Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

18

Glaucomas
Glaucoma in children is unusual; however, when intraocular disease is suspected in childhood the possibility of a primary or secondary elevation (or depression) of intraocular pressure must always be considered. Previously recognized causes of glaucoma in childhood are listed in Table 18-1. The diversity among these conditions should be noted.
 Signs and Symptoms
Signs and Symptoms
The symptoms of childhood glaucoma are highly variable. Although some children are asymptomatic, others develop intense light sensitivity associated with corneal opacification, epiphora, and loss of vision. There may be a gradual occurrence of these problems, or alternatively a child may be asymptomatic for months and then develop these signs and symptoms acutely. Rapid elevation of eye pressure causes pain. Abnormal enlargement of the cornea and eye occurs in children under 3 years of age secondary to an elevated intraocular pressure. Review of past facial photographs often confirms the presence of this defect many months prior to its recognition by the child’s parents. A cloudy cornea is the most common first sign of childhood glaucoma seen by parents or physicians in children with unsuspected glaucoma (Fig. 18-1). When bilateral and slow in onset, it may be accepted as normal for many months. The loss of corneal transparency is caused by edema of the corneal epithelium and stroma. Careful inspection of the cornea may reveal breaks in Descemet’s membrane (Haab’s striae), which is evidence for a raised intraocular pressure in early childhood (Fig. 18-2).
| Signs and Symptoms of Glaucoma |
|---|
| Light sensitivity |
| Pain |
| Epiphora |
| Irritability |
| Vomiting |
| Cloudy cornea |
| Corneal enlargement |
| Elevated pressure |
In addition to ocular signs and symptoms of glaucoma, secondary systemic abnormalities may occur and are especially common with acute glaucoma. Irritability, loss of appetite, and vomiting are seen and may be misunderstood before the ocular abnormality is recognized. Other systemic abnormalities may also provide information to help explain the cause of the pediatric glaucoma (Table 18-1).
I. Primary glaucomas A. Congenital open-angle glaucoma 1. Congenital 2. Infantile 3. Late recognized B. Autosomal dominant juvenile glaucoma C. Primary angle-closure glaucoma D. Associated with systemic abnormalities 1. Sturge-Weber syndrome 2. Neurofibromatosis (NF-1) 3. Stickler’s syndrome 4. Oculocerebrorenal (Lowe’s) syndrome 5. Rieger’s syndrome 6. Hepatocerebrorenal syndrome 7. Marfan syndrome 8. Rubinstein-Taybi syndrome 9. Infantile glaucoma associated with mental retardation and paralysis 10. Oculodentodigital dysplasia 11. Open-angle glaucoma associated with microcornea and absence of frontal sinuses 12. Mucopolysaccharidosis 13. Trisomy 13 14. Cutis marmorata telangiectasia congenita 15. Warburg syndrome 16. Kniest syndrome (skeletal dysplasia) 17. Michel’s syndrome 18. Nonprogressive hemiatrophy E. Associated with ocular abnormalities 1. Congenital glaucoma with iris and pupillary abnormalities 2. Aniridia a. Congenital glaucoma b. Acquired glaucoma 3. Congenital ocular melanosis 4. Sclerocornea 5. Iridotrabecular dysgenesis 6. Peters’ syndrome 7. Iridotrabecular dysgenesis and ectropion uveae 8. Posterior polymorphous dystrophy 9. Idiopathic or familial elevated episcleral venous pressure 10. Anterior corneal staphylom 11. Congenital microcoria with myopia 12. Congenital hereditary endothelial dystrophy 13. Congenital hereditary iris stromal hypoplasia II. Secondary glaucomas A. Traumatic glaucoma 1. Acute glaucoma a. Angle concussion b. Hyphema c. Ghost cell glaucoma 2. Late-onset glaucoma with angle recession 3. Arteriovenous fistula B. Secondary to intraocular neoplasm 1. Retinoblastoma 2. Juvenile xanthogranuloma 3. Leukemia 4. Melanoma 5. Melanocytoma 6. Iris rhabdomyosarcoma 7. Aggressive nevi of the iris C. Secondary to uveitis 1. Open-angle glaucoma 2. Angle-blockage glaucoma a. Synechial angle closure b. Iris bombe with pupillary block D. Lens-induced glaucoma 1. Subluxation-dislocation and pupillary block a. Marfan syndrome b. Homocystinuria 2. Spherophakia and pupillary block 3. Phacolytic glaucoma E. Secondary to surgery for congenital cataract 1. Lens material blockage of the trabecular meshwork (acute or subacute) 2. Pupillary block 3. Chronic open-angle glaucoma associated with angle defects F. Steroid-induced glaucoma G. Secondary to rubeosis 1. Retinoblastoma 2. Coats’ disease 3. Medulloepithelioma 4. Familial exudative vitreoretinopathy H. Secondary angle-closure glaucoma 1. Retinopathy of prematurity 2. Microphthalmos 3. Nanophthalmos 4. Retinoblastoma 5. Persistent hyperplastic primary vitreous 6. Congenital pupillary iris-lens membrane I. Glaucoma associated with increased venous pressure 1. Carotid or dural-venous fistula 2. Orbital disease J. Secondary to maternal rubella K. Secondary to intraocular infection 1. Acute recurrent toxoplasmosis 2. Acute herpetic iritis L. Ciliary block (malignant) glaucoma |
 Examination
Examination
Examination of children for glaucoma utilizes skills exercised in a complete pediatric eye examination. Prior to performing the ocular examination, it is necessary to obtain a detailed medical history. To perform the ocular examination, the examiner must have appropriate instruments and skill to perform the necessary assessments quickly and successfully. The examination of the young glaucoma patient will often be performed in both an office and an operating room setting under anesthesia (examination under anesthesia [EUA]).
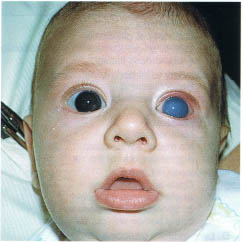
FIGURE 18-1. This 4-month-old developed sudden opacification of the left cornea, which was his first sign of congenital glaucoma. Bilateral corneal enlargement was also present.
| Examination Instruments for Glaucoma |
|---|
| Focused flashlight |
| Hand-held slit lamp |
| Hand-held tonometer |
| Indirect ophthalmoscope |
| 10 and 14D indirect lenses |
| Binocular loupe |
| Direct ophthalmoscope |
| Scleral transilluminator |
| Koeppe lens Barkan viewing scope |
The examination should begin with an estimate of vision (see Chapter 2). Is nystagmus present? Is there unusual avoidance of light? Strabismus? Pupillary reactivity should be noted. (This may be difficult if the corneas are cloudy or if the pupils are formed abnormally.) When possible, older children should have formal visual field testing.
| Pediatric Glaucoma Examination |
|---|
| History |
| Observation for light sensitivity |
| Vision assessment |
| Anterior segment examination |
| Cornea |
| Anterior chamber |
| Iris |
| Pupil |
| Lens assessment |
| Fundoscopy |
| Gonioscopy |
| Tonometry |
| Ultrasonography |
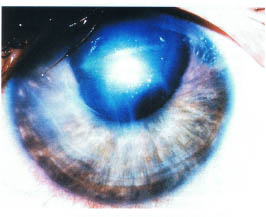
FIGURE 18-2. The cornea of this child with infantile glaucoma shows a central vertical break in Descemet’s membrane associated with curvilinear peripheral corneal breaks.
Inspection of the Anterior Segment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


