 Questions
Questions
1. Which of the following factors does not play a role in determining IOP?
a. rate of aqueous humor production by the ciliary body.
b. resistance to aqueous outflow across the trabecular meshwork-Schlemm’s canal system.
c. level of intracranial pressure.
d. level of episcleral venous pressure.
2. Glaucoma is defined as
a. a group of diseases that have in common a characteristic optic neuropathy associated with increased intraocular pressure.
b. a group of diseases that have in common a characteristic optic neuropathy with associated visual function loss.
c. a group of diseases that have in common high intraocular pressure with or without optic neuropathy.
d. a group of diseases that have in common a characteristic optic neuropathy with poor visual acuity.
3. Which of the following epidemiologic statistics is true regarding primary open angle glaucoma?
a. In the United States, it is the most frequent cause of nonreversible blindness in African Americans.
b. By the year 2020, it is estimated that 2.2 million Americans will be affected.
c. It is estimated that 10% have become bilaterally blind (best-corrected visual acuity ≤20/200 or visual field <20°).
d. Data from meta-analysis tends to overestimate the prevalence.
4. Which of the following is true in regard to worldwide racial disparity and primary open angle glaucoma?
a. Prevalence among blacks is three to four times higher than whites.
b. The racial disparity decreases with age.
c. In general, blacks have been found to have fewer nerve fibers at baseline.
d. Despite the higher prevalence in blacks, the likelihood of blindness is four times lower when compared to whites.
5. Which of the following is not a risk factor for the development of primary open angle glaucoma?
a. positive family history.
b. advanced age.
c. increased IOP.
d. increased corneal thickness.
6. Intraocular pressure can fluctuate throughout the day. Peak IOP occurs
a. upon awakening.
b. midday.
c. late evening.
d. during the night.
7. With respect to angle-closure glaucoma, which of the following is true?
a. Men are at increased risk.
b. The anterior chamber depth increases with age, predisposing to pupillary-block- induced angle-closure glaucoma.
c. Primary angle-closure glaucoma may occur in eyes with any type of refractive error.
d. Family history, while important in open-angle glaucoma, does not play a role in angle-closure glaucoma.
8. Which of the following gene mutation-phenotype pairings is incorrect?
a. GLC1A—associated with myocilin production in the trabecular meshwork after treatment with dexamethasone in both juvenile and adult forms of glaucoma.
b. GLC1B—associated with normal-tension forms of open-angle glaucoma.
c. GLC1C—associated with high pressure, late onset forms of glaucoma.
d. GLC1D—associated with a protein that catalyzes the formation of elastin fibers in exfoliation syndrome.
9. Several investigators have provided evidence that a gene responsible for some cases of juvenile-onset primary open-angle glaucoma resides on chromosome
a. 1.
b. 3.
c. 8.
d. X.
10. Which of the following is true in regard to aqueous humor dynamics?
a. Aqueous humor is produced in the anterior chamber and flows through the pupil.
b. Aqueous humor is produced by the inner nonpigmented cells of the ciliary processes.
c. Aqueous humor exits the eye by passing through the trabecular meshwork and into Schlemm’s canal before draining into the suprachoroidal spaces.
d. Aqueous humor exits the eye by passing through the uveoscleral pathway that ultimately drains into the venous system through a plexus of collector channels.
11. Aqueous humor is not formed or secreted as a result of
a. facilitated diffusion.
b. simple diffusion.
c. active secretion.
d. ultrafiltration.
12. Relative to plasma, aqueous has all of the following except
a. excess hydrogen ions.
b. excess chloride ions.
c. excess ascorbate.
d. excess bicarbonate.
13. All of the following can decrease aqueous humor production except
a. trauma.
b. intraocular inflammation.
c. general anesthetics such as Ketamine.
d. carotid occlusive disease.
14. Which of the following is not true in regard to trabecular outflow?
a. It is increased by cycloplegia.
b. It is the site of pressure-dependent outflow.
c. The juxtacanalicular meshwork is likely the major site of outflow resistance.
d. The trabecular meshwork functions as a oneway valve, permitting aqueous to leave and limiting flow in the other direction.
15. Uveoscleral outflow accounts for what percentage of total aqueous outflow facility?
a. <5%.
b. 5% to 10%.
c. 10% to 50%.
d. 75% to 90%.
16. The mean value for outflow facility in normal eyes is
a. 0.05 mL/min/mm Hg.
b. 0.15 mL/min/mm Hg.
c. 0.28 mL/min/mm Hg.
d. 0.48 mL/min/mm Hg.
17. Episcleral venous pressure
a. is not affected by alterations in body position.
b. normally ranges from 10 to 12 mm Hg.
c. can be altered by certain diseases of the orbit, the head, and the neck that obstruct venous return to the heart or shunt blood from the arterial to the venous system.
d. is associated with a rise in IOP in a 1:1 fashion in chronic conditions.
18. Data from large western epidemiologic studies demonstrate that intraocular pressure has a
a. non-Gaussian distribution with a skew toward lower pressures.
b. non-Gaussian distribution with a skew toward higher pressures.
c. gaussian distribution centered at 16 mm Hg.
d. gaussian distribution centered at 22 mm Hg.
19. Which of the following regarding intraocular pressure is false?
a. Screening for glaucoma based on IOP > 21 misses half of people with glaucoma and optic nerve damage.
b. There is no clear IOP level below which IOP can be considered safe and above which IOP can be considered elevated.
c. IOP is no longer considered a risk factor for the development of glaucoma.
d. IOP varies with heartbeat, respiration, and exercise.
20. Regarding Goldmann applanation tonometry:
a. The tonometer measures the force necessary to flatten a 3.06 mm2 area of cornea.
b. Measurements are most accurate with a central corneal thickness of 520 mm.
c. Excessive amounts of fluorescein result in inaccurately low IOP readings.
d. Corneal edema predisposes to inaccurately high IOP readings.
21. Which of the following findings was not reported in the Ocular Hypertension Treatment Study (OHTS)?
a. A thinner central cornea was a strong predictive factor for the development of glaucoma in subjects with ocular hypertension.
b. Subjects with a corneal thickness of 555 mm or less had a threefold greater risk of developing POAG when compared to those measuring >588 mm.
c. Central corneal thickness was found to be a risk factor for progression independent of IOP level.
d. More than four times as many subjects progressed to glaucoma in the observation group compared to those that were treated.
22. Current recommendations for cleaning Goldman-type tonometry tips between patients include all of the following except
a. 5 minutes soak in 40% isopropyl alcohol.
b. 5 minutes soak in 1:10 sodium hypochlorite solution (household bleach).
c. 5 minutes soak in 3% hydrogen peroxide.
d. Thorough wipe with an alcohol sponge.
23. Which of the following is incorrect in regard to gonioscopy?
a. Under normal conditions light reflected from the angle structures undergoes total internal reflection at the tear–air interface.
b. All gonioscopy lenses eliminate tear-air interface by placing a plastic or glass surface on the front surface of the eye while the space between the lens and cornea is filled by tears, saline, or a clear viscous substance.
c. The Goldmann lens is a type of direct viewing system.
d. The Zeiss lens is a type of mirrored, indirect viewing system.
24. Which of the following gonioscopy lenses would most likely narrow the angle on indentation gonioscopy?
a. Goldmann.
b. Posner.
c. Sussman.
d. Zeiss.
25. Which method of gonioscopy is considered best for evaluating a patient with potential traumatic (angle-recession) glaucoma?
a. Goldmann.
b. Koeppe.
c. Zeiss.
d. Sussman.
26. Which of the following is least likely to undergo spontaneous closure?
a. grade I angle.
b. grade II angle.
c. grade III angle.
d. grade IV angle.
27. The gonioscopic criteria for posttraumatic angle recession include all of the following except
a. an abnormally wide ciliary body band.
b. decreased prominence of the scleral spur.
c. torn iris processes.
d. marked variation of ciliary face width and angle depth in different quadrants of the same eye.
28. The adult optic nerve
a. is composed of neural tissue, glial tissue, extracellular matrix, and blood vessels.
b. consists of approximately 6 million axons.
c. has axons with cell bodies that lie in the bipolar layer of the retina.
d. expands from 1 to 2 mm in diameter upon exiting the globe.
29. The lamina cribrosa is made up of fenestrated sheets of connective tissue. Which of the following is incorrect regarding this structure?
a. It provides the main support for the optic nerve as it exits the eye.
b. The connective tissue is composed primarily of collagen.
c. The fenestrations within the lamina are larger temporally and nasally as compared with superior and inferior aspects.
d. The fenestrations may be seen on exam at the base of the optic nerve head cup.
30. There is a rich vascular supply to the optic nerve, retina, and choroid. Which of the following is a true statement?
a. The long posterior ciliary arteries penetrate the perineural sclera of the posterior globe to supply the peripapillary choroid, as well as most of the anterior optic nerve.
b. Some long posterior ciliary arteries course, without branching, through the sclera directly into the choroid; others divide within the sclera to provide branches to both the choroid and the optic nerve.
c. The central retinal artery penetrates the globe 3 to 5 mm behind the globe.
d. A noncontinuous arterial circle exists within the perineural sclera, known as the circle of Zinn-Haller, and is not found in all eyes.
31. There are four anatomic regions of the anterior optic nerve. Which of the following regions is incorrectly associated with a blood supply?
a. Superficial nerve fiber layer—supplied principally by recurrent retinal arterioles from the central retinal artery.
b. Prelaminar region—supplied by branches of short posterior ciliary arteries and branches of the circle of Zinn-Haller.
c. Lamina cribrosa region—supplied by branches of short posterior ciliary arteries and branches of the circle of Zinn-Haller.
d. Retrolaminar region—supplied solely by branches of short posterior ciliary arteries.
32. The mechanical theory of glaucomatous optic neuropathy emphasizes all of the following concepts except
a. direct compression of axonal fibers and support structures of the anterior optic nerve.
b. distortion of the lamina cribrosa plates and axoplasmic flow.
c. intraneural ischemia from decreased optic nerve perfusion.
d. cell death of the retinal ganglion cells from compression of axons.
33. What percentage of normal individuals will have cup–disc ratios of larger than 0.6?
a. <1%.
b. 5%.
c. 10%.
d. 25%.
34. Asymmetry of cup–disc ratio of more than 0.2 occurs in what percentage of the normal population?
a. <1%.
b. 5%.
c. 10%.
d. 25%.
35. In normal eyes, on average, _____ neuroretinal rim is thickest, while _____ rim is thinnest.
a. inferior, superior.
b. inferior, temporal.
c. temporal, inferior.
d. superior, inferior.
36. Which of the following is true with regard to splinter, or nerve fiber layer, hemorrhages near the optic nerve?
a. They may occur in as many as half of glaucoma patients at some time during the course of their disease.
b. Hemorrhages clear over weeks to months but are often followed by localized notching of the rim and visual field loss.
c. Individuals with normal-tension glaucoma are less likely to have disc hemorrhages.
d. They are pathognomonic for glaucoma.
37. Which of the following is not a characteristic of short-wavelength automated perimetry (SWAP)?
a. A blue stimulus is projected onto a yellow background.
b. This method is sensitive in early identification of glaucomatous damage.
c. The rate of perimetric change from early glaucoma may be higher than with conventional white-on-white visual fields.
d. The stimuli employed activate the M cells.
38. Which of the following is not true regarding visual field testing?
a. A cluster of two or more points depressed ≥5 dB compared with surrounding points is suspicious.
b. A single point depressed >10 dB is very unusual but is of less value on a single visual field than a cluster, because cluster points confirm one another.
c. Corresponding points above and below the horizontal midline should not vary markedly.
d. Normally the inferior field is depressed 1 to 2 dB compared with the superior field.
39. Which one of the following statements concerning perimetry is true?
a. In static perimetry, the stimulus intensity is held constant (static) and moved centrally until it is detected.
b. Kinetic perimetry is most useful for quantifying and tracking visual field changes in a patient with established glaucoma.
c. Early, specific signs of glaucoma include generalized constriction of isopters and baring of the blind spot.
d. For a visual field defect to be classified as glaucomatous, it should have corresponding optic nerve head abnormalities.
40. A 64-year-old African American man with a history of open-angle glaucoma presents with a Goldmann visual field documenting a superior nasal step to the I4e isopter in the right eye. When he returns with a deteriorated visual field 1 year later, the most likely form of deterioration is
a. an inferior Bjerrum scotoma.
b. a superior paracentral scotoma.
c. an inferior nasal step.
d. encroachment of his superior nasal step toward fixation.
41. Which one of the following visual field patterns will most quickly progress to loss of fixation?
a. split fixation to the I4e isopter.
b. central 5° island.
c. a large superior nasal step encroaching on fixation (<10°).
d. superior and inferior nasal steps encroaching to 20°.
42. When should other neurologic etiologies, other than glaucoma, be strongly considered?
a. The patient’s optic disc cupping is proportional to visual field loss.
b. The cupping of the nerve is more impressive than the pallor.
c. The progression of the visual field loss seems excessive.
d. The pattern of visual field loss respects the horizontal midline.
43. What percent of individuals in the general population who have glaucomatous optic neuropathy and/or visual field loss have an initial screening IOP of below 22 mm Hg?
a. 70% to 80%.
b. 30% to 50%.
c. 10% to 30%.
d. <10%.
44. Which of the following was not a finding in the Ocular Hypertension Treatment Study (OHTS)?
a. The purpose of the study was to evaluate the safety and efficacy of topical ocular hypotensive medications in preventing or delaying the onset of visual field loss and/or optic nerve damage in subjects with ocular hypertension.
b. Topical ocular hypotensive medication was effective in delaying or preventing the onset of POAG: a 22.5% decrease in IOP in the treatment group (vs. 4.0% in controls) was associated with a reduction of the development of POAG from 9.5% in controls to 4.4% in treated patients at 60 months’ follow-up.
c. OHTS subjects had thinner corneas than the general population, with black subjects having thinner corneas than white subjects.
d. Increased risk of onset of POAG was associated with increases in age, vertical and horizontal cup–disc ratio, pattern standard deviation, and IOP at baseline.
45. Which of the following was a finding in the Early Manifest Glaucoma Trial (EMGT)?
a. Treatment reduced IOP by 30%.
b. In multivariate analyses, progression risk was halved by treatment.
c. Progression risk decreased by 20% with each millimeter of mercury of IOP reduction from baseline to the first follow-up visit.
d. At 6 years, 62% of untreated patients showed progression, whereas 30% of treated patients progressed.
46. The Collaborative Initial Glaucoma Treatment Study compared medical and surgical approaches to newly diagnosed open-angle glaucoma patients and demonstrated that
a. Early visual loss was greater in the medically treated group.
b. After 5 years, the surgically managed group had worse visual field outcomes.
c. IOP reduction in the surgical group averaged 17 to 18 mm Hg, whereas that in the medically treated group was 14 to 15 mm Hg.
d. The rate of cataract removal was greater in the surgically treated group.
47. Which of the following is true in regard to low-tension or normal-tension glaucoma?
a. Authorities have separated normal-tension glaucoma into two groups based on disc appearance: a senile sclerotic group and a focal ischemic group.
b. Visual field defects in POAG tend to be more focal, deeper, and closer to fixation, especially early in the course, compared with those commonly seen in normal-tension glaucoma.
c. When compared to those with POAG, the neuroretinal rim has been reported to be thinner, especially superiorly, in persons with normal-tension glaucoma.
d. The Collaborative Normal-Tension Glaucoma Study (CNTGS) found that lowering IOP by at least 20% reduced the rate of visual field progression from 35% to 12% in subjects with normal-tension glaucoma.
48. A 54-year-old white woman presents with glaucomatous optic nerve head changes in each eye and split fixation in her right eye, consistent with her disc findings. Review of her record documents that she has progressively lost visual field and neural rim tissue while running IOPs in the low teens. Gonioscopy has been documented as normal repeatedly. She is currently on maximal tolerated medical therapy and reports subjective decrease in vision in her right eye. A surgical intervention in the right eye is felt to be the next indicated maneuver. Which procedure might be the one of choice?
a. iridoplasty.
b. surgical peripheral iridectomy.
c. trabeculectomy.
e. cyclocryotherapy or cyclophotocoagulation.
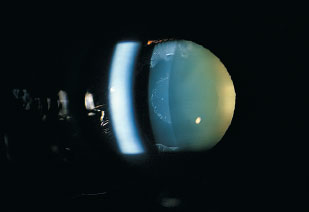
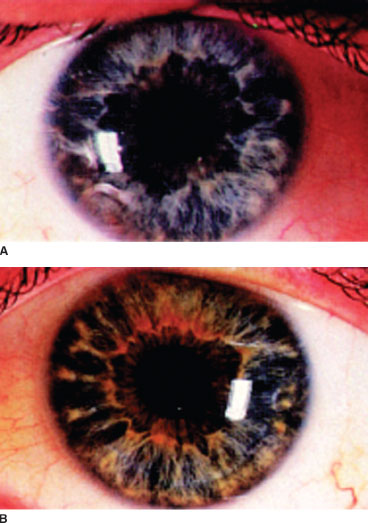
49. A 75-year-old Scandinavian woman presents for routine eye examination. She has no complaints. Her examination is significant for IOP of 23 in both eyes, anterior segment exam significant for findings as indicated by photograph below, and cup:disc ratio of 0.7 in both eyes. Which of the following is most likely true in regard to the remainder of her examination?
a. On gonioscopy, the trabecular meshwork is heavily pigmented with pigment deposition anterior to the Schwalbe line.
b. On gonioscopy, the chamber angle is narrow due to formation of synechiae.
c. On retroillumination, peripheral transillumination defects are seen.
d. On examination of the lens, she is noted to dilate widely with pigment visible on zonules.
50. In regard to the patient described in question 49, which of the following is least likely true?
a. The open-angle glaucoma associated with this condition is thought to be caused by material obstructing flow through, and causing damage to, the trabecular meshwork.
b. In this condition, IOP is often higher, with greater diurnal fluctuations than in POAG, and the overall prognosis is worse.
c. Laser trabeculoplasty can be very effective, but the response may not last as long as with POAG.
d. Lens extraction has a high likelihood of alleviating the condition.
51. Features that distinguish pseudoexfoliation glaucoma from primary open-angle glaucoma include all of the following except
a. greater sensitivity to laser therapy.
b. greater degree of interocular asymmetry.
c. the age of affected patients.
d. degree of trabecular meshwork (TM) pigmentation.
52. Which of the following glaucomas is least likely to respond to medical therapy alone?
a. pseudoexfoliation.
b. pigmentary glaucoma.
c. phacolytic glaucoma.
d. lens particle glaucoma.
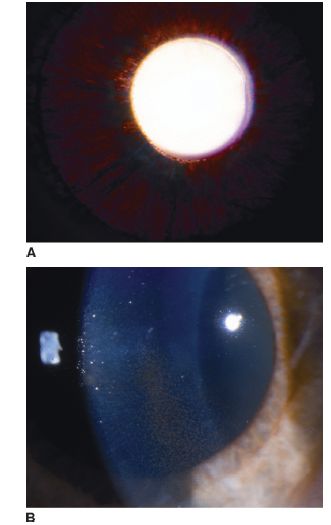
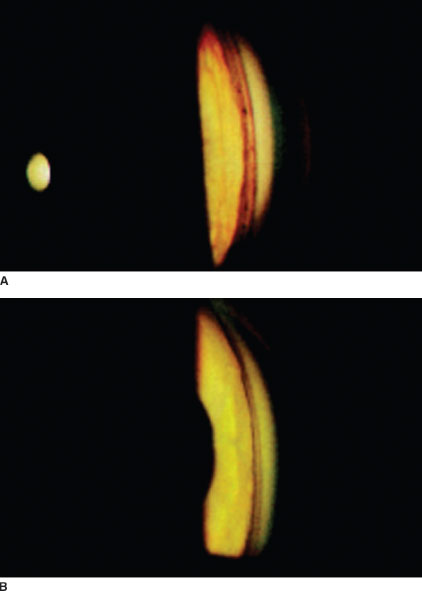
53. A patient presents with clinical findings as shown in the photographs A and B in the left column at the top of the next page. Which of the following statements is most applicable to this patient?
a. The risk of developing glaucoma is approximately 50% to 75%.
b. Glaucoma associated with these findings occurs most commonly in young black males who have high myopia.
c. Glaucoma associated with these findings is characterized by wide fluctuations in IOP which can exceed 50 mm Hg.
d. The presence of a Krukenberg’s spindle is necessary to make the diagnosis.
54. In regard to treatment options for the patient in question 53, which of the following is not true?
a. Medical treatment is often successful in reducing IOP.
b. Patients respond well to laser trabeculoplasty, although the effect may be short-lived.
c. Laser iridectomy has been proposed as a means of minimizing posterior bowing of the iris.
d. Filtering surgery is usually unsuccessful in these patients.
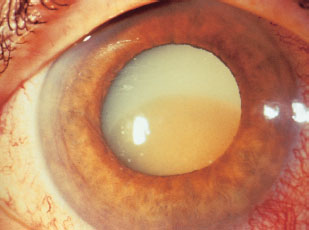
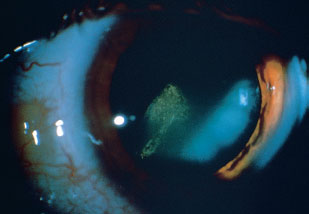
55. A 73-year-old male presents with sudden onset pain and redness in his right eye (see image in next column). His vision has been poor in the eye for 3 years. His only significant history is that he had cataract surgery in the fellow eye 4 years ago. There is no history of trauma. Clinical examination demonstrates markedly elevated IOP and an open angle. Which of the following is most likely true?
a. Keratic precipitates are often present in this condition.
b. Cellular debris may be seen layering in the anterior chamber, leading to a pseudohypopyon.
c. Definitive therapy requires laser iridotomy.
d. Leakage of lens protein occurs through large defects in the lens capsule.
56. The most common cause of glaucoma in primary or metastatic tumors of the ciliary body is
a. direct tumor invasion of the anterior chamber angle.
b. angle closure by rotation of the ciliary body.
c. angle closure by anterior displacement of the lens-iris diaphragm.
d. neovascularization of the angle.
57. Which of the following regarding glaucomatocyclitic crisis is not true?
a. The iritis associated with this entity is mild, with few small, round keratic precipitates (KP).
b. Chronic suppressive therapy with topical nonsteroidal anti-inflammatory agents or mild steroids is effective in preventing attacks.
c. KP may be seen on the trabecular meshwork, suggesting trabeculitis.
d. Intraocular pressure is usually markedly elevated, in the 40 to 50 mm Hg range, and corneal edema may be present.
58. What percent of patients with Fuchs heterochro-mic iridocyclitis will have a secondary open-angle glaucoma?
a. 15%.
b. 30%.
c. 50%.
d. 90%.
59. Which of the following is true in regard to treating glaucoma secondary to elevated episcleral venous pressure.
a. Medications that increase trabecular outflow are more effective than drugs that reduce aqueous humor formation.
b. Glaucoma filtering surgery may be complicated by a ciliochoroidal effusion or a supra-choroidal hemorrhage.
c. Prostaglandin analogs are not effective in any patients.
d. Laser trabeculoplasty is effective unless there are secondary changes in the outflow channels.
60. In a patient who presents with traumatic hyphema, elevated IOP, and a history of sickle cell disease, which of the following is safest to use for IOP reduction?
a. apraclonidine.
b. brimonidine.
c. epinephrine.
d. dipivefrin.
61. Which of the following is not true in regard to ghost cell glaucoma?
a. It is considered a secondary open-angle glaucoma caused by degenerated red blood cells blocking the trabecular meshwork.
b. The cells develop within 1 to 3 weeks of a vitreous hemorrhage.
c. The cells gain access to the anterior chamber through a disrupted hyaloids face.
d. Medical therapy with aqueous suppressants is the preferred initial approach.
62. The cells that are postulated to cause increased IOP in cases of retinal detachment (Schwartz-Matsuo syndrome) are
a. pigment.
b. inflammatory cells.
c. retinal pigment epithelium.
d. photoreceptor outer segments.
63. Which of the following ocular biometrics does not predispose to primary angle closure?
a. shallow anterior chamber.
b. thick lens.
c. increased anterior curvature of the lens.
d. large corneal diameter.
64. A 60-year-old Chinese woman presents with sudden onset pain, headache, blurred right eye vision, nausea, and vomiting. She reports that she had been watching a movie with her husband when these symptoms started and now describes rainbow- colored halos around lights. On examination of her right eye she has hand motions vision, intraocular pressure of 50, iris bombé, mid-dilated pupil, and corneal edema. Which of the following findings is least likely to be found on further evaluation of the eye?
a. mild aqueous cell and flare.
b. congested episcleral vessels.
c. retinal vascular occlusion.
d. anterior chamber depth of 2.6 mm.
65. In patient referenced in question 64, what is the best course of action at this time?
a. argon laser trabeculoplasty.
b. selective laser trabeculoplasty.
c. peripheral iridectomy.
d. trabeculectomy.
66. An untreated fellow eye in a patient who has had an acute angle-closure attack has a _____ chance of developing an acute attack of angle closure over the next 5 to 10 years.
a. 5% to 10%.
b. 15% to 35%.
c. 40% to 80%.
d. >90%.
67. Which of the following medications is least likely to be associated with the induction or aggravation of angle-closure glaucoma?
a. pilocarpine.
b. oral antihistamines.
c. cyclopentolate.
d. aspirin
68. A patient with bilaterally narrow anterior chamber angles and normal IOP should probably undergo which of the following tests?
a. the prone-dark room test.
b. topical steroid challenge.
c. thymoxamine test.
e. careful, depressed dilated examination.
69. A patient with bilaterally narrow anterior chamber angles and elevated IOP should probably undergo which of the following tests?
a. the prone-dark room test.
b. topical steroid challenge.
c. thymoxamine test.
e. careful, depressed dilated examination.
70. Which of the following clinical features is least likely to lead to a suspicion of plateau iris in a patient with angle closure?
a. deep anterior chamber centrally.
b. a young, myopic patient.
c. a flat iris plane.
d. a small anterior segment.
71. A 24-year-old myope presents with acute angle closure glaucoma. Examination reveals that the central anterior chamber appears to be of normal depth and the iris plane appears to be rather flat for an eye with angle closure. What entity is most likely to be found on gonioscopy?
a. plateau iris.
b. blood in Schlemm’s canal.
c. heavily pigmented trabecular mesh work.
d. neovascularization of the angle.
72. Angle closure secondary to plateau iris is most often secondary to what primary underlying anatomic derangement?
a. abnormally concave corneoscleral limbus.
b. abnormally thickened peripheral iris stroma.
c. forward displacement of the ciliary processes.
d. increased relative pupillary block.
73. Which of the following is true in regard to microspherophakia?
a. It is often familial and may occur as part of either Weill-Marchesani or Down’s syndrome.
b. It can lead to ectopia lentis.
c. Treatment with miotics may tighten zonules, flatten the lens, and pull it posteriorly, breaking pupillary block.
d. Cycloplegics may make pupillary block worse by rotating the ciliary body forward, loosening the zonule, and allowing the lens to become more globular.
74. What is the treatment of choice for neovascularization of the iris due to retinal ischemia in a patient with clear media?
a. observation.
b. panretinal photocoagulation.
c. panretinal cryotherapy.
d. vitrectomy with endophotocoagulation.
75. A 65-year old female with history of angle closure glaucoma in the past and pseudophakia presents 1 week after trabeculectomy. Her vision is hand motions, intraocular pressure is 50 and on exam she has a cloudy cornea and uniformly shallow anterior chamber. Of the following pathologies, which is least likely?
a. aqueous misdirection.
b. choroidal detachment.
c. acute angel-closure glaucoma.
d. suprachoroidal hemorrhage
76. In reference to the patient in question 75, her B-scan ultrasound demonstrates no choroidal pathology. What is the optimal management at this time if the patient has a patent peripheral iridotomy?
a. surgical iridectomy.
b. vitrectomy.
c. mydriatic and IOP lowering agents.
d. lensectomy.
77. Which of the following is true in regard to epithelial and fibrous downgrowth?
a. Epithelial downgrowth is more prevalent than fibrous ingrowth and progresses more rapidly.
b. The YAG laser produces characteristic white burns on the epithelial membrane on the iris surface that can help confirm the diagnosis of epithelial downgrowth as well as demarcate the extent of involvement.
c. The growth of epithelium or fibrovascular tissue into the angle can cause a secondary angle-closure glaucoma for which surgery is the preferred treatment.
d. Epithelial proliferation can be present in three forms: pearl tumors of the iris, epithelial cysts, and epithelial ingrowth.
78. A 46-year-old female with no prior ocular history presents with bilateral ocular pain, headaches, and worsening of vision. On examination she is noted to have a six diopter myopic shift, IOP of 60, and uniformly shallow anterior chamber in both eyes. What oral medication was she most likely started on recently?
a. isoniazid.
b. ethambutol.
c. topiramate.
d. clonazepam.
79. For the patient in question 78 what is the best initial treatment?
a. discontinuation of offending oral medication, IOP lowering agents, and laser peripheral iridotomy.
b. discontinuation of offending oral medication, IOP lowering agents, and surgical peripheral iridectomy.
c. discontinuation of offending oral medication, IOP lowering agents, and miotics.
d. discontinuation of offending oral medication, IOP lowering agents, and cycloplegics.
80. The underlying mechanism of the syndrome above is
a. ciliochoroidal effusion or detachment.
b. central serous retinopathy.
c. acute elongation of the globes.
d. pupillary block.
81. A mother states that her 6-month-old child has been tearing for the past month and feels that he may not see well with his right eye. Given the findings in the image below, what is the most likely diagnosis?
a. retinoblastoma.
b. congenital glaucoma.
c. nasolacrimal duct obstruction.
d. congenital hereditary endothelial dystrophy.

82. What is the optimal management for lowering IOP in a child with congenital glaucoma and a hazy cornea?
a. topical IOP lowering agents.
b. goniotomy.
c. trabeculotomy ab externo.
d. trabeculectomy or shunt procedure.
83. Which of the following IOP lowering agents should be avoided in children <3 years of age?
a. topical brimonidine.
b. topical timolol.
c. topical dorzolamide.
d. oral acetazolamide.
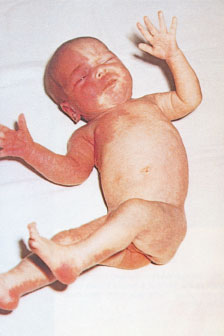
84. The infant pictured at the top of the next page presents with glaucoma; the mechanism leading to elevated IOP is most likely which of the following?
a. increased aqueous production.
b. elevated episcleral venous pressure.
c. congenital anterior chamber anomalies.
d. choroidal hemangioma leading to optic nerve cupping.
85. Which of the following syndromes is not associated with glaucoma?
a. Axenfeld-Rieger syndrome.
b. Sturge-Weber syndrome.
c. neurofibromatosis 1.
d. neurofibromatosis 2.
86. Which of the following pairings of medication and method of action is incorrect?
a. latanoprost: increase uveoscleral outflow.
b. timolol: decrease aqueous production.
c. brimonidine: decrease aqueous production, increase trabecular outflow.
d. dorzolamide: decrease aqueous production.
87. Which of the following pairings of medication and ocular side effects is incorrect?
a. latanoprost: increased pigmentation of iris, lashes, hypertrichosis.
b. timolol: corneal anesthesia, punctate keratitis.
c. brimonidine: blurring, dryness, eyelid edema.
d. dorzolamide: induced hyperopia, keratitis, dermatitis.
88. Which of the following pairings of medication and systemic side effects is incorrect?
a. latanoprost: flulike symptoms, joint or muscle pain, headache.
b. timolol: bradycardia, heart block, bron-chospasm, decreased libido, mood swings, reduced exercise tolerance.
c. brimonidine: fatigue, hypertension, syncope, dizziness, anxiety.
d. dorzolamide: depression, malaise, bitter taste.
89. Which of these is not a concern when using echothiophate iodide?
a. intense miosis.
b. retinal detachment.
c. angle closure.
d. dry mouth.
90. All glaucoma agents are considered class C during pregnancy except for one agent. Which of the following is considered a class B agent during pregnancy?
a. brimonidine.
b. pilocarpine.
c. timolol.
d. dorzolamide.
91. The proper pediatric dose of acetazolamide (Diamox) is
a. 15 mg/kg/day in one dose.
b. 15 mg/kg/day in three or four divided doses.
c. 5 mg/kg/day in one dose.
d. 5 mg/kg/day in three or four divided doses.
92. The agent most likely to cause topical sensitization and medicamentosa is
a. timolol.
b. betaxolol.
c. epinephrine.
d. pilocarpine.
93. Which of the following miotics is a direct-acting agent?
a. echothiophate.
b. carbachol.
c. demecarium.
d. pilocarpine.
94. Which of the following complications of miotic administration is least likely with the indirect agents?
a. cataractogenesis.
b. bradycardia.
c. punctal stenosis.
d. retinal tears and detachment.
95. The side effect of carbonic anhydrase inhibitors that is most commonly encountered is
a. paresthesias.
b. gastrointestinal distress.
c. kidney stones.
d. anemia.
96. A 73-year-old man reports to the office on his first day following a cataract extraction complaining of severe eye pain. Visual acuity is counting fingers at 3 ft in the involved eye. Slit-lamp examination reveals a diffusely shallow anterior chamber and corneal edema without hypopyon. The next step should be
a. dilated fundus examination.
b. tonometry.
c. gonioscopy.
d. B-mode ultrasonography.
97. In the patient referenced in question 96, after obtaining an applanation IOP of 42 mm Hg and attempting to examine the fundus unsuccessfully, ultrasonography is performed and reveals a normal posterior segment. Gonioscopy reveals a completely closed angle. The next intervention should be
a. surgical revision of the wound.
b. peripheral iridotomy.
c. dilation with potent cycloplegics.
d. medical treatment with potent miotics.
98. The intervention in question 97 fails. What is the next step?
a. surgical revision of the wound.
b. peripheral iridotomy.
c. dilation with potent cycloplegics.
d. medical treatment with potent miotics.
99. During initial laser trabeculoplasty for open angle glaucoma, what circumference of the tra-becular meshwork is usually treated?
a. 90°.
b. 180°.
c. 270°.
d. 360°.
100. The correct spot size for argon laser trabeculoplasty (ALT) is
a. 50 µm.
b. 100 µm.
c. 200 µm.
d. 500 µm.
101. When effective, laser trabeculoplasty is expected to lower intraocular pressure by what percent?
a. 10% to 15%.
b. 20% to 25%.
c. 30% to 40%.
d. 50%.
102. In which of the following patients is laser trabeculoplasty contraindicated?
a. primary open angle glaucoma.
b. pigmentary glaucoma.
c. exfoliation syndrome.
d. synechial angle closure.
103. What percentage of patients who undergo laser trabeculoplasty have a transient rise in intraocular pressure?
a. <1%.
b. 5%.
c. 10%.
d. 20%.
104. In regard to iridocorneoendothelial (ICE) syndromes, which of the following is not true?
a. They are almost always unilateral and affect women more frequently than men.
b. The degree of IOP elevation directly reflects the amount of angle synechialization.
c. In Chandler’s syndrome, there may be corneal edema with only modestly elevated or normal IOP.
d. Essential iris atrophy features stretch and atrophic iris holes with corectopia.
105. A 37-year-old man presents with gradual loss of vision affecting his right eye. His past medical and ocular histories are unremarkable. Visual acuity is 20/400 in the right eye and 20/15 in the left eye. The neuromuscular examination is normal. Slit-lamp examination reveals stellate keratic precipitates on the right corneal endothelium, along with a dense white cataract and “washed-out” appearing iris stroma, as shown in image A. There are trace cells in the aqueous. The left eye is normal (image B). IOPs are 32 in the right eye and 12 in the left eye. Gonioscopy of the right eye reveals prominent, engorged vessels that bridge the angle without synechiae. Gonioscopy of the left eye is normal. The right fundus cannot be clearly seen due to the cataract. Which one of the following is true regarding this patient?
a. There was probably an episode of intense intraocular inflammation affecting the right eye in the past.
b. Antibody titers to herpes zoster virus are likely to be elevated in serum and aqueous humor.
c. A classic sign of this disorder is hyphema occurring at the beginning of filtration surgery.
d. The glaucoma is due to typical rubeosis and secondary angle closure.
106. A 48-year-old man presents complaining of difficulty reading. Subjective refraction reveals +0.25 in both eyes, giving 20/15 in both eyes. During the completion of the routine examination, IOP is measured as 34 mm Hg in the right eye and 16 mm Hg in the left eye. Gonioscopy of the right eye is shown in image A and the left eye is shown in image B. The right optic nerve shows evidence of inferior rim excavation. Which one of the following regarding these findings is false?
a. This entity is more common in men.
b. The incidence and severity of the glaucoma in this condition are correlated with the extent of angle abnormalities.
c. Careful slit-lamp examination may reveal iris abnormalities in the right eye.
d. The same pathophysiologic process will usually affect the left eye within the next 3 to 5 years.
107. Which one of the following regarding antime-tabolite glaucoma therapy is false?
a. Mitomycin-C (MMC) directly interacts with DNA, blocking RNA and subsequent protein synthesis in all metabolically active cells.
b. The antiproliferative effects of MMC are generally more potent and longer-lasting than those of a comparable dose of 5-fluorouracil (5-FU).
c. Great care should be taken to ensure adequate exposure of the bleb wound edges to MMC in order to gain the maximal antifibrotic effect.
d. 5-FU is associated with a greater incidence of postoperative hypotony and surface-related complications than MMC.
108. Which of the following is not a risk factor for bleb-related endophthalmitis?
a. old age.
b. blepharitis.
c. male gender.
d. nasolacrimal duct obstruction.
109. Which of the following is true in regard to the adult lens?
a. It typically measures 9 mm equatorially and 5 mm anteroposteriorly.
b. The relative thickness of the cortex decreases with age.
c. The lens adopts an increasingly flat shape with age.
d. The index of refraction increases with age.
110. The lens capsule is made of a transparent basement membrane composed of what type of collagen?
a. type I.
b. type II.
c. type III.
d. type I V.
111. What is the thickness of the lens capsule at the central posterior pole?
a. 2 to 4 µm.
b. 8 to 10 µm.
c. 12 to 15 µm.
d. 18 to 20 µm.
112. What enzyme has been found to play a pivotal role in the development of “sugar” cataracts that can occur in diabetics?
a. hexokinase.
b. polyol dehydrogenase.
c. aldose reductase.
d. glucose-6-phosphatase.
113. When the ciliary muscle contracts, the diameter of the muscle ring is
a. reduced, relaxing tension on the zonules, allowing the lens to become more spherical.
b. increased, relaxing tension on the zonules, allowing the lens to become more spherical.
c. reduced, increasing tension on the zonules, allowing the lens to become less spherical.
d. increased, increasing tension on the zonules, allowing the lens to become less spherical.
114. Anterior lenticonus can be found in association with what syndrome?
a. Alport’s syndrome.
b. Down’s syndrome.
c. Edwards’ syndrome.
d. Patau’s syndrome.
115. Lens colobomas are typically located in which quadrant?
a. superior.
b. inferior.
c. nasal.
d. temporal.
116. Patients with Peters’ anomaly may display which of the following lens anomalies?
a. posterior cortical or polar cataract.
b. adhesion between the lens and retina.
c. a misshapen lens displaced anteriorly into the pupillary space.
d. macrospherophakia.
117. Approximately what percentage of congenital cataracts are a component of a more extensive syndrome or disease?
a. 10%.
b. 33%.
c. 50%.
d. 75%.
118. Of the congenital and infantile cataracts, which type is the most common?
a. lamellar.
b. anterior polar.
c. posterior polar.
d. cerulean.
119. Which of the following statements is true in regard to congenital rubella syndrome and lens changes?
a. Cataract and glaucoma are often found simultaneously.
b. Live virus particles may be recovered from the lens as late as 3 years after the patient’s birth.
c. Excessive postoperative inflammation is very rare after cataract removal.
d. Lens changes are most often characterized by blue nuclear opacifications.
120. Dilated examination reveals a dense white spot on the vitreal surface of the posterior capsule just inferonasal to the center of the posterior capsule. The patient should be advised that
a. Cataract formation with visual loss is imminent.
b. The patient should have a glucose tolerance test immediately.
c. The patient should have urinalysis performed to detect hematuria and proteinuria.
d. The patient has a benign finding with no significant implications.
121. Which of the following is the histopathological description of the cataract shown at the top of next column?
a. increased number of lamellar membrane whorls.
b. local swelling and disruption of lens fiber cells.
c. collection of crystals on the inner surface of the posterior capsule.
d. posterior migration of the lens epithelial cells from the lens equator.
122. Which of the following drugs is correctly matched with the lens changes it classically causes?
a. phenothiazines: small vacuoles within the anterior lens capsule and epithelium.
b. miotics: pigmented deposition in the anterior lens epithelium.
c. amiodarone: stellate anterior axial pigment deposition.
d. statins: posterior subcapsular cataracts.
123. An infant presents to clinic with bilateral oil droplet cataracts. Mom notes that the child has appeared yellow and is not feeding well. Once the diagnosis is confirmed, how should this child be systemically managed?
a. elimination of milk and milk products from the diet.
b. enzyme replacement therapy.
c. penicillamine.
d. liver transplant.
124. A patient presents with red, painful eye 2 weeks after significant blunt trauma. On exam, sig-nificant cell and flare with keratic precipitates are noted along with increased intraocular pressure, cataract, and disruption of the capsular surface. These findings are most likely representative of
a. phacoantigenic uveitis.
b. phacolytic glaucoma.
c. phacomorphic glaucoma.
d. Posner-Schlossman syndrome.
125. For the patient in question 124, histopathologic examination would demonstrate
a. rare white blood cells.
b. pigmented debris but no white blood cells.
c. macrophages with ingested lens proteins.
d. zonal granulomatous inflammation surrounding a breach of the lens capsule
126. For the patient in question 124, what is the definitive therapy for this condition?
a. topical or periocular steroids.
b. lens extraction.
c. systemic steroids.
d. topical intraocular pressure lowering agents.
127. What is the most common indication for cataract surgery?
a. glare.
b. visual acuity worse than 20/50.
c. patient’s desire for improved vision.
d. mature cataract.
128. After cataract surgery, corneal edema may occur in the immediate postoperative period. Epithelial edema in the face of a compact stroma immediately after surgery is likely due to which of the following?
a. prolonged surgery.
b. inflammation.
c. small retained nuclear fragments in the angle.
d. elevated IOP with an intact endothelium.
129. Epithelial downgrowth is a rare complication of intraocular surgery, occurring less frequently with modern cataract surgery techniques. How should diagnosis be confirmed?
a. surgical sampling of membrane.
b. anterior segment OCT.
c. ultrasound biomicroscopy.
d. Argon laser application to demonstrate white burn formation.
130. A 77-year-old female presents 12 hours after cataract surgery with pain, redness, and photophobia in the operated eye. On exam she is found to have 20/400 vision with marked anterior chamber reaction and trace hypopyon. Which detail in the history above favors a diagnosis of Toxic Anterior Segment Syndrome (TASS) over infectious endophthalmitis?
a. the age of the patient.
b. the timing of the findings.
c. the level of vision.
d. the amount of anterior chamber reaction.
131. During cataract surgery, the surgeon notices that the patient’s pupil dilates poorly and undulates in response to intraocular irrigation. What medication is this patient likely on?
a. tamoxifen.
b. tamsulosin.
c. tacrolimus.
d. flonase.
132. Which is not recommended in the event of posterior capsular rupture during cataract surgery?
a. anterior vitrectomy to avoid vitreous prolapse.
b. insertion of IOL when safe and indicated.
c. careful removal of fragments that are not visible.
d. watertight closure of incisions.
133. Which of the following lenses has the lowest likelihood of posterior capsular opacification (PCO)?
a. silicone lens with round edge.
b. silicone lens with square edge.
c. acrylic lens with round edge.
d. acrylic lens with square edge.
134. A patient with history significant for deep vein thrombosis is brought to the operating room in preparation for cataract surgery. A retrobulbar injection is performed, and soon after the injection the orbit is taut with marked proptosis, elevated IOP, and significant ecchymosis of the lids and conjunctiva. What is the most likely complication of the retrobulbar injection at this time?
a. globe penetration.
b. retrobulbar hemorrhage.
c. inadvertent intradural injection.
d. inadvertent intravenous injection.
135. In the patient described in question 134, which of the following is not considered a potential maneuver to counteract the complication described?
a. topical IOP lowering agents.
b. anterior chamber paracentesis.
c. lateral canthotomy and cantholysis.
d. extracapsular cataract extraction.
136. Which of the following is not a risk factor for the development of suprachoroidal hemorrhage during cataract surgery?
a. hyperopia.
b. hypertension.
c. glaucoma.
d. chronic intraocular inflammation.
137. A 75-year-old gentleman presents with pain, photophobia, and worsening vision 3 days after uneventful cataract surgery. His vision is found to be light perception and clinical findings as depicted in the image below. Which of the following is indicated for this patient?
a. management with topical antibiotics and steroids.
b. systemic fourth generation fluoroquinolones.
c. vitreous tap with injection of intravitreal antibiotics.
d. pars plana vitrectomy with intravitreal antibiotics.

138. The crystalline lens is derived from which embryonic tissue?
a. ectoderm.
b. endoderm.
c. mesoderm.
d. neural crest.
139. A patient presents after filtering surgery with a large filtering bleb and a shallow anterior chamber. Which of the following is the most likely diagnosis?
a. bleb leak.
b. overfiltration.
c. pupillary block.
d. aqueous misdirection.
140. Which of the following organisms is the most common cause of bleb-associated endophthalmitis?
a. Bacillus cereus.
b. Streptococcus species.
c. Coagulase negative Staphylococcus.
d. Haemophilus influenzae.
 Answers
Answers1. c. The Goldmann equation summarizes the relationship between many of these factors and the intraocular pressure (IOP) in the undisturbed eye
Po = (F / C) + Pv
where P0 is the IOP in millimeters of mercury (mm Hg), F is the rate of aqueous formation in microliters per minute (μL/min), C is the facility of outflow in microliters per minute per millimeter of mercury (μL/min/mm Hg), and P is the episcleral venous pressure in millimeters of mercury. Resistance to outflow (R) is the inverse of facility (C).
1. c. The Goldmann equation summarizes the relationship between many of these factors and the intraocular pressure (IOP) in the undisturbed eye:
2. b. While intraocular pressure is one of the primary risk factors for glaucoma, its presence or absence does not have a role in the definition of the disease.
3. a. The estimated prevalence of POAG in the United States in individuals older than 40 years is 1.86%. This translates to nearly 2.22 million Americans affected in the year 2000. Three to five percent have become bilaterally blind. The number of POAG patients is estimated to increase by 50% to 3.36 million in 2020. This number may be an underestimate, since visual field loss is required in the definition of POAG, and many individuals have glaucoma without documented visual field loss. POAG is the most frequent cause of nonreversible blindness in African Americans.
4. a. Among whites aged 40 years and older, a prevalence of between 1.1% and 2.1% has been reported based on population-based studies performed throughout the world. The prevalence among blacks is three to four times higher, with at least four times the likelihood of blindness. This racial disparity increases with age, with the likelihood of blindness from POAG increasing to 15 times higher for blacks in the age group 46 to 65 years. Blacks have larger discs and more nerve fibers; it has been hypothesized that the increased disc size is associated with increased mechanical strain in the region of the optic nerve.
5. d. Besides increased IOP, factors known to be associated with an increased risk for the development of glaucoma include advanced age, decreased corneal thickness, racial background, and a positive family history.
6. d. Current evidence suggests that peak IOP occurs during the night and is therefore, not caught on routine diurnal testing. The nocturnal rise may be due to variations in body position, and it has been suggested that measurement of supine IOP during office visits may approximate this nocturnal peak.
7. c. Women are at higher risk, likely due to shallower anterior chambers when compared to men. The anterior chamber decreases in depth and volume with age, which predisposes to pupillary block. Anterior chamber depth and volume are smaller in hyperopic eyes. Although PACG may occur in eyes with any type of refractive error, it is typically associated with hyperopia. Some of the anatomic features of the eye that predispose to pupillary block, such as more forward position of the lens and greater than average lens thickness, are inherited. Thus, relatives of subjects with angle-closure glaucoma are at greater risk of developing angle closure than is the general population.
8. d. Exfoliation syndrome is associated with the LOXL1 gene. The glaucoma associated with GLC1D resembles high-pressure POAG. The other associations are correct.
9. a. This form of the disease is characterized by markedly elevated pressures, often greater than 40 mm Hg, and poor response to medication. Other cloned genes known to be associated with glaucoma include PAX6 (11p13, aniridia), CYP1B1 (2p21, congenital glaucoma), PITX2 (4q25, Axenfeld-Rieger syndrome), LMX1B (9q34, glaucoma associated with nail-patella syndrome).
10. b. Aqueous humor is produced in the posterior chamber and flows through the pupil into the anterior chamber. Aqueous exits the eye by passing through the trabecular meshwork and into Schlemm’s canal before draining into the venous system through a plexus of collector channels, as well as through the uveoscleral pathway, which is proposed to exit through the root of the iris and the ciliary muscle, into the suprachoroidal spaces and through the sclera. The inner nonpigmented epithelial cells, which protrude into the posterior chamber, contain numerous mitochondria and microvilli; these cells are thought to be the actual site of aqueous production.
11. a. Active secretion, or transport, consumes energy to move substances against an electrochemical gradient and is independent of pressure; it accounts for the majority of aqueous production and involves, at least in part, activity of the enzyme carbonic anhydrase II. Ultrafiltration refers to a pressure-dependent movement along a pressure gradient. In the ciliary processes, the hydrostatic pressure difference between capillary pressure and IOP favors fluid movement into the eye, whereas the oncotic gradient between the two resists fluid movement. Diffusion is the passive movement of ions across a membrane related to charge and concentration.
12. d. Aqueous humor has an excess of hydrogen and chloride ions, an excess of ascorbate, and a deficit of bicarbonate relative to plasma.
13. c. Aqueous humor production may decrease following trauma or intraocular inflammation and following the administration of certain drugs, such as general anesthetics and some systemic hypotensive agents. Ketamine is a general anesthetic that is associated with a rise in intraocular pressure. Carotid occlusive disease may also decrease aqueous humor production.
14. a. Uveoscleral outflow, not trabecular outflow, is increased by cycloplegia. Trabecular outflow is increased by miotics.
15. c. Estimates of this value vary significantly. Most widely accepted estimates range from 15% to 20% with some being as low as 10%, and some as high as 50%. Uveoscleral outflow is pressure-independent.
16. c. Outflow facility in normal eyes ranges from 0.22 to 0.28 mL/min/mm Hg, and decreases with age, ocular surgery, and trauma. Glaucoma patients often have decreased outflow facility.
17. c. Episcleral venous pressure changes are associated with alterations in body position and with certain diseases of the orbit, the head, and the neck that obstruct venous return to the heart or shunt blood from the arterial to the venous system. The usual range of values is 8 to 10 mm Hg. In acute conditions, according to the Goldmann equation, IOP rises approximately 1 mm Hg for every 1 mm Hg increase in episcleral venous pressure. The relationship is more complex and less well understood, however, in chronic conditions. Chronic elevations of episcleral venous pressure may be accompanied by changes in IOP that are of greater or less magnitude than predicted by the Goldmann equation.
18. b. Data from these studies demonstrated a mean IOP of 16 mm Hg, with a standard deviation of 3 mm Hg. IOP had a non-Gaussian distribution with a skew toward higher pressures, especially in individuals older than age 40.
19. c. Elevation of IOP is still seen as an important risk factor for the development of glaucoma. Although other risk factors affect an individual’s susceptibility to glaucomatous damage, IOP is the only one that can be effectively altered. IOP can vary with time of day, heartbeat, respiration, exercise, fluid intake, systemic medication, and topical medications.
20. b. The Goldmann applanation tonometer measures the force necessary to flatten an area of the cornea of 3.06 mm diameter. An excessive amount of fluorescein results in wide mires and an inaccurately high reading. Measurements are most accurate with a central corneal thickness of 520 mm; however, the accepted range of normal is between 537 and 554 mm. Increased corneal thickness may give an artificially high IOP measurement; decreased corneal thickness, an artifi-cially low reading. Corneal edema predisposes to inaccurate low readings, whereas pressure measurements taken over a corneal scar will be falsely high.
21. d. The last statement is false. OHTS included patients with IOP 24 to 32 mm Hg and randomized patients to observation or to the reduction of IOP by at least 20% by topical medications. 4.4% of patients that were treated progressed to optic nerve or visual field loss during a 5-year period. More than twice as many of the untreated observation group (9.5%) progressed.
22. a. A 5-minute soak of 70% isopropyl alcohol should be used.
23. c. Direct gonioscopy is performed with a binocular microscope, a fiber-optic illuminator or slit-pen light, and a direct goniolens, such as the Koeppe, Barkan, Wurst, Swan-Jacob, or Richardson lens. Indirect gonioscopy is more frequently used and utilizes Posner, Sussman, Zeiss, and Goldmann-type lenses.
24. a. The Posner, Sussman, and Zeiss lenses have a smaller area of contact than the Goldmann lens and about the same radius of curvature; pressure on the cornea may falsely open the angle with the first three lenses while narrowing the angle with the Goldmann-type lenses.
25. b. Koeppe gonioscopy is considered best for evaluating a patient with potential angle recession because this system allows easier comparison of one eye with the fellow eye, or one portion of the angle with another.
26. d. Grade IV describes a 45° angle between the surface of the trabecular meshwork and the iris while grade I describes a 10° angle. Thus, a grade IV angle is less likely to undergo spontaneous closure.
27. b. The criteria include an increased prominence of the scleral spur. Other findings on gonioscopy may include microhyphema, hypopyon, retained foreign body, iridodialysis, precipitates, pigmentation of lens equator, IOL haptics, ciliary body tumors.
28. a. The adult optic nerve consists of 1.2 to 1.5 million axons that have cell bodies located in the ganglion cell layer. The optic nerve head is 1.5 mm in diameter, and expands to 3 to 4 mm upon exiting the globe as the fibers become myelinated.
29. c. The fenestrations within the lamina are larger superiorly and inferiorly as compared with the temporal and nasal aspects of the optic nerve. It is possible that these differences play a role in the development of glaucoma.
30. d. The first two statements are true for the short posterior ciliary arteries, not the long posterior ciliary arteries. The central retinal artery penetrates the optic nerve at 10 to 15 mm behind the globe.
31. d. The prelaminar and laminar regions have similar blood supplies. The retrolaminar region is supplied by the short posterior ciliary arteries as well as the pial arterial branches coursing adjacent to the retrolaminar optic nerve region.
32. c. Two hypotheses have emerged to explain the development of glaucomatous optic neuropathy, the mechanical and ischemic theories. The mechanical theory stresses the importance of direct compression of the axonal fibers, distortion of the lamina cribrosa plates, and interruption of axoplasmic flow, resulting in the death of the RGCs. The ischemic theory focuses on intraneu-ral ischemia resulting from decreased optic nerve perfusion. This perfusion may result from the stress of IOP on the blood supply to the nerve or from processes intrinsic to the optic nerve.
33. b. Five percent of normal individuals will have cup–disc ratios of greater than 0.6.
34. a. Less than 1% of normal individuals have an asymmetry of >0.2.
35. b. A convention referred to as the ISNT rule may be useful in identifying thinning of the neu-roretinal rim. In general, the Inferior neuroretinal rim is the thickest, followed by the Superior rim, the Nasal rim, and finally the Temporal rim. If the rim widths do not follow this progression, there should be increased concern for the presence of focal loss of rim tissue.
36. b. Disc hemorrhages may occur in as many as one-third of glaucoma patients at some time during the course of their disease. Individuals with normal-tension glaucoma are more likely to have disc hemorrhages. Optic disc hemorrhage is an important prognostic sign for the development or progression of visual field loss, and any patient with a splinter hemorrhage requires detailed evaluation and follow-up. These hemorrhages are not pathognomonic as they may be caused by posterior vitreous detachments, diabetes mellitus, branch retinal vein occlusions, and anticoagulation therapy.
37. d. Frequency-doubling technology (FDT) is believed to activate M cells.
38. d. Normally the superior field is depressed 1 to 2 dB compared with the inferior field.
39. d. If a patient has glaucomatous visual field–type defects, corresponding optic nerve head abnormalities should exist. Otherwise, alternative etiologies should be considered. In static perim-etry, the stimulus is of variable intensity and is kept stationary (static) until it is noticed by the patient. Baring of the blind spot and generalized constriction are not very specific and can be produced by miosis, uncorrected refractive error, aging, and cataract.
40. d. Areas of retina and/or optic nerve damaged by glaucoma are believed to be more vulnerable to ongoing damage at lower IOPs. Thus, field defects tend to become more severe with time. New defects also may appear, of course, but generally accompany progression of previous defects.
41. a. Split fixation is the presence of visual field loss that comes close to fixation. A typical pattern of progression is (a) loss near fixation (paracentral scotoma) to (b) split fixation to (c) loss of fixation. Thus, the eye at greatest risk is not one with a 5° central field but one with split-fixation in the horizontal meridian.
42. c. Other neurologic etiologies of field loss should be explored when the patient’s optic disc seems less cupped than would be expected for the degree of visual field loss; pallor of the disc is more impressive than cupping; progression of field loss seems excessive; pattern of field loss respects the vertical midline; and location of cupping or thinning does not correspond to proper location of field defect.
43. b. Several studies have indicated that as many as 30% to 50% of individuals in the general population who have glaucomatous optic neuropathy and/or visual field loss have initial screening IOPs below 22 mm Hg.
44. c. OHTS subjects had thicker corneas than the general population, with black subjects having thinner corneas than white subjects.
45. b. At 6 years, 62% of untreated patients showed progression, whereas 45% of treated patients progressed. Treatment reduced IOP by 25%. Risk factors for progression included no treatment, age, higher IOP, exfoliation, more severe visual field defect, and bilateral glaucoma. In multivariate analyses, progression risk was halved by treatment. Progression risk decreased by 10% with each mm HG of IOP reduction from baseline to the first follow-up visit.
46. d. Early visual loss was greater in the surgically treated group, but after 5 years both groups had similar visual field outcomes. IOP reduction in the medical group averaged 17 to 18 mm Hg, whereas that in the surgically managed group was 14 to 15 mm Hg.
47. a. Visual field defects in normal-tension glaucoma tend to be more focal, deeper, and closer to fixation compared with those commonly seen in normal-tension glaucoma. When compared to those with POAG, the neuroretinal rim has been reported to be thinner, especially inferiorly and inferotemporally. CNTGS found that lowering IOP by 30% reduced the rate of visual field progression from 35% to 12% in subjects with normal-tension glaucoma.
48. c. Given the extent of the glaucomatous damage as indicated by split fixation and progression of both fields and disc at low-normal pressures, the maximal decrease in IOP is necessary. Primary filtration presents the best choice. Iridoplasty is usually reserved for eyes with plateau iris syndrome (or, sometimes angle closure). Peripheral iridectomy would not be appropriate because the angles appear normal, and the likelihood of excellent pressure control after combined procedure is not high enough. Cyclocryotherapy and cyclopho-tocoagulation are reserved for end-stage disease.
49. a.(see explanation for answer 50).
50. d. This patient has pseudoexfoliation syndrome, which is characterized by the deposition of fibrillar material in the anterior segment of the eye. The trabecular meshwork is often heavily pigmented with inferior pigmented deposition referred to as the Sampaolesi’s line. On goni-oscopy, the angle can be narrow, most likely the result of anterior movement of the lens–iris diaphragm related to zonular weakness. On retroillumination, transillumination defects are seen at the pupillary margin. These patients dilate poorly and are predisposed to zonular dehiscence and complications during and after cataract surgery. Lens extraction does not alleviate the condition, and these patients often have increased ocular inflammation after any ocular surgery.
51. c. In pseudoexfoliation, fibrillar material is deposited in the anterior segment of the eye. Patients with this glaucoma are often resistant to medical therapy, but laser trabeculoplasty is often very effective. Pseudoexfoliation with glaucoma also differs from POAG in that it is often monocular or asymmetric and has greater pigmentation of the trabecular meshwork, as well as pigment deposited anterior to Schwalbe’s line (Sampaolesi’s line). There is considerable overlap in the age range of patients affected by each disorder.
52. c. Phacolytic glaucoma results when mature or hypermature cataracts leak high molecular weight proteins through microscopic defects in the capsule. A resultant macrophage response clogs the trabecular meshwork. Although medication is used for short-term IOP control, definitive therapy requires cataract extraction. Other lens-induced conditions may respond to topical steroid. Lens particle glaucoma occurs when lens cortex material deposits along the TM and can be seen after cataract surgery. Medical therapy to lower IOP and reduce inflammation can help.
53. c.(see explanation for answer 54).
54. d. This patient has signs of pigment dispersion syndrome. The syndrome does not universally lead to glaucoma as the risk is approximately 25% to 50%. Glaucoma associated with these findings occurs most commonly in young (20–50 years of age) white males who have high myopia. Affected females tend to be older than affected males. The presence of a Krukenberg’s spindle is not necessary to make the diagnosis. Filtering surgery is usually successful; however, extra care is warranted, because young patients with myopia may be at increased risk of hypotony maculopathy.
55. b. This is phacolytic glaucoma, an inflammatory glaucoma caused by leakage of lens protein through microscopic openings in the capsule of a mature or hypermature cataract. The lack of keratic precipitates helps distinguish phacolytic glaucoma from phacoantigenic glaucoma. Definitive therapy requires cataract extraction.
56. a. The most common cause of glaucoma in primary or metastatic tumors of the ciliary body is direct invasion of the anterior chamber angle.
57. b. The etiology of glaucomatocyclitic crisis, or Posner-Schlossman syndrome, remains unknown. There is no evidence that chronic suppressive therapy with topical nonsteroidal antiinflammatory agents or mild steroids is effective in preventing attacks.
58. a. Fifteen percent of patients with Fuchs heterochromic iridocyclitis will have secondary open-angle glaucoma.
59. b. Medications that reduce aqueous humor formation are more effective than drugs that increase trabecular aqueous outflow. Prostaglandin analogs may be effective in some patients. Laser trabeculoplasty is not effective unless there are secondary changes in the outflow channels. Glaucoma filter-ing surgery may be complicated by a ciliochoroi-dal effusion or a suprachoroidal hemorrhage.
60. b. Adrenergic agonists with significant α1-agonist effects (apraclonidine, dipivefrin, epineph-rine) should also be avoided in sickle cell disease because of concerns regarding anterior segment vasoconstriction.
61. b. Ghost cells develop within 1 to 3 months of a vitreous hemorrhage. While medical therapy is the preferred initial approach, these patients may require anterior chamber irrigation, pars plana vitrectomy, and/or trabeculectomy to control the condition.
62. d. It has been suggested that a chronic rheg-matogenous retinal detachment leads to the liberation of photoreceptor outer segments, which, migrating through the retinal tear, reach the anterior chamber and impede aqueous outflow through the trabecular meshwork.
63. d. A small corneal diameter and radius of curvature are factors that predispose to primary angle closure.
64. d. This is a patient with an acute angle closure attack. Anterior chamber depth of <2.5 mm predisposes patients to primary angle closure. Retinal vascular occlusion may occur as a result of increased intraocular pressure.
65. c. The definitive treatment for acute angle closure is an iridectomy, laser or surgical. In this patient, it may be best to first lower the intraocular pressure (IOP) using agents such as β-adrenergic antagonists; α2-adrenergic agonists; prostaglandin analogs; and oral, topical, or intravenous carbonic anhydrase inhibitors. Miotics do not tend to work when IOP is elevated above 40 to 50 mm Hg, but can be helpful once IOP has been lowered beyond this threshold.
66. c. An untreated fellow eye in a patient who has had an acute angle-closure attack has a 40% to 80% chance of developing an acute attack of angle closure over the next 5 to 10 years.
67. d. Both mydriatics and miotics can precipitate angle-closure in eyes with shallow anterior chambers. This is true for both topical medications and systemic drugs that affect the pupil. Examples include antihistamines, which can have anticholinergic activity.
68. a. Angle-closure develops in only a small number of patients with narrow anterior chambers. A number of provocative tests exist to attempt to cause angle closure in susceptible patients. Perhaps the most predictive is the prone–dark room test. IOP is measured before and after 30 to 60 minutes of total dark adaptation attained with the patient prone. Dark will induce pupillary dilation, and prone positioning will move the lens forward. Both tend to increase pupillary block. None of these tests, however, has been evaluated in a prospective study.
69. c. The patient with very narrow angles and elevated pressure may have “mixed mechanism” glaucoma with partial angle closure due to pupillary block superimposed on open-angle glaucoma To determine if an angle-closure component is present, the effect of minimizing pupillary block on IOP must be determined. Cholinergic miotics (pilocarpine) will cause miosis and lessen pupillary block but also will exert traction on the trabecular meshwork and lower IOP by this unrelated mechanism. Thymoxamine, a selective alpha-adrenergic antagonist, causes miosis and lessens pupillary block, without affecting outflow facility. A decrease in pressure after thymoxamine (lessened pupillary block) implies partial angle closure, and iridotomy is indicated. No change in IOP after thymoxamine-induced miosis implies that an iridotomy may not be helpful.
70. d. A small anterior segment is not associated with plateau iris.
71. a. Angle closure in plateau iris is most often caused by anteriorly positioned ciliary processes that critically narrow the anterior chamber recess by pushing the peripheral iris forward. A component of pupillary block is often present. Plateau iris may be suspected if the central anterior chamber appears to be of normal depth and the iris plane appears to be rather flat for an eye with angle closure. Plateau iris should be considered in younger patients with myopia.
72. c. Anterior displacement of the ciliary processes pushes the peripheral iris forward, which subsequently narrows the anterior chamber and blocks the trabecular meshwork. This has been confirmed with anterior segment ultrasonography. Patients who have plateau iris syndrome (e.g., resistant to laser peripheral iridotomy) should be treated with long-term miotics and possibly iridoplasty.
73. b. Treatment with cycloplegia may tighten the zonule, flatten the lens, and pull it posteriorly, breaking the pupillary block. Miotics may make the condition worse by increasing the pupillary block and by rotating the ciliary body forward, loosening the zonule and allowing the lens to become more globular. Microspherophakia is often familial and may occur as an isolated condition or as part of either Weill-Marchesani or Marfan’s syndrome.
74. b. While anti-VEGF therapy has become more widely used, the treatment of choice is still considered panretinal photocoagulation.
75. b. Choroidal detachment can present with shallow or flat anterior chamber, but the IOP is typically low. All of the other choices can present with high IOP.
76. c. Ultrasound is a critical step in evaluation of this patient. If no posterior pathology is found, then aqueous misdirection is suspected, especially in the setting of a patent iridotomy. Atropine and phenylephrine can help break the attack, along with IOP lowering agents. If these measures fail, then surgical options can be explored. These include YAG laser disruption of the anterior hyaloids face, vitrectomy, lensectomy, or ALT of the ciliary processes.
77. d. Fibrous ingrowth is more prevalent than epithelial downgrowth. Argon laser gives the characteristic white burns on the epithelial membrane surface, not YAG. Medication is the preferred treatment of the secondary glaucomas that present without a pupillary block mechanism, although surgical intervention may be required.
78. c. See answer 80 for explanation.
79. d. See answer 80 for explanation.
80. a. This patient likely started topiramate (Topamax) <1 month ago. She is experiencing an idiosyncratic reaction in which bilateral acute myopia (>6 D), bilateral ocular pain, headache, and bilateral angle-closure glaucoma can occur. The underlying mechanism is ciliochoroidal effusion, which causes relaxation of the zonules and anterior displacement of the lens-iris complex. Aggressive cycloplegia may relieve the attack and the secondary angle-closure glaucoma usually resolves within 24 to 48 hours with medical treatment. The myopia takes longer to resolve, often times up to 2 weeks. A PI is not indicated because pupillary block is not the underlying mechanism of angle-closure in these patients.
81. b. A child that presents with a large eye, or buphthalmos, and tearing has congenital glaucoma until proven otherwise. Other signs and symptoms of this condition include corneal edema, increased IOP, increased cup:disc ratio, photophobia, and blepharospasm. An exam under anesthesia should be performed if enough information cannot be obtained in a clinic setting. This condition can be mistaken for nasolacrimal duct obstruction because tearing is often the only presenting symptom.
82. c. While medications can be used to control IOP in children for a short period of time, they are not recommended for long-term IOP control. Surgical management is preferred in these patients. If the cornea is clear, both goniotomy and trabeculotomy ab externo are viable surgical options with comparable success rates. In a patient with a hazy cornea, however, goniotomy is difficult to perform and trabeculotomy ab externo is the preferred surgical option. Trabeculectomy and shunt procedures are reserved for patients in whom prior surgical options have failed.
83. a. α2-Adrenergic agents should be avoided in children < 3 years because of the risk of apnea and other CNS adverse effects. b-Adrenergic antagonists can be used but parents should be alert for apnea, hypotension, and cough (which may be a sign of reactive airway disease exacerbation). Carbonic anhydrase inhibitors (CAIs) may be used, but children require assessment for possible acidosis, hypokalemia, and feeding problems if given oral CAIs. Topical CAIs are relatively safe.
84. c. While elevated episcleral venous pressure plays a role in the glaucoma of Sturge-Weber syndrome, it often is implicated after the first decade of life. In infants, it is the angle anomalies that play the largest role in elevated IOP.
85. d. The principle ocular finding in NF2 is posterior subcapsular cataract. NF2 is not associated with glaucoma.
86. c. Brimonidine decreases aqueous production and increases uveoscleral outflow.
87. d. Dorzolamide can cause induced myopia, blurred vision, stinging, keratitis, conjunctivitis, and dermatitis.
88. c. Brimonidine can lead to hypotension, not hypertension.
89. d. Echothiophate iodide can cause increased salivation, secretions, and gastrointestinal cramping. Other ophthalmologic side effects include iris cysts and punctual stenosis.
90. a. Brimonidine is considered a class B agent during pregnancy, although use of this agent should be avoided in nursing mothers because of the effects on infants.
91. b. Caution must be exercised in the use of carbonic anhydrase inhibitors for small children because of their susceptibility to weight loss, lethargy, and metabolic acidosis.
92. c. Epinephrine has a well-established tendency to provoke irritation and allergic responses. More than one-fifth of patients will eventually experience an adverse local reaction with prolonged use.
93. d. Direct-acting miotics interact directly with the acetylcholine receptor, whereas indirect-acting agents increase the activity of native acetylcholine at the synaptic junction (by blocking its enzymatic degradation). Pilocarpine is a purely direct agent, whereas carbachol is felt to exhibit both direct and indirect effects. The only commercially available purely indirect parasympathomimetic currently is demecarium. Indirect parasympathomimetics can also be used against eyelid lice infestations because of their potent insecticidal effects.
94. b. Indirect agents, along with the strongest direct agents, tend to have the most pronounced systemic and ocular side effects. Bradycardia is never seen with any of the miotics.
95. a. Changes in urine pH secondary to carbonic anhydrase inhibitors can predispose a patient to calcium oxalate and calcium phosphate nephrolithiasis. Aplastic anemia is a rare, but potentially lethal side effect related to the sulfa derivation of the drugs. Gastrointestinal distress occurs, but not most commonly. Hypokalemia may occur as a result of the effects on renal ion transport, but hypocalcemia is not seen. Paresthesias are reported by most patients taking these potent agents.
96. b. High IOP secondary to angle closure may be causing severe eye pain and decreased visual acuity. Hypotony (wound leak, cyclodialysis) could precipitate painful choroidal hemorrhage.
97. b. Because pupillary block is probably present, an iridotomy should be performed. Miotics tend to increase postoperative inflammation and should be avoided here.
98. c. Failure to relieve postoperative angle closure with iridotomy suggests malignant glaucoma, which often responds to potent cycloplegics. If medical management fails, laser treatment to open the anterior hyaloid face, or even pars plana vit-rectomy, is necessary.
99. b. Usually, one half of the circumference, or 180°, of the trabecular meshwork is treated during an initial laser trabeculoplasty.
100. a. Argon laser trabeculoplasty (ALT) uses a 50 mm beam with variable power to produce blanching or a tiny bubble at the anterior pigmented edge of the TM. This requires 180° of treatment, rather than 360°. Outflow facility typically improves following successful ALT.
101. b. When effective, laser trabeculoplasty is expected to lower IOP 20% to 25%.
102. d. Laser trabeculoplasty is contraindicated in patients with inflammatory glaucoma, iridocor-neal endothelial (ICE) syndrome, neovascular glaucoma, and synechial angle closure.
103. d. Up to 20% of patients undergoing laser trabeculoplasty can have a transient rise in IOP, sometimes reaching up to 50 to 60 mm Hg. Topical apraclonidine 1% or brimonidine 0.2% has been shown to blunt postoperative IOP elevation.
104. b. The glaucoma associated with ICE syndrome is often worse than predicted by the extent of synechiae, likely due to clinically undetectable endothelialization of the angle.
105. c. The constellation of heterochromia iridis (compare the two images carefully), gelatinous– stellate keratic precipitates, mild anterior chamber reaction, distinctive rubeosis, and ipsilateral cataract and glaucoma is nearly pathognomonic for Fuchs’ heterochromatic iridocyclitis. If inflammation is severe, another diagnosis should be considered. The iris atrophy in Fuchs’ is generally diffuse and stromal, whereas that of herpes zoster iritis is typically sectoral with pigment epithelial involvement. The rubeosis is distinctive because the vessels are typically quite fine and rarely induce synechiae or angle closure. The vessels are also quite fragile and spontaneous or iatrogenic hyphema (as the paracentesis is performed at filtration surgery) is a classic sign. The mechanism for the glaucoma is poorly understood. Cataract surgery is usually indicated for visual rehabilitation; it has little or no effect on the glaucoma. In fact, in many patients, IOP does not increase for many months or years after cataract extraction.
106. d. Assuming the left angle is normal, this patient can be diagnosed with angle recession (posttraumatic) glaucoma affecting the right eye. Because men are victims of ocular trauma far more frequently than women, this glaucoma is more common in men. The lifetime risk for developing glaucoma seems to be correlated with the amount of angle recession and is estimated to be approximately 10% in patients with 180° of involved angle. Iris sphincter tears, Vossius’ ring, and posterior subcapsular cataract all may be seen in conjunction with the disorder. Retinal dialysis must be ruled out in the posttraumatic period by a dilated retinal examination with 360° scleral depression. Although the disorder may be bilateral if the contralateral eye is traumatized, it is much more commonly unilateral.
107. c. Typically, the surgeon should fastidiously avoid contact between the MMC-containing sponge and the wound edges to reduce the risk of postoperative wound leaks and hypotony. This is one of the main reasons why most MMC filters are performed with a limbus-based flap. MMC is associated with a lower incidence of hypotony and corneal-surface disorders than 5-FU.
108. a. Young age is a risk factor for bleb-related endophthalmitis. In addition, contact lens use and chronic bleb leak are also risk factors.
109. a. The lens increases in thickness and curvature and has a decreased index of refraction with age. The eye may become more hyperopic or myopic with age depending on the balance of these changes.
110. d. The lens capsule is made up of type IV collagen.
111. a. The lens capsule is thinnest at the posterior pole.
112. c. Aldose reductase is the key enzyme in the sorbitol pathway. When glucose increases in the lens, as in hyperglycemic states, the sorbitol pathway is activated relatively more than glycolysis. Sorbitol accumulates and is retained in the lens.
113. a. This is the process of accommodation. When the ciliary muscle contracts, the axial thickness of the lens increases, diameter decreases, and dioptric power increases.
114. a. Alport’s syndrome is usually X-linked, but can be autosomal recessive. In addition to anterior lenticonus, it is associated with renal failure, deafness, cataract, and fleck retinopathy.
115. b. They may be associated with colobomas of the uvea as well.
116. c. In addition to this finding, patients can display adhesions between lens and cornea, anterior cortical or polar cataract, and microspherophakia.
117. b. Approximately one-third of congenital cataracts are a component of a more extensive syndrome or disease, one-third occur as an isolated inherited trait, and one-third result from undetermined causes.
118. a. Lamellar cataracts are the most common type of congenital and infantile cataracts.
119. b. The lens changes are often characterized by pearly white nuclear opacifications. After cataract surgery, there is often excessive inflammation from the release of live virus particles. Both glaucoma and cataract are not usually present simultaneously in the same eye, which likely has to do with timing of the exposure and maternal infection.
120. d. Mittendorf ’s dot is a remnant of the posterior tunica vasculosa lentis and results in a white dot inferonasally on the posterior capsule of the lens. It is meaningless visually.
121. d. This is a posterior subcapsular cataract. Choice “a” describes nuclear cataracts. Choice “b” is a cortical cataract.
122. c. Phenothiazines can cause pigmented deposits in the anterior lens epithelium in an axial configuration. Miotics can lead to small vacuoles within and posterior to the anterior lens capsule and epithelium that can progress to posterior cortical and nuclear lens changes. Long-term human studies demonstrated that statins do not increase cataract risk and may actually reduce the risk of nuclear cataracts by 50% over 5 years. Amiodarone, in addition to cataracts, can cause deposits in the cornea and optic neuropathy.
123. a. The characteristic lens changes and systemic findings point to galactosemia. This is an inherited autosomal recessive inability to convert galactose to glucose. The disease is fatal if untreated and can present within the first few weeks of life with cataracts, malnutrition, hepatomegaly, jaundice, and mental deficiency. Diagnosis can be confirmed by demonstration of galactose in the urine.
124. a. (See answer 126 for explanation)
125. d. (See answer 126 for explanation)
126. b. This is phacoantigenic (or phacoanaphy-lactic) uveitis that occurs days to weeks after a large amount of lens protein is released through a ruptured lens capsule. A granulomatous response ensues and is difficult to control until the lens is removed. Phacolytic glaucoma occurs as a complication of a mature or hypermature cataract in which lens proteins leak through an intact but permeable lens capsule. The trabecu-lar meshwork can become clogged with lens particles and engorged macrophages in this condition. Phacomorphic glaucoma occurs when an intumescent cataract causes pupillary block and induces a secondary angle-closure glaucoma.
127. c. The decision to operate is not based solely on a specific level of reduced acuity.
128. d. Decreasing IOP via aqueous release from paracentesis site often results in immediate resolution of edema.
129. d. Argon laser burns applied to the membrane or iris surface will appear white if epithelial cells are present.
130. b. TASS presents within 12 to 24 hours, whereas acute infectious endophthalmitis typically develops 2 to 7 days after surgery.
131. b. Tamsulosin, or Flomax, can be associated with intraoperative floppy iris syndrome (IFIS). It is used for the treatment of benign prostatic hypertrophy.
132. c. It is recommended that only removal of fragments that are visible and easily accessible be attempted. Referral for prompt vitreoretinal consultation is also indicated.
133. d. PCO formation is influenced by lens material (PMMA > silicone > acrylic) and edge design (round > square). Pooled data has found the overall PCO rate at 5 years to be 28%.
134. b.(See answer 135 for explanation)
135. d. Treatment of retrobulbar hemorrhage is targeted at lowering intraocular pressure as quickly as possible. Cataract surgery should not be performed when a serious hemorrhage has occurred as the risk of iris prolapse and expulsive choroidal hemorrhage increases. The patient’s medical history must always be considered as this patient had a history of thrombosis for which he was anticoagulated, increasing his risk for retrobulbar hemorrhage.
136. a. Suprachoroidal hemorrhage is more common in patients with hypertension, tachycardia, obesity, high myopia, anticoagulation, glaucoma, advanced age, and chronic ocular inflammation.
137. d. This patient has acute postoperative endo-phthalmitis. The Endophthalmitis Vitrectomy Study (EVS) demonstrated that for with HM or better vision, vitrectomy and vitreous tap/inject were equally beneficial. For patients with LP or worse vision, vitrectomy was found to be better than vitreous tap/inject.
138. a. The crystalline lens is derived from ectoderm.
139. b. A bleb leak would cause a flat bleb. Pupillary block and aqueous misdirection would not change the size of the bleb.
140. b. Streptococcus species account for about half of all bleb-associated endophthalmitis, followed by coagulase negative Staphylococcus and Haemophilus influenzae.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


