Glaucoma in Aphakia and Pseudophakia
Mark A. Werner
Alana L. Grajewski
Classification
The terms aphakic glaucoma or pseudophakic glaucoma erroneously imply that the glaucoma is caused by the lens extraction or state of aphakia or pseudophakia. There are many causes that, alone or in combination, can result in elevated intraocular pressure (IOP). For this reason, these terms should be avoided and the glaucoma best described by the specific underlying mechanism responsible for the pressure elevation. The etiology of elevated IOP after cataract extraction is often multifactorial. In general, it is not unusual for there to be more than one coexisting mechanism for the glaucoma. Management of these concurrent problems is directed at each component individually. As the nature of cataract surgery has evolved from intracapsular cataract extraction (ICCE) to extracapsular cataract extraction (ECCE) to clear corneal phacoemulsification, the possible mechanisms for postoperative glaucoma have also changed. Management depends to a large degree on treating the primary mechanism. There are also some treatment considerations common to all categories. To categorize the pathogenesis of elevated IOP in aphakic or pseudophakic eyes, the broad classifications of open-angle or closed-angle are useful, as is the temporal relationship of the IOP elevation to surgery (e.g., early versus late, transient versus persistent).
Incidence
The reported incidence of glaucoma after cataract extraction has steadily decreased due to advances in microsurgical technique. In the 1970s, the reported incidence of postoperative glaucoma varied from 0.7% to 12%, along with variations in suture material and method of closure.1,2 However, as the occurrence of microscopic leaks and hypotony has diminished with improved sutures and tighter closure, the incidence of immediate IOP elevation after cataract surgery has likely increased.3 Chronic secondary glaucoma, however, decreased as frequency of postoperative shallow chambers with peripheral anterior synechiae formation decreased. In the 1980s, the incidence in eyes undergoing standard ECCE was approximately 4%.4 Several large series comparing ICCE with ECCE found no difference in the frequency of postoperative glaucoma when wound closure was similar.5,6 There is little published data regarding incidence of chronic glaucoma with modern small incision phacoemulsification and in-the-bag intraocular lens (IOL) placement; however, the authors believe it is further reduced.
Both anterior (ACIOL) and posterior (PCIOL) chamber intraocular lens implantation after cataract extraction have also been associated with postoperative glaucoma. Previously, chronic secondary glaucoma complicated uneventful cataract extraction in 5.5% of eyes that received anterior chamber IOL implants, compared with 1.6% of eyes that had posterior chamber lens implants.7 More recently, investigators have found lower rates of glaucoma with open-loop flexible ACIOL implants.8 Iris-plane or iris-fixed lenses, which are rarely seen today, often have been associated with prolonged IOP elevation.9 The incidence of postoperative glaucoma in eyes receiving secondary anterior chamber implants has been recorded to be as high as 11.3%.10
Pre-Existent Open-Angle Glaucoma in Cataract Extraction
Cataract and glaucoma frequently coexist in the same eye. The effect of cataract extraction on IOP control in patients with pre-existent primary open-angle glaucoma can be divided into two categories:
Transient effects: The immediate or acute elevation of IOP appears to occur more frequently in glaucomatous eyes than in nonglaucomatous eyes. Preoperative argon laser trabeculoplasty has been reported to be beneficial in postoperative IOP control,11,12 but Savage et al.13 and McGuigan et al.14 reported significant postoperative IOP spikes despite previous control with laser and topical medications.
Persistent effects: In contrast, a small long-term decrease in IOP and improved IOP control after lens extraction has been consistently reported.15,16,17 Undiagnosed preoperative pupillary block may be a factor in improved postoperative IOP control in some cases, because it is most often resolved by cataract extraction, but other factors likely play a role.17
Co-existent Cataract and Glaucoma
The primary decision regarding management of postoperative IOP elevation in this group of patients begins preoperatively with the choice of surgery. If a patient has a cataract that is visually significant in the presence of glaucoma, the choice of surgery includes the following: (a) cataract surgery alone; (b) initial glaucoma filtering surgery, with cataract surgery planned as a future procedure; and (c) a combined glaucoma and cataract procedure. Opinions differ regarding each of these alternatives, and management of the patient with co-existent cataract and glaucoma is controversial.
The procedure of choice for each patient depends on several factors, including functional severity of the cataract, severity of the glaucoma (optic nerve and visual field damage), the patient’s tolerance to current medication, and the feasibility of performing a second surgical procedure. Cataract extraction alone is indicated in patients who have good IOP control, are on a minimal amount of well-tolerated medication, and have mild glaucomatous damage. The advantage of performing cataract extraction alone is the likelihood of fewer complications. The disadvantages are frequent postoperative IOP spikes and overall minimal IOP lowering.
A two-stage approach may be considered for a patient whose moderate or profound glaucomatous damage is uncontrolled despite maximally tolerated medication and whose cataract is mild to moderate. In this situation, filtration surgery is performed initially; if the cataract is marginal, the cataract surgery is scheduled for a future date. The advantage of this approach may be better long-term IOP control than cataract surgery combined with a standard trabeculectomy. This effect of improved IOP control may be undone to some extent following subsequent cataract surgery, but a direct comparison of these two approaches is lacking. Disadvantages of the two-stage approach include: (a) a required second surgery; (b) the possibility of postoperative IOP spikes despite the presence of a functional filter;18 and (c) the possibility that the patient will require a third operation if the initial filtering surgery fails after cataract extraction.
A combined phacoemulsification and trabeculectomy may also be indicated for patients with advanced optic nerve and visual field damage.19 Advantages are the reduced number of surgical interventions and the decreased frequency of an early postoperative IOP elevation. Compared with the two-stage approach, a combined procedure offers early visual rehabilitation. Disadvantages include added surgical difficulty and an increased rate of surgical complications. As stated above, long-term IOP control may be compromised when filtration surgery is done in combination with cataract extraction.20,21,22 For this reason, several groups have attempted to enhance the filter function by using either intraoperative mitomycin C or postoperative subconjunctival 5-fluorouracil. Some of these reports have been encouraging, but long-term data have yet to be reported.23,24 In one study, only patients having identified risk factors, such as previous failed trabeculectomy, African American race, preoperative IOP ≥ 20 mmHg with medications, and use of ≥ two medications preoperatively, were found to benefit from mitomycin C.25,26
Other surgical options have been investigated more recently for patients with co-existing cataract and glaucoma. Nonpenetrating glaucoma surgery, endoscopic cyclophotocoagulation, endoscopic erbium:YAG goniopuncture, trabeculotomy, ab interno trabeculectomy, Ex-PRESS mini-shunt placement, and other procedures have achieved sustained IOP lowering in combination with cataract surgery.27,28,29,30,31,32
Cataract Extraction in Eyes with Previous Trabeculectomy
Most studies indicate a slight loss of IOP control on average following phacoemulsification.33,34,35 However, an acute rise in pressure is also possible. One of the authors (MW) has observed an acute rise in IOP six days after an uneventful phacoemulsification with posterior chamber intraocular lens implantation with posterior synechialysis. The patient responded favorably to needling of the bleb with 5-fluourouracil injection. In another report, following Nd:YAG capsulotomy in an aphakic patient, vitreous reportedly came forward and blocked the surgical ostomy, leading to acute IOP elevation.36 An anterior vitrectomy was performed, but the pressure remained elevated despite medical therapy.36
Postcataract Extraction Complications and Management
Transient Postoperative Intraocular Pressure Elevation
In the immediate postoperative period, a transient IOP elevation may accompany uncomplicated cataract extraction. Both ICCE37,38 and ECCE39,40 have been associated with significant and rapid changes in IOP after surgery with similar incidences. The majority of early postoperative conditions are transient and related to outflow obstruction. In addition, chronically elevated IOP may result from several early postoperative conditions, described below.
Why worry about postoperative IOP spikes that are generally self-limited? Hayreh et al. has reported on a series of postcataract extraction anterior ischemic optic neuropathy (AION).41 The vision in his series of 11 eyes ranged from 6/6 to hand motions, with two patients having worsening of previously diagnosed glaucoma. The pathogenesis was felt to be compromised blood flow to the optic nerve from a combination of increased IOP postoperatively, present in most patients to some degree, and systemic hypoperfusion.41
Acute Infection
Endophthalmitis can cause an early IOP elevation, and its presence should be considered in the immediate postoperative period in patients with elevated IOP and inflammation. (A complete discussion of postoperative endophthalmitis can be found elsewhere in these volumes.)
Bacterial infection should be suspected whenever IOP elevation is associated with pain, decreased vision, and both intraocular and extraocular inflammation, particularly within 1 to 7 days after cataract extraction. Appropriate clinical and laboratory evaluation should be instituted.
Management
Attention to treatment of the infection takes precedence to managing the IOP. The mechanism of IOP elevation is most likely secondary to outflow obstruction from inflammatory cells and debris, and appropriate antimicrobial treatment with or without pars plana vitrectomy should aid in clearing this particulate load. If the IOP remains elevated, other underlying mechanisms of IOP elevation should be looked for, identified, and treated as outlined in the remainder of this chapter.
Viscoelastic Substances
The transition from ICCE to ECCE has lead to a transition in postoperative complications. In particular, zonulolytic glaucoma induced by alpha-chymotrypsin has been replaced by transient early IOP elevation associated with viscoelastic substances, including sodium hyaluronate and chondroitin sulfate.42,43,44
IOP elevation can fluctuate as high as 60 mmHg and occurs by the first postoperative day.45 Spontaneous resolution can occur within 48 to 72 hours. Preexisting glaucoma is associated with more frequent and more severe IOP spikes.46,47 Postoperative IOP elevation has been encountered with all viscoelastics to some degree.48 Several studies have found no difference in IOP rise for various types of viscoelastics.48,49 Rainer et al. found a significantly higher IOP increase with Viscoat (sodium chondroitin sulfate-sodium hyaluronate) compared with Healon 5(sodium hyaluronate).50 The authors postulate that the dispersive qualities of Viscoat preclude the complete removal of viscoelastic at the end of surgery, leading to higher IOP spikes.50 Methylcellulose 1% to 2% and hydroxypropyl methylcellulose 2% appear to offer some protection to corneal endothelium without raising the IOP.51
Mechanical obstruction of the trabecular meshwork with reduced outflow facility is the most likely primary mechanism of elevated IOP for all the viscoelastic agents. In enucleated human eyes, the outflow facility was decreased by 65%.52 Glasser et al.43 reported a decrease in postoperative IOP elevation after anterior chamber irrigation of sodium hyaluronate, but Stamper and associates53 found that aspiration of sodium hyaluronate did not significantly reduce the incidence of IOP elevation. Outflow facility in enucleated human eyes was not affected by either irrigation or aspiration of the sodium hyaluronate; it was improved by anterior chamber irrigation with hyaluronidase.
Management
The postoperative IOP elevation that occurs with the use of viscoelastic agents is exacerbated by cortical remnants and blood. Careful cortical cleanup and aspiration of the viscoelastic agent may reduce the degree of IOP elevation. Prophylactic treatment of all patients (particularly those with preexistent glaucoma) with topical or systemic carbonic anhydrase inhibitors, topical β-adrenergic blockers, or intracameral carbachol may decrease the incidence or severity of postoperative IOP elevation.54,55,56,57,58 Transient IOP elevation may be treated medically in many cases. For large IOP spikes, particularly those associated with pain or preoperative glaucoma, fluid and/or viscoelastic may be released from a paracentesis wound at the slit lamp with relative ease.
Hyphema
Most early postoperative hemorrhages associated with cataract extraction or combined procedures are self-limited. The source of the hemorrhage can be the edge of the corneoscleral wound, an iridectomy, or other site of iris trauma. Unless there is a significant amount of blood, debris, or the presence of a viscoelastic substance in the anterior chamber, these early postoperative hyphemas are asymptomatic and not associated with elevated IOP. The mechanism of IOP elevation is obstruction of the trabecular meshwork by one or more of the following: blood, debris, macrophages, and clot. These substances are usually reabsorbed spontaneously without treatment.
Management
Unless reabsorption is delayed by excessive debris or previously compromised outflow, medical management is usually adequate. Pharmacologic agents used are carbonic anhydrase inhibitors or β-adrenergic blockers. To minimize iris movement and treat the often attendant intraocular inflammation, cycloplegics and corticosteroids can be of benefit. Surgical evacuation is necessary only if the glaucoma is unresponsive to tolerated medical therapy or there is risk of corneal blood staining.
Inflammation and Lens Particle Glaucoma
Cellular and chemical mediators of inflammation decrease trabecular meshwork function and outflow by a variety of mechanisms and in varying degrees of severity. Both cellular and particulate inflammatory debris can clog trabecular meshwork and compromise outflow.59,60 Additionally, the increased aqueous protein concentration caused by the breakdown of the blood-aqueous barrier also contributes to early postoperative IOP elevation. Each of these inflammatory components are further exacerbated by the presence of any residual viscoelastic substance in the anterior chamber.43 Contrary to decreasing outflow facility, the role that prostaglandins play in postoperative IOP elevation may relate to their effect on increasing aqueous production.
Cortical lens fragments retained in either the anterior chamber or the vitreous can also obstruct the trabecular meshwork in the form of free lens particles or macrophages swollen with lens material (Figs. 1 and 2). Glaucoma probably does not occur in most eyes that contain few cortical remnants. However, the inflammatory response may be more pronounced and prolonged in eyes containing a larger amount of lens material. When inflammation is marked, keratic precipitates and even a hypopyon may be present. Distinction between this sterile inflammatory endophthalmitis and infectious endophthalmitis can be difficult and may depend on the initial response to therapy. The presence or absence of IOP elevation is not helpful in making this distinction because IOP may be normal or elevated in both situations.
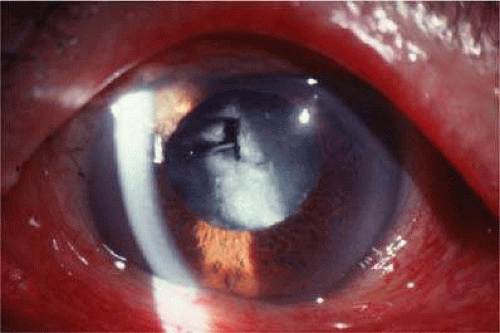 FIGURE 1. Fluffy, hydrated cortical lens fragments retained in the capsular bag after cataract extraction, resulting in inflammation and elevated intraocular pressure. (Courtesy of E. Hodapp, M.D., Miami, FL). |
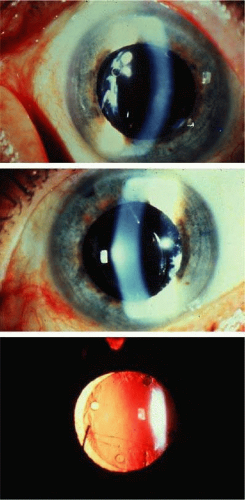 FIGURE 2. A. Posterior chamber lens implant with prolene haptics, with the patient’s head in the primary position. B. Same posterior chamber lens implant as in figure a, but with the patient’s head tilted, demonstrating mobility of the lens in the posterior chamber. C. Transillumination defects in the iris secondary to chronic lens movement and trauma to the pigment epithelium, same patient. (Courtesy of R. K. Parrish II, M.D., Miami, FL). |
Management
Inflammation is likely to occur to some degree after cataract extraction. The degree to which this will affect postoperative IOP depends to some extent on pre-existent trabecular meshwork function and the severity of the inflammatory response. Compromised outflow may be, at least in part, offset by aqueous hyposecretion. In general, treatment is aimed at controlling the inflammation with corticosteroids. Aspirin and nonsteroidal anti-inflammatory agents (e.g., indomethacin) may also help to control postoperative inflammation.
Management of elevated IOP relies on treatment with aqueous suppressants. Because of the disruption of the blood-aqueous barrier, hyperosmotic agents are of limited utility in the postoperative patient with inflammation. Miotics and prostaglandins should be avoided. Mydriatics or cycloplegics to prevent formation of posterior synechiae are recommended if inflammation is marked. If posterior synechiae do develop in the inflamed postoperative eye, attempts should be made to break these with dilation to avoid pupillary block as a result of a secluded pupil. If pharmacologic mydriasis is unsuccessful, laser pupilloplasty may achieve photomydriasis.61 After iris bombé does develop, however, a laser iridotomy is indicated if vigorous mydriasis is unsuccessful.
Lens particle glaucoma treatment is similarly aimed at the underlying inflammation. The glaucoma usually resolves as the retained cortical material resorbs and inflammation decreases. Aqueous suppressants are of temporary help in controlling this transient IOP elevation. If spontaneous reabsorption is prolonged or medical therapy either fails or is not well tolerated, surgical removal of the residual cortex is necessary.
Vitreous in the Anterior Chamber
Anterior chamber vitreous prolapse can occur after an ICCE or after inadvertent rupture or dialysis of the posterior capsule during ECCE. In the case of phacoemulsification or planned ECCE, vitreous prolapse is often associated with other IOP-provoking elements, such as inflammatory debris or blood.62,63 The mechanism of open-angle postoperative glaucoma in this setting may be related to the degree of inflammation and blood in the anterior chamber. Another potential mechanism is direct obstruction of the trabecular meshwork by vitreous fibrils, whose peripheral extent may sometimes be difficult to appreciate on examination.64
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


