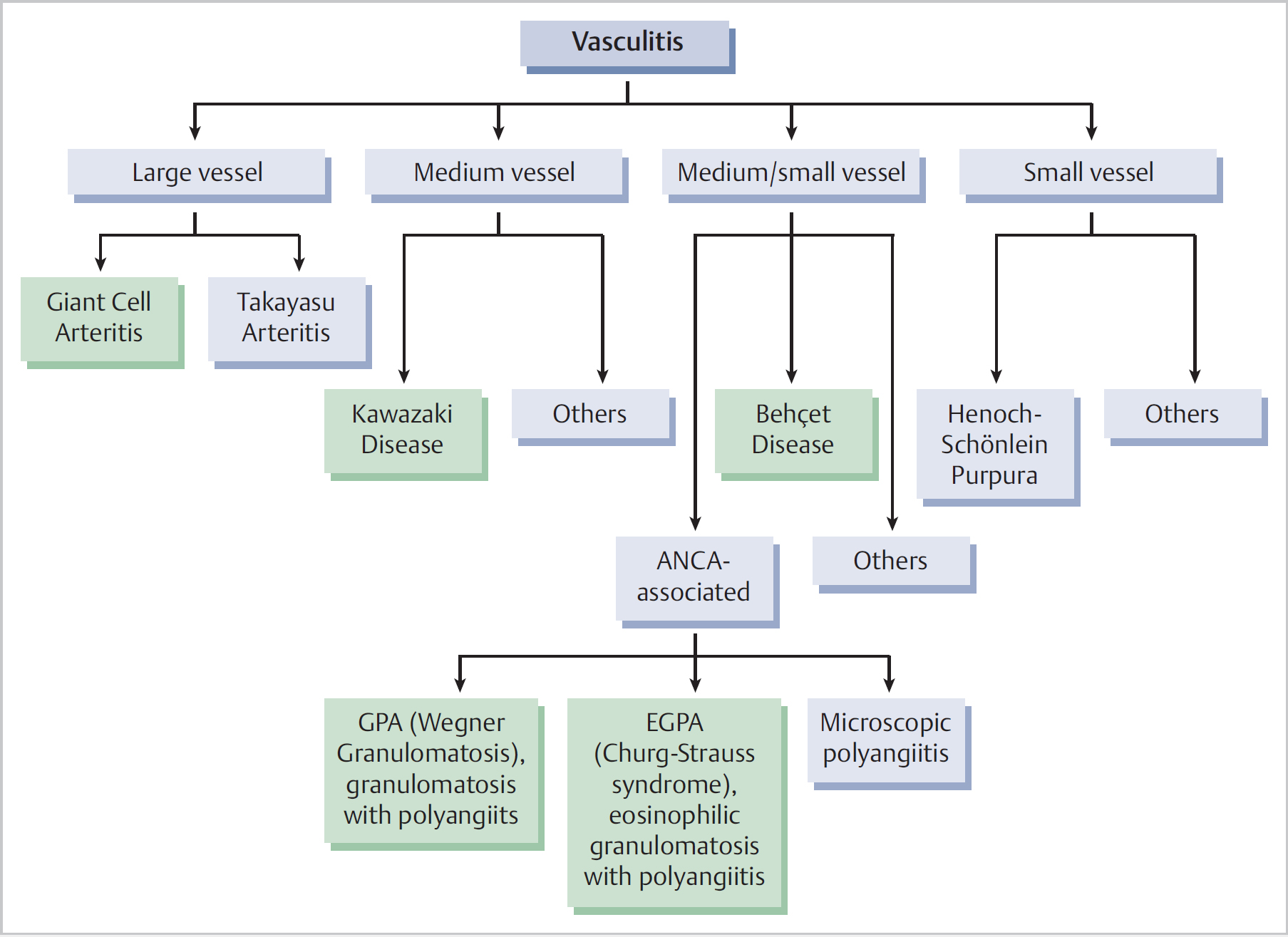
23 Granulomatosis with Polyangiitis and Other Vasculitides in the ENT Region • Vasculitis consists of a heterogeneous group of systemic conditions involving the inflammation of blood vessels • Tissue damage occurs either due to vessel wall damage and haemorrhage into adjacent tissue (e.g., vasculitic rash), or secondary to endothelial tissue, impairment of blood flow, and ischaemia of dependent structures (e.g., septal perforation) • In each type of vasculitis the disease generally follows a certain organ distribution pattern but can nevertheless affect a variable combination of organs in any given patient • There can be a significant overlap between each form of vasculitis as well as with other immune-mediated conditions. Although classifications are essential for designing the best treatment, communication, and research, always consider that these are “man-made” boundaries when assessing ENT patients with suspected vasculitis • These conditions are specialty examination favorites. When suspecting vasculitis as the patient’s diagnosis, remember to seek the opinion of a rheumatologist or other physician with a special interest in vasculitis as part of the answer • Fig. 23.1 demonstrates types of vasculitis more commonly affecting the ENT region (shaded), within the wider vasculitis disease group • Recent pathophysiological and ethical developments have led to new nomenclature for the ANCA-associated vasculitides: • Multisystem granulomatous vasculitis of small/medium arteries, most commonly affecting the paranasal sinuses, lungs, and kidneys • Systemic symptoms: malaise, unexplained pyrexia, weight loss • ENT involvement: resistant sinusitis, purulent rhinorrhoea, epistaxis, septal perforation, saddlenose deformity, secondary atrophic rhinitis with nasal crusting that continues after remission of disease activity, middle ear disease, laryngeal inflammation, subglottic stenosis • Over 60% of all GPA patients initially present with ENT symptoms, highlighting the role of otolaryngologists in its diagnosis • Delay in diagnosis and treatment can lead to irreversible tissue damage in vital organs (e.g., kidneys), highlighting the importance of early diagnosis • Over 80% of patients with classic multisystem involvement have raised anti-neutrophil cytoplasmic antibody (ANCA) titers, mostly of the cytoplasmic pattern (c-ANCA) and against the proteinase 3 antigen (c-ANCA-PR3) • ANCA positivity occasionally occurs in other non-vasculitic conditions such as inflammatory bowel disease, rheumatoid arthritis, and other autoimmune diseases, HIV, and other chronic infections • In the limited form of GPA (ENT ± lungs) over 50% of patients are ANCA negative, posing a diagnostic challenge for the ENT surgeon • Always consider CXR (cavitating pulmonary nodules) and urinalysis (blood cells, proteins) in addition to ANCA if suspecting GPA • Nasal biopsies have a maximum diagnostic yield of 25% and only when large samples are taken from macroscopically abnormal areas • Samples from clinically normal nasal mucosa or quiescent subglottic lesions (stenoses) are nondiagnostic • Paranasal sinus CT findings may include bony destruction, new bony formation, and orbital pseudotumours • Association with relapsing polychondritis, presenting with lobulesparing pinna chondritis, nasal pain, subglottic stenosis, and vestibulocochlear involvement • Treatment requires immunosuppressant agents in addition to corticosteroids in the majority of patients (compare with CSS)
23.1 General Description
23.2 Vasculitis in ENT
 Granulomatosis with polyangiitis (GPA, formerly Wegener granulomatosis or WG)
Granulomatosis with polyangiitis (GPA, formerly Wegener granulomatosis or WG)
 Eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg–Strauss syndrome or CSS)
Eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg–Strauss syndrome or CSS)
23.3 Granulomatosis with Polyangiitis or Wegener Granulomatosis
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


