Fig. 5.1
Artificial subconjunctival drainage (trabeculectomy) versus physiologic canal-based collector channel outflow. (a) During trabeculectomy, a segment of tissue is removed at the limbus, creating a sclerostomy site (arrow). (b) This creates a pathway for aqueous to exit underneath the sclera (false passageway) into the subconjunctival space, creating a non-physiologic outflow pathway, seen as a bleb. (c) Improvement in physiologic outflow. Appearance of episcleral veins (black arrow) 1 week post-canal-based surgery, IOP 12 mmHg. (d) When the patient looks slightly up, the IOP increases, forcing aqueous into recently cleaved open Schlemm’s canal and out the adjacent veins causing a transient laminar washout of venous blood (white arrows). The black and white arrows are located in the same episcleral positions. This is similar to the phenomena of laminar flow in aqueous veins as described by Goldmann and Ascher
Fig. 5.2
Glaucoma surgery algorithm for physiologic restoration of outflow. It is no longer necessary to filter every glaucoma patient; the surgeon and patient now have the option to enhance flow into the patient’s natural drainage system. Surgeons with experience in filtration and tube surgery along with canal-based techniques have greater options in order to tailor the surgery to the patient’s specific needs. In general, patients with earlier disease who have less damage to their natural collectors are good candidates for MIGS, while patients with advanced disease whose collectors are atrophic are better candidates for creation of a new drainage system as in filtration or tube shunt surgery. **indicates non-FDA approved devices/procedures
Trabeculotomy, a time honored bleb-less angle procedure, reduces IOP by increasing flow into the natural outflow pathway. It cleaves open a diseased glaucomatous outflow system and improves aqueous flow into Schlemm’s canal and adjacent collector channels, thereby avoiding an artificial bleb drainage system. Trabeculotomy has evolved over the past 50 years from an ab externo metal segmental trabeculotome approach to a minimally invasive gonioscopy assisted ab interno microcatheter (iTrack, Ellex Medical Lasers, Ltd.) circumferential approach [4–9]. In this chapter, the authors describe the Gonioscopy Assisted Transluminal Trabeculotomy (GATT) procedure, an ab interno suture-less circumferential MIGS for the treatment of adult and developmental open angle glaucomas [10].
5.2 Preoperative Evaluation
Prior to considering a GATT surgery, one must evaluate the drainage angle using a gonioprism preoperatively. The patient must not only have an open angle with identifiable landmarks but the angle must also be free of extensive peripheral anterior synechiae (PAS) or neovascularization, as this may result in extensive bleeding and inflammation and thus surgical failure. The cornea must also be sufficiently clear to allow for a proper view intraoperatively. If the patient has an unstable intraocular lens (IOL), one should consider an alternative surgery as the GATT surgery requires a moderate amount of intraocular manipulation.
5.3 Surgical Procedure
After a standard sterile preparation, the surgical eye is draped and an open wire nasal lid speculum inserted to hold the eyelids open. A 23-gauge needle paracentesis track, oriented tangentially, is placed in either the supero-nasal or infero-nasal quadrant (Fig. 5.3a). This initial track serves as the entry site for the microcatheter or suture. A viscoelastic (sodium hyaluronate) is injected into the anterior chamber through this site. A temporal paracentesis is created (Fig. 5.3b). A suture (the authors prefer a 4.0 or 5.0 nylon suture, however, others prefer a 6.0 polypropylene suture) with a blunted tip or the microcatheter (iTrack, Ellex) is inserted into the anterior chamber through the entry site with the tip resting in the nasal angle (Fig. 5.3c). The microscope and the patient’s head are then oriented to allow proper visualization of the nasal angle with a Swan-Jacob goniolens. A 1–2 mm goniotomy of the anterior trabecular meshwork is created in the nasal angle with a microsurgical blade through the temporal site (Fig. 5.3d). Typically, upon decompression of the eye, blood will reflux into the canal, allowing for improved identification of angle structures. Microsurgical forceps are then introduced through the temporal site and used to grasp the microcatheter or suture within the anterior chamber. The distal tip of the microcatheter is then inserted into Schlemm’s canal at the goniotomy incision (Fig. 5.3e). Within the anterior chamber, the microsurgical forceps are used to advance the catheter through the canal circumferentially 360°. Viscoelastic is reinserted as needed to keep a clear medium for optimal viewing.
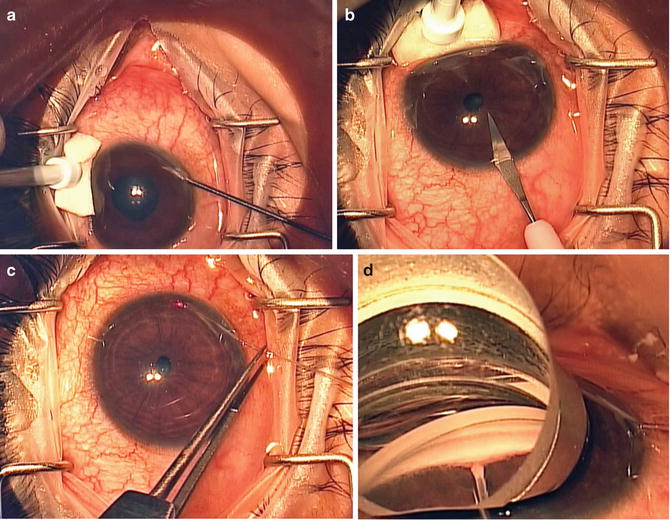
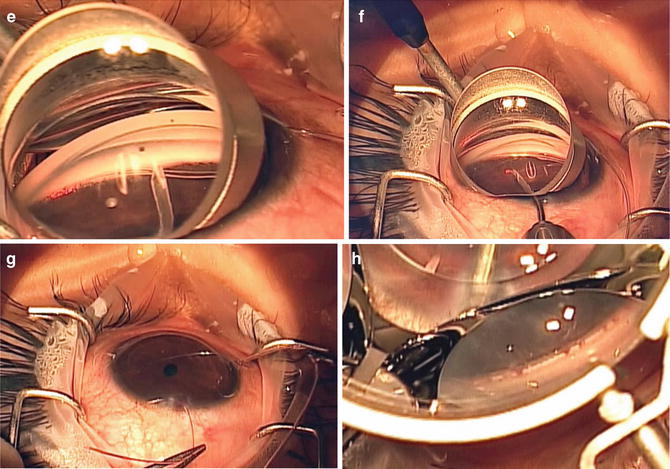
Fig. 5.3
GATT procedure. (a) tangential nasal paracentesis is made with a 23 gauge needle followed by miochol and viscoelastic. (b) A larger temporal paracentesis is fashioned with a 15° blade; this site will accommodate entry for the microsurgical graspers. (c) The iTrack catheter is inserted into the anterior chamber. The distal tip rests above the iris in the nasal angle and the proximal portion is secured to the nearby drape for directional stability. (d) After appropriate tilting of the microscope and patient’s head, the angle is viewed through the Swan-Jacob goniolens. An MVR blade is used to create a 1–2 mm goniotomy for access to the canal. Expose the canal as seen in the photo. (e) Insert the microcatheter into the canal while visualizing the course of the illuminated tip. (f) Advance the tip for 360°, then retrieve the illuminated tip from the angle, pulling it towards and out the temporal paracentesis site. This initiates the circumferential trabeculotomy. (g) Stabilize the distal tip of the microcatheter as it exits from the temporal incision and pull the proximal portion of the catheter to complete the trabeculotomy. (h) Intraoperative goniophotograph of angle immediately after trabeculotomy demonstrating an opened canal with blood reflux from adjacent collectors. At the end of the procedure, after AC washout, the wounds are hydrated with BSS until watertight
When using a microcatheter, the surgeon can visco-dilate the canal as the catheter is being passed as this may improve outcomes. If this is performed, one must keep the catheter moving for if the catheter stops, a Descemets detachment can occur. The progress of the microcatheter is noted by observing the illuminated tip. When a suture is used, the progress of the suture can be appreciated through use of a gonioprism. Upon retrieving the distal tip, after the catheter has passed 360° around the canal, the catheter tip is externalized from the temporal corneal incision creating the first half of the 360° trabeculotomy (Fig. 5.3f). Then, traction is placed on the proximal aspect of the catheter, thus completing the 360° ab interno trabeculotomy (Fig. 5.3g). Intraoperative inspection of the anterior chamber angle immediately after performance of the trabeculotomy often reveals discrete areas of blood reflux from adjacent collector channels (Fig. 5.3h). The viscoelastic is then removed from the anterior chamber by a two-handed irrigation aspiration system in order to wash the anterior chamber of blood. Near the end of the procedure, a 25 % anterior chamber fill with viscoelastic can be instilled to help tamponade bleeding from the canal. This may decrease the chance of a significant postoperative hyphema. The wounds are hydrated and checked to ensure a watertight closure. Postoperative steroid (sub-conjunctival or intracameral) and antibiotic drops are given per the surgeon’s discretion.
In certain cases, the suture or microcatheter cannot be passed 360° in one direction and stops at around 180–270°. In these limited trabeculotomy cases, create a new paracentesis site in order to better access the termination of the catheter or suture tip. Perform the goniotomy directly over the site where the probe stopped and retrieve the distal end from this location cleaving the cannulated part of the canal. A suture/microcatheter can then be passed in the opposite direction through an additional 23-gauge needle incision thus completing a 360° trabeculotomy.
5.4 Intraoperative Evaluation
During the irrigation/aspiration portion of this surgery, one can often appreciate an episcleral venous fluid wave [11]. The authors feel this is intraoperative evidence and confirmation of an intact collector system and is correlated with postoperative IOP control.
5.5 Postoperative Evaluation and Care
After surgery, all patients should be given topical broad-spectrum antibiotics and topical steroids. Pilocarpine can be used in the immediate postoperative period if the IOP is >15 mmHg; this may help keep the trabecular shelf open. The topical antibiotics should be stopped at postoperative week 1. The topical steroids (prednisolone acetate 1 %) should be tapered over 1–2 months, depending on the inflammation. Topical nonsteroidal anti-inflammatory (NSAID) drops can be used in addition to steroids to help control inflammation. Patients sometime have an IOP spike due to topical steroids. In these situations, the authors have used NSAIDS to control inflammation while rapidly tapering topical steroid drops. The patient’s IOP should be treated during the postoperative period per the surgeons’ discretion however, usually once steroid drops are eliminated, the IOP will decrease. Typically, patients are seen on postoperative day 1, week 1, and then 2–3 weeks later. Afterwards, patients are then followed a month or two after and then every 3 months for a few visits before scheduling them out to every 6 months. Gonioscopy should be performed around the 1 month visit and then regularly afterwards to ensure that the trabecular shelf remains open and free of PAS (Fig. 5.4).
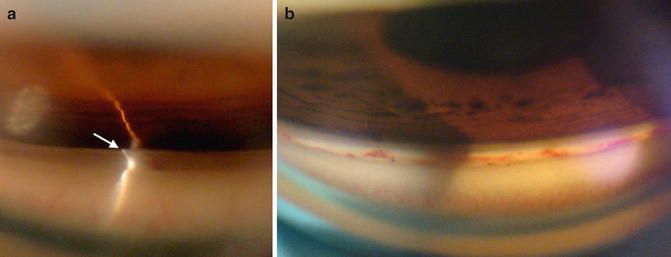
Fig. 5.4
Angle goniophotograph post-trabeculotomy. (a) Trabecular shelf. When the angle is successfully cleaved open, a large trabecular leaflet of tissue, termed the trabecular shelf, extends well over the iris. This is easily and consistently seen on gonioscopy within the superior angle. Filamentary cleavage of the canal creates this type of opening because the vector forces during cleavage of the suture or iTrack preferentially open first at Schwalbe’s line. The large posterior leaflet then protrudes over the iris and may attach to it, keeping the canal open. (b) Blood in angle post-trabeculotomy. Blood may be seen at various stages of healing in the angle post-trabeculotomy. Some of the blood appears to be in Schlemm’s canal as expected. However, other vessels may represent undesirable or excessive scarring (wound healing) in the canal. At this time, our knowledge of wound healing in the canal after trabeculotomy is limited
5.6 Outcomes
Several authors have reported on the success rates of circumferential ab externo trabeculotomy in various adult open angle glaucomas as well as pediatric glaucomas. Ikeda et al. reported nearly a 90 % success rate with a mean follow-up of 9.5 years, in patients diagnosed with developmental glaucoma that were treated with an ab externo trabeculotomy [12]. Similarly, Tanihara reported success rates in patients with primary open angle glaucoma (POAG) and pseudoexfoliation glaucoma (PXF) of 76.4 % and 83.6 %, respectively, at 1 year. After 5 years, the success rates dropped to 58 % and 73.5 % in POAG and PXF patients, respectively [13]. Of note, there was substantial loss to follow up after 5 years in this study. Additionally, the success rates for trabeculectomy were similar to those reported at 5 years with the Tube versus Trabeculectomy (TVT) study [3]. Other authors have reported better long-term results. For example, Iwao et al. reported compared ab externo trabeculotomy with trabeculectomy in patients diagnosed with steroid-induced glaucoma [14]. These authors demonstrated that after 3 years, the trabeculotomy group had a success rate of 78.1 % versus 55.8 % in the trabeculectomy group.
Preliminary results with the GATT procedure are very similar (if not better) than the previously published results for ab externo trabeculotomy. The authors reviewed all cases that underwent a GATT surgery with at least 6 months of follow up (unpublished data). This study included 203 eyes of 177 patients, 66 % Caucasian, with an average age of 64.5 years, all of whom underwent the GATT procedure. The analysis was divided between a high pressure group (preoperative IOP ≥ 18 mmHg) and a low pressure group (preoperative IOP < 18 mmHg). The “high pressure” group (n = 159 eyes) had a preoperative IOP averaging 26.7 ± 7.8 mmHg on 3.2 ± 1.1 medications. In eyes with ≥6 months follow-up (n = 92 eyes), the mean IOP was reduced to 14.8 ± 5.6 mmHg on an average of 1.4 medications (p < 0.001). By 1 year, the cumulative proportion failing was 34.8 %. The “low pressure” group (n = 44 eyes) had a preoperative IOP averaging 15.3 ± 2.1 mmHg on 2.6 ± 1.1 medications. In eyes with ≥6 months follow-up, the mean IOP was reduced to 13.5 ± 3.5 mmHg on 0.7 ± .8 medications (p = 0.010). Overall, 38 of 203 eyes (18.7 %) were considered treatment failures, with 16 of the 38 eyes requiring further glaucoma surgery.
Grover et al. published on the initial results in POAG and secondary open angle glaucoma patients [10]. The group of patients was the same as the group reported above; however, the data was reported differently. Only one eye per patient was included (randomly selected). If an eye had a complication or failure from the surgery, they were also included in the study. This analysis strategy allowed for a more conservative approach to outcomes data analysis. Using this analysis, 85 patients with an age range of 24 to 88 years underwent GATT with at least 6 months of follow-up. In the 57 patients with POAG, the IOP decreased by an average of 7.7 mmHg [(SD, 6.2 mmHg) or 30.0 % (SD, 22.7 %)] with an average decrease in glaucoma medications of 0.9 (SD, 1.3) at 6 months. In this group, the IOP decreased by 11.1 mmHg (SD, 6.1 mmHg; 39.8 % [SD, 16.0 %]) with 1.1 fewer glaucoma medications at 12 months. In the secondary glaucoma group of 28 patients, IOP decreased by 17.2 mmHg (SD, 10.8 mmHg; 52.7 % [SD, 15.8 %]) with an average of 2.2 fewer glaucoma medications at 6 months. In this group, the IOP decreased by 19.9 mmHg (SD, 10.2 mmHg; 56.8 % [SD, 17.4 %]) with an average of 1.9 fewer medications (SD, 2.1) at 12 months. Failure was defined as postoperative IOP ≥21 mmHg and/or a drop in IOP <20 % or need for further glaucoma surgery. Using this definition, treatment was considered to have failed in 9 % (8/85) of patients because of the need for further glaucoma surgery. The cumulative proportion of failure at 1 year ranged from 0.1 to 0.32, depending on the group. Lens status or concurrent cataract surgery did not have a statistically significant effect on IOP in eyes that underwent GATT at either 6 or 12 months (P > 0.35). The most common complication was transient hyphema, seen in 30 % of patients at the 1-week visit.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


