OVERVIEW
- Head and neck cancer is increasing as the population ages
- Squamous cell carcinoma of the mucous membrane is the most common cancer identified in the head and neck
- Head and neck cancer associated with excessive use of alcohol and smoking in the elderly, and with human papilloma virus (HPV) in the younger patient
- The most common site identified in the UK and EU population is the oral cavity and the larynx
- Oral cavity cancer presents most common on the later border of the tongue, with ulceration and pain
- Larynx cancer, most frequently presents with painless hoarseness, because of involvement of the vocal cord
- Prognostic factors include the site of the primary disease and its TNM stage, as well as each patients’ co-morbidity
- Choice of treatment is a balance between the efficiency of treatment and the likelihood of survival, also including functional and quality of life outcomes
Definition
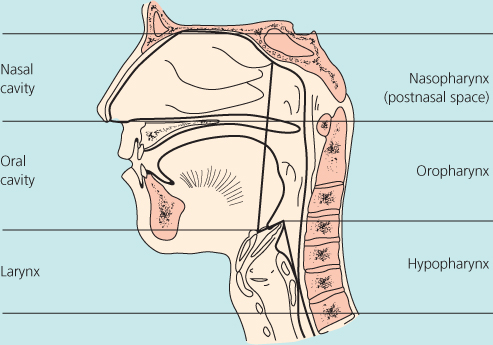
Head and neck cancer encompasses any malignant diagnosis of organs and supporting tissues, the majority being the mucous membrane, above the clavicle, yet not including the brain and orbits. Skin cancer is generally not included, yet some clinicians will also manage such patients, as both diseases occur in a similar aged population. Thus cancers of the oral cavity, nose, paranasal sinuses and nasopharynx, oropharynx, larynx and hypopharynx are included (Figure 24.1). Also included, but may vary worldwide, are the salivary glands and the thyroid.
The majority of head and neck cancers are squamous cell carcinomas of the oral cavity and larynx, whereas cancers of the salivary glands and the thyroid gland are unique to their anatomical area. When cancer affects the head and neck area major functions can be affected such as speech, voice, swallowing, taste, and smell, and treatment can result in additional functional alterations resulting in variable effects on patient’s quality of life. When making a treatment decision a balance between the efficiency of treatment and the likelihood of survival needs to be considered, including functional and quality of life outcomes. Attempts to encompass such decision-making has resulted in the “Head and neck cancer multidisciplinary team (MDT)” meeting weekly to discuss and plan patients treatment, anticipate any physical and psychological support required, and to plan functional rehabilitation.
Incidence
Cancer of the mouth is the tenth most common cancer worldwide, but is the seventh most common cause of cancer deaths. Nasopharyngeal cancer is largely restricted to southern China, and oral cavity cancer is highest in India. The highest incidence of head and neck cancer is seen in South East Asia, Western Pacific and Western Europe. The male to female ratio reported varies from 2:1 to 15:1 depending on the site of disease.
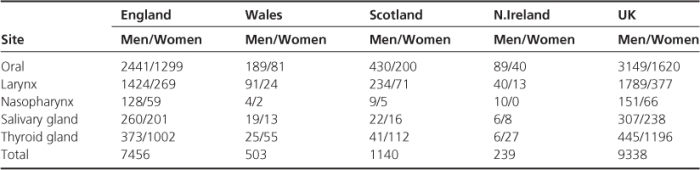
Head and neck cancer in the European Union (EU) 2008, reports that laryngeal cancer is the most frequent diagnosed, most often within the age 50–70 years and is rarely made in patients younger than 40 years. The overall incidence of laryngeal cancer was 3.4 per 100 000 with a mortality of 1.6. The incidence in men is 6.8, with a mortality of 3.4, and the incidence in women is 0.6, with a mortality of 0.2 per 100 000. The estimated incidence per 100 000 of laryngeal cancer ranges from 8.9 in Hungary to 1.6 in Sweden, with men more likely to be affected 5–7:1 women. The recorded new cases by country, sex and site in the UK are tabulated (Table 24.1).
Table 24.1 Recorded numbers of new cases of head and neck cancer in the UK 2004.
Risk factors
Tobacco (smoking and smokeless products such as quid) and alcohol are the major risk factors worldwide and account for approximately 75% of all cases. Their effects are multiplicative when combined. Smoking is more strongly associated with laryngeal cancer and alcohol consumption than it is with cancers of the pharynx and oral cavity. Quitting tobacco smoking for a short period of time (1–4 years) results in a head and neck cancer risk reduction of around 30% compared with current smoking, and after 20 years can reduce the risk of developing oral cavity cancer to the level of a lifelong non-smoker and the risk of laryngeal cancer by 60% after 10–15 years. The benefits of cessation or quitting alcohol, on the risk of developing head and neck cancer, are observed after more than 20 years, when the level of risk reaches that of non-drinkers. While most people who smoke and drink do not develop a head and neck cancer, a genetic predisposition has been demonstrated. Virus infections as a risk factor have been recognised since the mid 1960s with Epstein–Barr virus (EBV) and the development of nasopharyngeal cancer. Recently the HPV subtype16 (human papilloma virus) has been associated with a significant rise in the diagnosis of oropharyngeal cancer. This disease is a distinct disease entity, with patients being diagnosed younger (usually under 50 years), usually not indulging in smoking and excess alcohol intake, most often presenting with enlarging and palpable cervical lymph nodes.
Presentation
Patients with head and neck cancers present with a variety of symptoms, depending on its site location. Laryngeal cancer commonly presents with hoarseness. Pharyngeal cancer may present in the early phase with a sore throat, local pain, “feeling of a lump in the throat” or a neck mass, and when late with dysphagia, hoarseness and/or breathing difficulty. Oral cavity cancer presents early with a painful ulcerative lesion on the lateral border of the tongue with/or without a neck swelling (Figure 24.2). Nose tumours may present with unilateral nasal obstruction, a bloody nasal discharge or even deafness in one ear!

Patients with a head and neck cancer present frequently with a neck swelling which is gradually increasing in size. Many others are diagnosed with non-specific symptoms commonly associated with benign conditions, such as throat discomfort, earache, cough or alteration to voice quality. Within the NHS, “Referral guidelines for the patients with suspected cancer” have been drawn up (Box 24.1) and patients with such symptoms will be seen by a cancer specialist within the “2-week rule”.
Head and neck: urgent referral
- An unexplained lump in the neck, of recent onset, or a previously undiagnosed lump that has changed over a period of 3–6 weeks
- An unexplained persistent swelling of the parotid or submandibular gland
- An unexplained persistent sore or painful throat
- Unilateral unexplained pain in the head and neck area for >4 weeks, associated with otalgia (ear ache) but a normal otoscopy
- Unexplained ulceration of the oral mucosa or mass persisting for >3 weeks
- Unexplained red or white patches (including suspected lichen planus) of the oral mucosa that are painful or swollen or bleeding
Thyroid: urgent referral
- A solitary nodule increasing in size
- A history of neck irradiation
- A family history of an endocrine tumour
- Unexplained hoarseness or voice change
- Cervical lymphadenectomy
- Very young (prepubertal) patient
- Patient aged 65 years or older
What’s the hospital process?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


