Fig. 6.1
Size comparison of glaucoma drainage device and XEN Gel Stent implant
6.2.1 Lumen Size and Flow
Laminar flow through a tube is calculated based on Hagen–Poiseuille equation (Eq. (6.1)). Outflow resistance depends on the tube geometry, flow rate, and viscosity of liquid. To avoid hypotony, the maximum flow rate should equal the maximum production of aqueous in the human eye (which is 2 μL/min or 3 mL per day). The resistance of outflow is a combination of outflow resistance of the tube and outflow resistance of the subconjunctival space. We all agree that outflow resistance of the subconjunctival space is minimal, therefore all outflow resistance has to come from the tube itself. In a glaucoma drainage device such as the Ahmed Glaucoma Valve (New World Medical, Inc.), outflow resistance comes from the valve mechanism; in Baerveldt Glaucoma Implants (Abbott Medical Optics, Inc.), the tube is initially ligated to allow a capsule to form around the plate to increase subconjunctival resistance. In the XEN 45 Gel Stent, the size of the lumen is small to allow enough flow resistance based on Hagen–Poiseuille equation to prevent hypotony. The size of XEN 45 Gel Stent reduces the risk of hypotony by providing 6–8 mmHg of flow resistance.
6.3 Surgical Technique
A less invasive ab-interno approach is used. The injector is a single use 27 gauge needle with a preloaded XEN Gel Stent in a peel pack. The injector is designed to protect the XEN Gel Stent and to accurately deliver into the correct anatomical location. Placement is 1 mm posterior to limbus in the anterior chamber angle. During implantation, the stent will be hydrated and swell into place to decrease the risk of migration; the lumen diameter remains fixed.
Please refer to the accompanying Video for a step-by-step delivery technique.
Get Clinical Tree app for offline access

1.
Prep the eye in a standard fashion.
2.
Intended placement quadrant is supero-nasal and 3 mm behind the limbus (marking pen used).
3.
Corneal incision: main and sideport incisions are created.
4.
A preloaded, single use injector is provided to the physician.
5.
Viscoelastic is injected in the eye to allow better visualization and stability.
6.
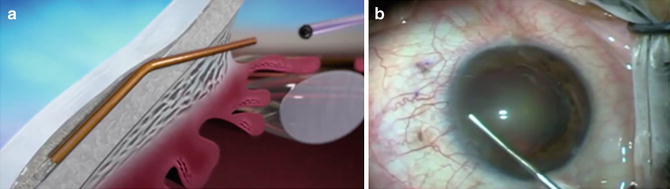
Optional goniolens used. Placement is forgiving: anywhere from Schwalbe’s line to scleral spur (Fig. 6.2a, b).
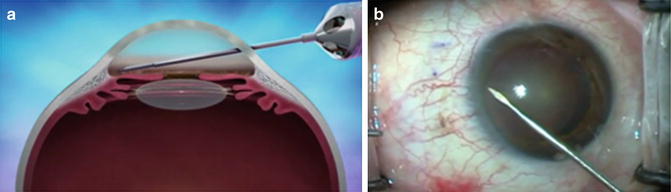
Fig. 6.2
Illustration (a) and surgical footage (b) of inserter passing across the anterior chamber to reach the angle
7.
The needle is pushed to go through the sclera and into the subconjunctival space; bevel is visualized under the conjunctiva (Fig. 6.3a, b).
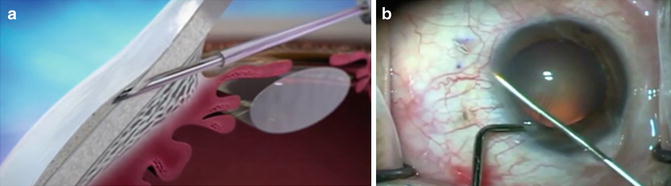
Fig. 6.3
Illustration (a) and surgical footage (b) of needle entering the angle and creating a ~3 mm scleral tunnel. Blue arrows pointing at the pre-marked target exit at 3 mm from the limbus
8.
The XEN Gel Stent is deployed and visualized under the conjunctivae (Fig. 6.4a, b).
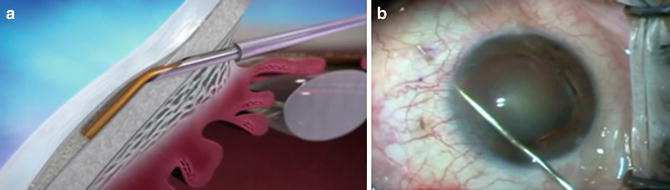
Fig. 6.4
Illustration (a) and surgical footage (b) of implant being deployed in position (blue arrow pointing at distal end of implant)
9.
Procedure is complete by retracting the injector and disposing it (Fig. 6.5a, b).