negative (c, e). Considering the findings showed in Figs. 15.4 and 15.5, 68Ga-DOTATOC PET/CT changed the tumor staging from primary extra-adrenal paraganglioma to multifocal disease in this case
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
