![]() 16
16 ![]()
Glaucoma Associated with Systemic Disease
Joern B. Soltau
Definition
What Systemic Diseases and Problems Are Associated with Elevated Intraocular Pressure or Glaucoma?
Several groups of systemic diseases can be associated with elevated intraocular pressure (IOP) and/or glaucomatous optic neuropathy: endocrine disorders, vascular disease, collagen vascular disease, renal disease and hemodialysis, hematologic disorders, primary familial amyloidosis, irradiation, systemic viral disease, parasitic disease, dermatologic disorders, and neurologic disorders. For management see Figure 16–1.
GLAUCOMA ASSOCIATED WITH ENDOCRINE DISORDERS
Definition
What Are the Main Endocrine Disorders that Are Associated with Elevated IOP?
Glaucoma occurs in association with several endocrine disorders: pituitary disease, Cushing’s syndrome, diabetes mellitus, and thyroid disease. For management see Figure 16–2.
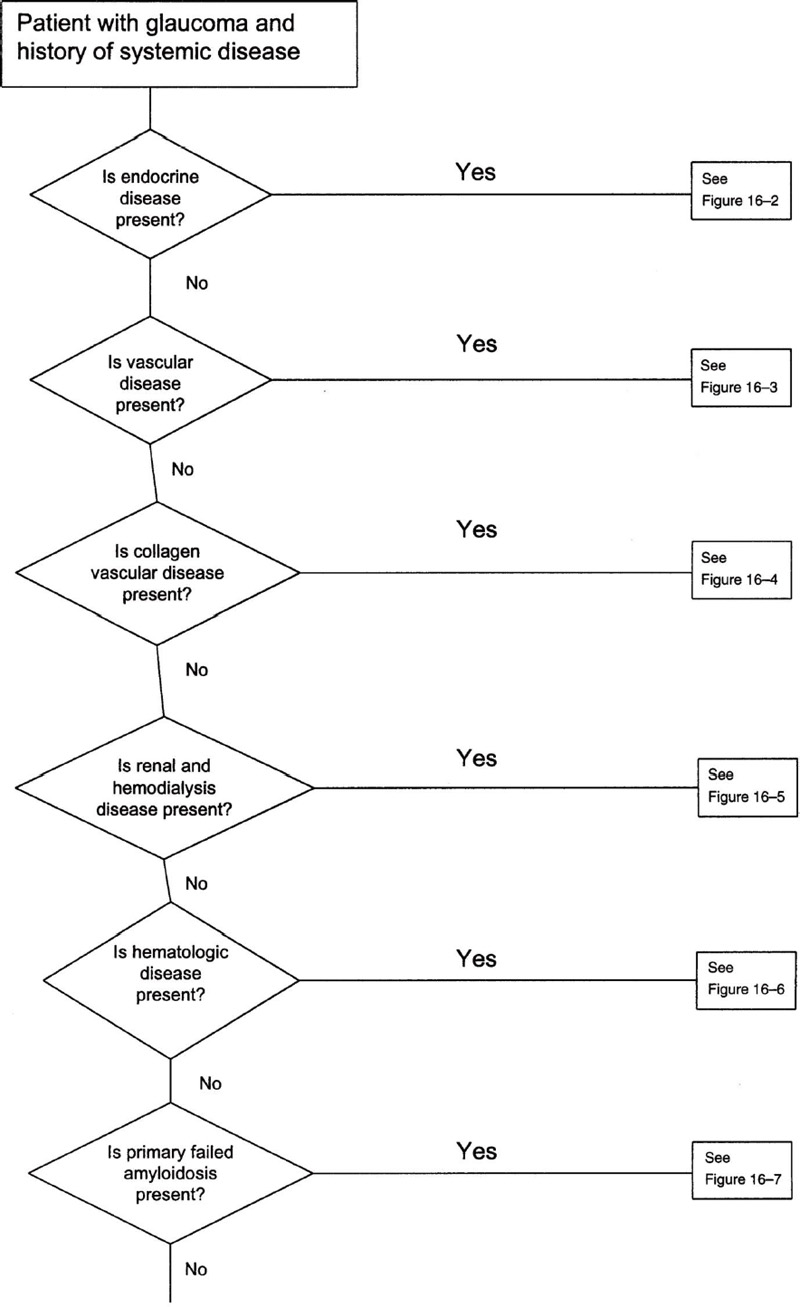
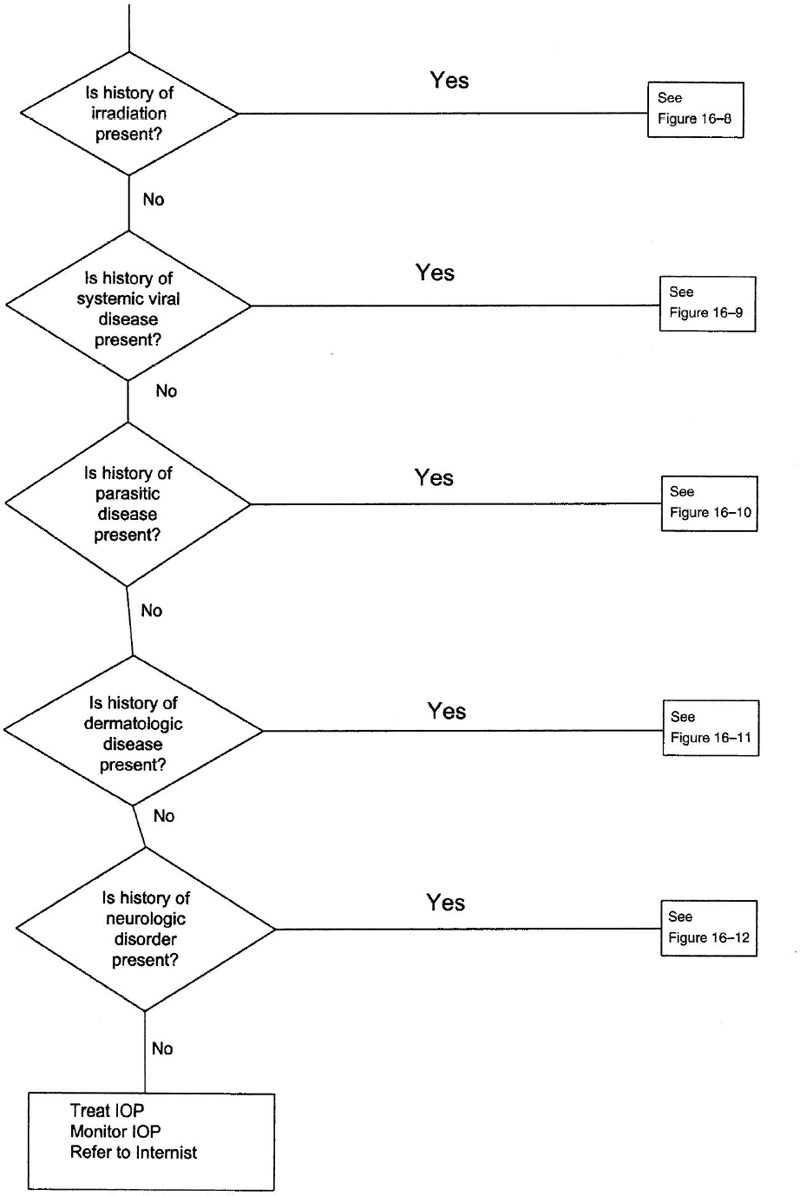
Figure 16–1. Management of a patient with glaucoma and systemic disease(s).
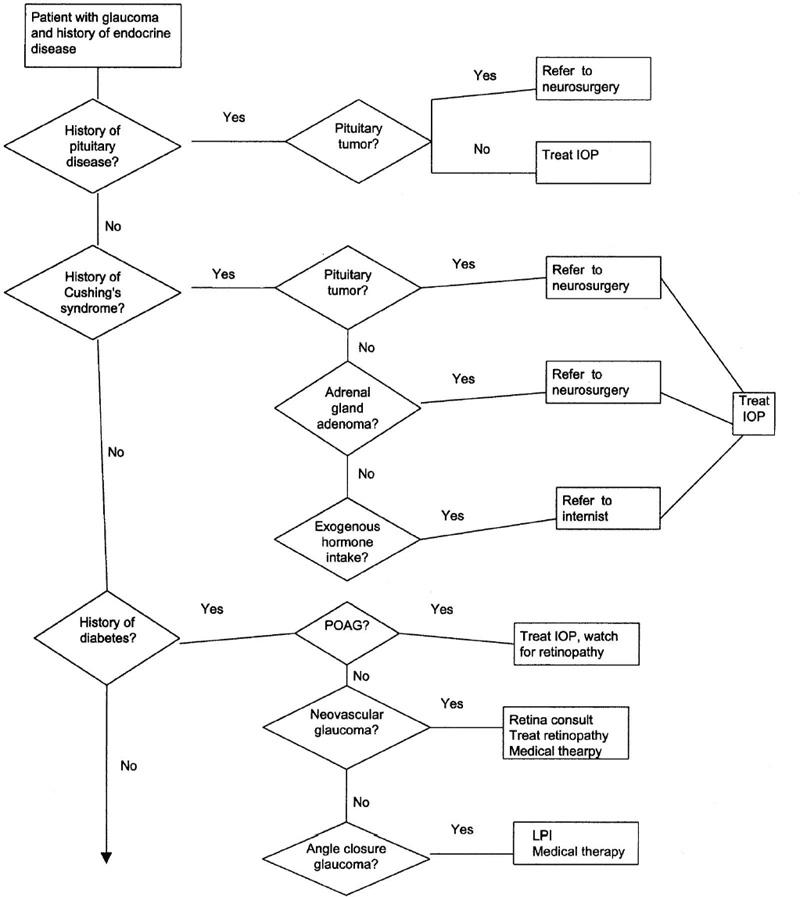
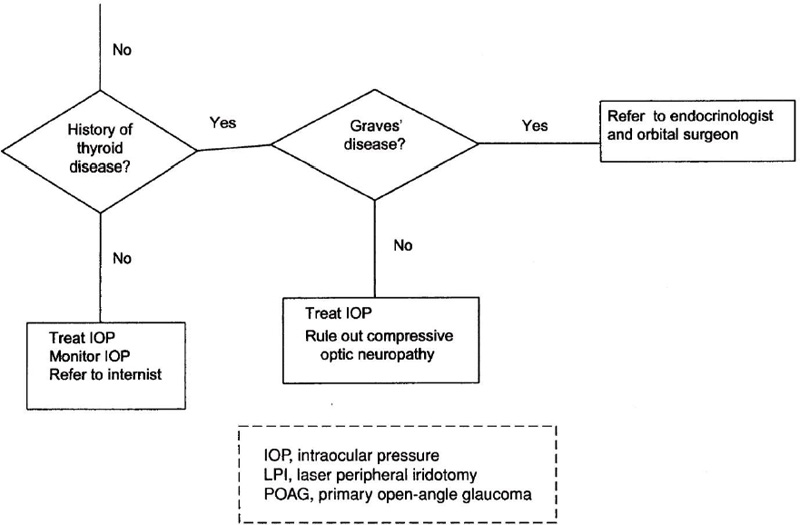
Figure 16–2. Management of a patient with glaucoma and endocrine disease.
GLAUCOMA ASSOCIATED WITH PITUITARY DISEASE
Definition
How Does Pituitary Disease Present Clinically?
The two most common types of pituitary adenomas are prolactinomas and somatotropic adenomas. Hyperprolactinemia is the most common form of pituitary hyperfunction. In women hyperprolactinemia causes galactorrhea, amenorrhea, and infertility. In men it causes impotence and diminished libido. Somatotropic adenomas are the second most common form of pituitary adenoma. These tumors produce excess growth hormone, resulting in skeletal growth changes in childhood leading to gigantism. In adults excess growth hormone secretion results in soft tissue swelling and hypertrophy involving the extremities and face, the hallmarks of acromegaly.
Why Is the IOP Elevated in Patients with Pituitary Disease?
There has been a suspicion that IOP can be regulated by neural and/or humoral influences on the rate of aqueous humor formation. However, it is difficult, if not impossible, to separate specific influences of the central nervous system on the IOP from vascular-induced or other secondary alterations. Although there is an association between chronic open-angle glaucoma and pituitary tumors, the exact mechanism by which this occurs is unknown.
Epidemiology and Importance
Is the IOP Elevated in Someone with Pituitary Disease?
In one study, patients with open-angle glaucoma were found to have on average growth hormone levels twice as high as controls after intravenous administration of arginine,1 and patients with hyperprolactinemia were found to have a sustained increase in IOP after water load compared to normal individuals.2 However, in a group of patients with acromegaly the elevated IOP was felt to be secondary to a thicker cornea in this group of patients.3
Diagnosis and Differential Diagnosis
It is still unclear if there is a direct link between increased growth hormone or prolactin levels and IOP. Therefore, it is paramount to make sure that in patients with the above-named conditions other etiologies for the elevated IOP are excluded and that existing or progressing visual field defects are not caused by the pituitary tumor itself.
Treatment and Management
Treatment of glaucoma in patients with pituitary tumors is the same as that for patients with chronic open-angle glaucoma. Progression in visual field changes may be due to either the glaucoma or the tumor itself. Therefore, special care must be taken when visual field changes are not consistent with optic nerve head changes or are not typical for glaucoma. For example, prominent bitemporal visual field depression should alert the physician to exclude pituitary pathology even in the presence of typical glaucoma related visual field changes.
Future Considerations
Further exploration of the central regulation of IOP may help to understand the pathophysiology of open-angle glaucoma.
GLAUCOMA ASSOCIATED WITH CUSHING’S SYNDROME
Definition
What Is Cushing’s Syndrome?
Cushing’s syndrome may be associated with corticotropic adenomas of the pituitary gland, adrenal gland adenomas, or exogenous hormone administration. Excessive adrenocorticotropic hormone (ACTH) results in centripetal obesity, hypertension, diabetes, amenorrhea, osteoporosis, and muscle atrophy.
Why Is the IOP Elevated in Patients with Cushing’s Syndrome?
The facility of outflow is up to 50% decreased in patients with Cushing’s syndrome.4–6 Excessive ACTH production from a pituitary corticotropic adenoma causes the adrenal gland to increase secretion of Cortisol, which in turn decreases the outflow facility (see Chapter 15).
Is There a Connection Between Chronic Open-Angle Glaucoma and Gushing’s Syndrome?
Increased plasma Cortisol levels7–9 and a disturbance of the hypothalamo-hypophyseal-adrenal gland system10,11 have been found in patients with ocular hypertension and glaucoma.
Epidemiology and Importance
In one study, IOP greater than 21 mm Hg was found in only four eyes of 62 patients with Cushing’s syndrome.12 In another series, 7 out of 29 patients with Cushing’s syndrome had IOPs above 23 mm Hg.13
Diagnosis and Differential Diagnosis
Cushing’s syndrome might be caused by a pituitary adenoma. Therefore, it is of paramount importance to make sure that progression in visual field changes is not caused by compressive optic neuropathy by the tumor itself. Special care must be taken when visual field changes are not consistent with optic nerve head changes or are not typical for glaucoma.
Treatment and Mangement
Glaucoma in patients with Cushing’s syndrome is treated the same as chronic open-angle glaucoma. Adrenalectomy with resulting normalization of hormone levels may allow IOP and reduced outflow facility to return to normal.4–6,12,14
Future Considerations
Further research into the influence of glucocorticoids on aqueous outflow, on the expression of trabecular meshwork inducible glucocorticoid response (TIGR) protein in particular, will help understand the mechanism of open-angle glaucoma.15–17
GLAUCOMA ASSOCIATED WITH DIABETES MELLITUS
Definition
Two main types of diabetes exist: type I, insulin-dependent diabetes mellitus, and type II, non–insulin-dependent diabetes mellitus. Chronic open-angle glaucoma, angle-closure glaucoma, and neovascular glaucoma have all been associated with both forms of diabetes mellitus.
Epidemiology and Importance
Is There a Connection Between Chronic Open-Angle Glaucoma and Diabetes Mellitus?
The issue of whether open-angle glaucoma is more prevalent in patients with diabetes mellitus appears to be controversial.18 Although many studies do show a positive correlation between those two conditions,6,19–27 other studies do not confirm this association.28–34 However, some studies have shown that IOP in patients with type I and II diabetes mellitus seems to be higher than in the general population.23,24,35,36
Can Diabetes Mellitus Cause an Angle-Closure Attack?
Lens swelling through influx of free water from acute hyperglycemia may precipitate an angle-closure attack in susceptible individuals.37,38
Is Neovascular Glaucoma Still an Issue in Diabetic Patients?
Neovascular glaucoma is the final complication of diabetic proliferative retinopathies. Its incidence has significantly decreased due to the improvement of the management of diabetic patients and systematic panretinal photocoagulation.39
Diagnosis and Differential Diagnosis
In every patient with diabetes mellitus, the clinician’s suspicion needs to be raised to detect ocular complications. For the glaucoma specialist this includes detection of visual field changes that are not secondary to defects caused by retinal photocoagulation for diabetic retinopathy, but rather secondary to glaucomatous optic neuropathy. The evaluation of optic nerve head changes might also be difficult in a patient with active or regressed neovascularization of the disc. Regular gonioscopy is also important to detect early neovascularization of the angle and neovascular glaucoma early in its course.
Treatment and Management
Treatment of glaucoma in association with diabetes mellitus is aimed at the underlying etiology—open-angle glaucoma, angle-closure glaucoma, or neovascular glaucoma. Treating a patient with open-angle glaucoma and diabetes can be very challenging, because visual field changes might be secondary to diabetic retinopathy or laser treatment of the disease. Diabetics with glaucoma seem to have more inferior visual field defects than patients without diabetes.18
Future Considerations
It is hoped that future studies will further elucidate the association of diabetes mellitus with open-angle glaucoma. Inhibition of angiogenic factors like vascular endothelial growth factor (VEGF) that lead to iris and angle neovascularization in diabetic retinopathy will be a new tool to treat neovascular glaucoma.40
GLAUCOMA ASSOCIATED WITH THYROID DISEASE
Definition
How Does Graves’ Disease Present Clinically?
Graves’ disease presents with hyperthyroidism with one or more of the triad of diffuse goiter, dermopathy, and ophthalmopathy. Graves’ disease usually occurs between the ages of 30 and 50, with women more often affected than men.
How Does Graves’ Disease Cause IOP Elevation?
Glaucoma can occur by several mechanisms including elevated episcleral venous pressure through infiltration of the orbital tissues, impaired outflow facility, and fibrosis of the extraocular muscles compressing the globe in the different positions of gaze and thus elevating the IOP.
The association between hypothyroidism and open-angle glaucoma is controversial.41,42 Systemic thyroid medication did lower IOP in patients with hypothyroidism.43–46 Thyroid disease might also be a risk factor for normal-tension glaucoma.47
Epidemiology and Importance
In one series 24% of patients with thyroid-associated orbitopathy (TAO) were noted to have an IOP greater than 22 mm Hg but less than 30 mm Hg.48 In another series of 482 patients, 4.8% of patients had open-angle glaucoma or IOP greater than 22 mm Hg.49 Only a prolonged duration of active TAO in association with ocular hypertension correlated with progression to glaucomatous damage.48,50
Diagnosis and Differential Diagnosis
It is important to differentiate visual field and optic nerve head changes in an individual with Graves’ disease from changes caused by compressive optic neuropathy related to the infiltrative thyroid orbitopathy.
Treatment and Management
Glaucoma due to thyroid eye disease is treated the same as chronic open-angle glaucoma. In patients with infiltrative ophthalmopathy, high-dose corticosteroids, radiotherapy, extraocular muscle surgery,49 and orbital decompression49,51,52 may be indicated for various reasons and may help in the management of the glaucoma.
Future Considerations
Future studies might be able to document a direct influence of thyroid hormone on the regulation of aqueous flow.
GLAUCOMA ASSOCIATED WITH VASCULAR DISEASES
Definition
Ocular ischemia from ophthalmic artery occlusion and internal carotid artery disease, and retinal ischemia from central retinal vein occlusion (CRVO), central retinal artery occlusion (CRAO), branch retinal vein occlusion (BRVO), and cerebrovascular disease, have all been shown to cause glaucoma. For management, see Figure 16–3.
Epidemiology and Importance
Why Are Vascular Occlusive Diseases of the Retina Important?
Ocular ischemia from occlusion of the ophthalmic artery and vascular occlusive disease of the retina can result in the development of rubeosis iridis and neovascular glaucoma. Ischemic CRVO is the most common cause of neovascular glaucoma in this group, with 60% of eyes developing iris neovascularization and 33% of eyes progressing to neovascular glaucoma. Ischemic hemispheric branch retinal vein occlusion (HRVO), nonischemic CRVO, and CRAO are all associated with the development of neovascular glaucoma to a much lesser extent. CRVO has been associated with systemic diseases such as cardiovascular disease, hypertension, and diabetes mellitus, systemic medications such as oral contraceptives and diuretics, and elevated IOP whether on an open-angle or angle-closure basis.53–59
Why Are Cerebrovascular Diseases Important?
Neovascular glaucoma may occur secondary to several cerebrovascular diseases such as carotid artery occlusive disease, giant cell arteritis, and Takayasu’s disease.56,60,61 Glaucoma secondary to elevated episcleral venous pressure has been associated with carotid-cavernous sinus fistulas and arteriovenous malformations (see Chapter 6).
Diagnosis and Differential Diagnosis
Screening gonioscopy in eyes with vascular occlusion, especially central retinal vein occlusion, is important to detect angle neovascularization before development of florid neovascular glaucoma.54,62 Carotid Doppler studies and echocardiogram further diagnose possible causes for ocular ischemia. In patients with symptoms of giant cell arteritis it might be necessary to obtain an erythrocyte sedimentation rate and a temporal artery biopsy.
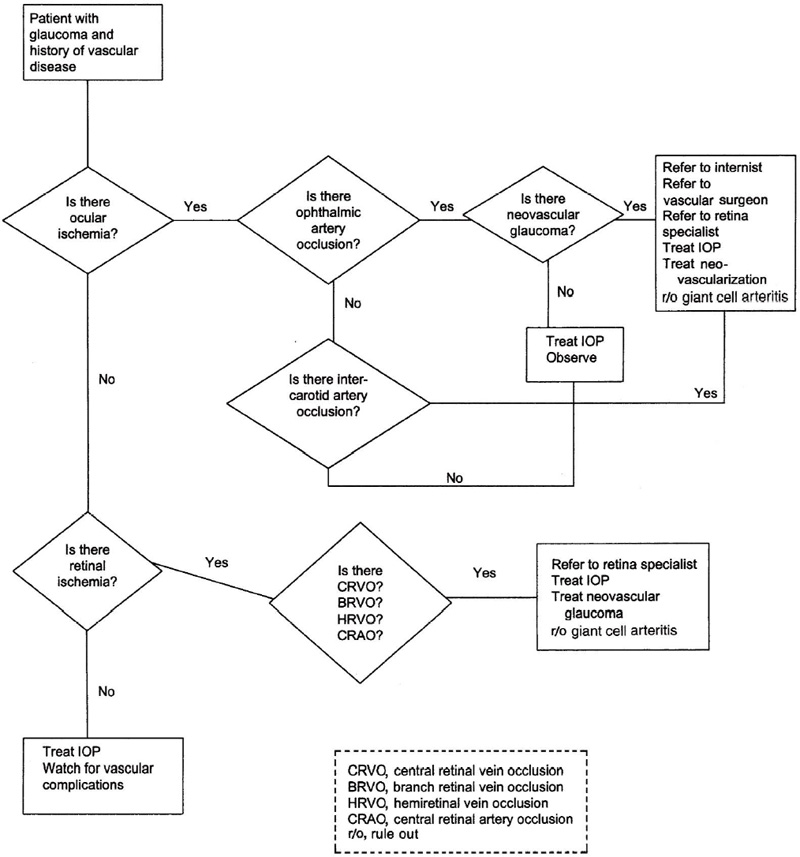
Figure 16–3. Management of a patient with glaucoma and vascular disease.
Treatment and Management
Treatment for glaucoma secondary to vascular occlusive disease of the retina is aimed at the underlying mechanism producing the glaucoma. Neovascular glaucoma is initially treated with cycloplegia, topical steroids, aqueous suppressants, and retinal laser photocoagulation. In patients with open angles and no evidence of neovascular glaucoma, elevated pressure in either eye should be reduced. Angle-closure glaucoma secondary to pupillary block requires an iridotomy. Non–pupillary block angle-closure glaucoma secondary to CRVO can in most cases be treated medically. Implantation of a glaucoma drainage device may be necessary if medical therapy fails to lower the IOP.
Prevention of neovascular glaucoma may be possible with prompt panretinal photocoagulation.54 Creating a chorioretinal anastomosis, applying recombinant tissue plasminogen activator, cannulating the retinal vein, transecting the posterior scleral ring, and using hemodilution have all been tried in the treatment of CRVO.63,64
Treatment of glaucoma secondary to cerebrovascular disease also is aimed at the underlying disease process. Carotid artery occlusive disease may produce neovascular glaucoma. Endarterectomy may be helpful in the management by preventing progressive infarction of ocular tissues. Therapy for glaucoma secondary to elevated episcleral venous pressure such as seen with arteriovenous malformations and carotid cavernous sinus fistulas is for the primary condition, and medical therapy is used to lower the IOP.
GLAUCOMA ASSOCIATED WITH COLLAGEN VASCULAR DISEASES
Definition
Open- or closed-angle glaucoma can occur with keratitis, episcleritis, scleritis, and uveitis in association with several collagen vascular diseases, like juvenile rheumatoid arthritis (JRA), rheumatoid arthritis (RA), scleroderma, Wegener’s granulomatosis, systemic lupus erythematosus and relapsing polychondritis. For management, see Figure 16–4.
Epidemiology and Importance
How Often Are Collagen Vascular Diseases Associated with Glaucoma?
Secondary glaucoma due to chronic uveitis can be seen in 14 to 27% of children affected with JRA.65–69 Four percent of patients with scleritis secondary to rheumatoid arthritis have been found to have glaucoma.70
Neovascular glaucoma is a known complication of collagen vascular disease. It has been found in patients with scleroderma,71 Wegener’s granulomatosis,72 and systemic lupus erythematosus.73 Relapsing polychondritis has been associated with uveitic glaucoma.74 Angle closure secondary to uveal effusion and posterior scleritis has been documented in patients with systemic lupus erythematosus.75,76
Diagnosis and Differential Diagnosis
It is important to keep in mind that patients presenting with uveitic or neovascular glaucoma can suffer from potentially life-threatening conditions, such as collagen vascular diseases. Appropriate workup and prompt referral to a specialist might be lifesaving.
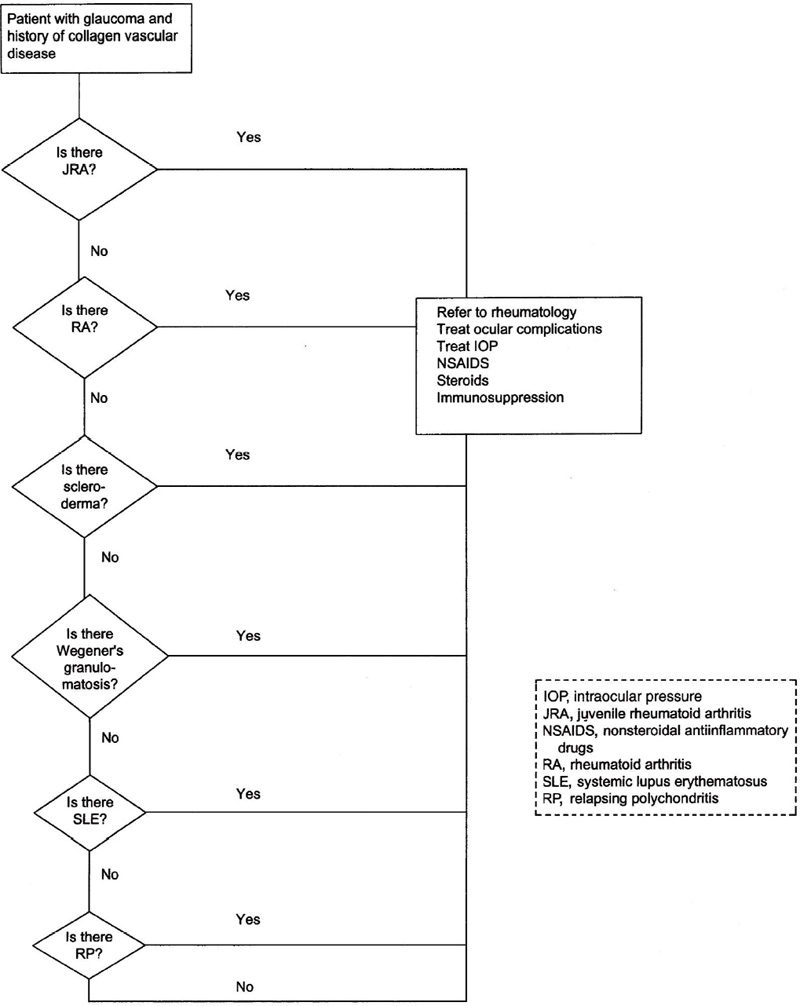
Figure 16–4. Management of a patient with glaucoma and collagen vascular disease.
Treatment and Management
How Is Glaucoma Associated with the Collagen Vascular Diseases Managed?
Treatment is directed at the underlying condition. The mainstay of therapeutics includes nonsteroidal antiinflammatory drugs and oral corticosteroids. Not infrequently immunosuppressive or cytotoxic agents are necessary to control the disease.
The associated uveitis is treated with topical and/or local corticosteroids and cycloplegics. Occasionally systemic corticosteroids are needed if the inflammation is severe. The secondary glaucoma can be treated medically with aqueous suppressants and occasionally surgically if necessary.
Treatment of neovascular glaucoma is described in Chapter 14.
GLAUCOMA ASSOCIATED WITH RENAL DISEASE AND HEMODIALYSIS
Definition
What Is the Relationship Between Renal Disease and Hemodialysis and Glaucoma?
Elevated IOP can be found in patients during and after hemodialysis,77 in patients following renal transplantation, and in patients with cystinosis.78 For management, see Figure 16–5.
Why Is the IOP Elevated in Some Patients During and After Hemodialysis?
During hemodialysis for chronic renal failure, changes in serum osmolality result in fluctuation in IOP. As serum osmolality falls, changes in the osmolality of the intraocular fluids do not occur simultaneously. This results in the flow of free water into the eye raising the IOP. The greater the reduction in outflow facility, the larger the gain in IOP tends to be.79–81
However, if an increase of plasma colloid osmotic pressure is induced by removing fluid during hemodialysis, a drop in IOP can be noted.82,83
How Is Renal Transplantation Associated with Glaucoma?
Up to one-third of the patients with renal disease requiring transplantation develop elevated IOP postoperatively. This appears to be a steroid response related to the use of systemic steroids to prevent transplant rejection.
By What Mechanism Can Cystinosis Cause Glaucoma?
Cystinosis is a rare metabolic disease characterized by the deposition of cystine crystals in many parts of the body, in particular the kidney and the eye. Cystine crystals have been found in the uvea, conjunctiva, and cornea. A peripheral pigmentary retinopathy can develop in childhood. There has been one report of a young adult with cystinosis who developed an attack of acute angle-closure glaucoma. Pathology specimens of the iris revealed the presence of cystine crystals in the iris stroma and in the iris pigmentary epithelium. Cystine crystals were also found in this patient’s conjunctival stroma and conjunctival mast cell granules. It was felt that the cystine crystals caused increased iris thickening and rigidity leading to angle closure.78
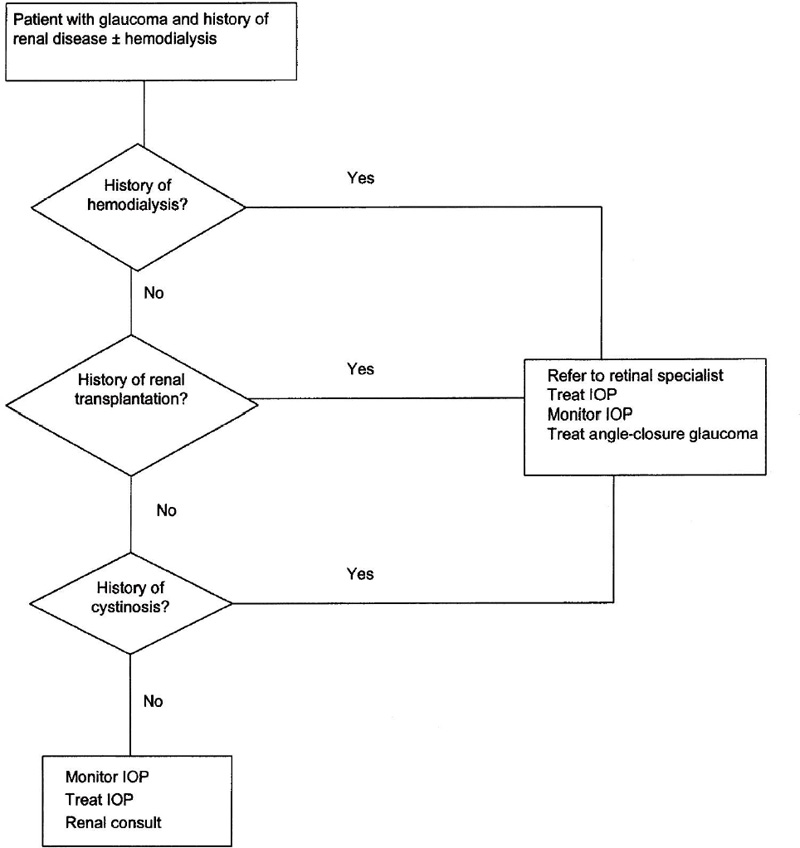
Figure 16–5. Management of a patient with glaucoma and renal disease and hemodialysis.
Epidemiology and Importance
Fluctuations of IOP occur during hemodialysis in patients with renal failure. During the first 2 hours of hemodialysis, a small decrease in IOP has been noted, followed by a rise in IOP after prolonged hemodialysis. An average rise in IOP of 7 mm Hg has been noted.84–86 However, it is not known if these changes are significant enough to cause glaucoma by itself in a nonglaucomatous eye.77,87–89 With newer hemodialysis techniques a significant change in IOP does not occur.90,91
Diagnosis and Differential Diagnosis
In patients with progressive glaucomatous optic neuropathy who are treated with hemodialysis, it might be helpful to monitor the IOP during and shortly after hemodialysis.
Treatment and Management
How Is Glaucoma Associated with Renal Disease and Hemodialysis Managed?
With current hemodialysis techniques, patients without a history of elevated IOP and/or decreased outflow facility are at a very low risk for developing glaucomatous optic neuropathy. On the other hand, eyes with uncontrolled glaucoma and seemingly good IOP control might have IOP spikes during or after hemodialysis. Acetazolamide has been found to prevent pressure spikes in this setting.92 However, acetazolamide has also been shown to cause severe metabolic acidosis in this setting.93
Steroid responders following renal transplantation can be successfully managed with medical therapy. Occasionally they will require glaucoma filtration surgery.
Is Glaucoma a Concern in Patients with Cystinosis?
Because cystinosis is a rare disease, relatively little is known about the treatment of secondary angle-closure glaucoma associated with this disease. Surgical trabeculectomy and iridectomy successfully treated the one case cited in the literature.78
GLAUCOMA ASSOCIATED WITH HEMATOLOGIC DISORDERS
Definition
Which Are the Main Hematologic Disorders Associated with Glaucoma?
Glaucoma has been found to be associated with the hyperviscosity syndromes and with the sickle cell hemoglobinopathies. For management, see Figure 16–6.
How Do the Hyperviscosity Syndromes Produce Glaucoma?
The hyperviscosity syndromes refer to a group of diseases that increase serum viscosity and subsequently decrease blood flow. The main clinical entities are polycythemia and the dysproteinemias. The reduction in blood flow results in dilation and tortuosity of the retinal veins. If a secondary central retinal vein occlusion occurs, neovascular glaucoma can develop.94,95 A 32-year-old man has been described who developed central retinal vein occlusion with resulting neovascular glaucoma after strenuous activity associated with dehydration.94
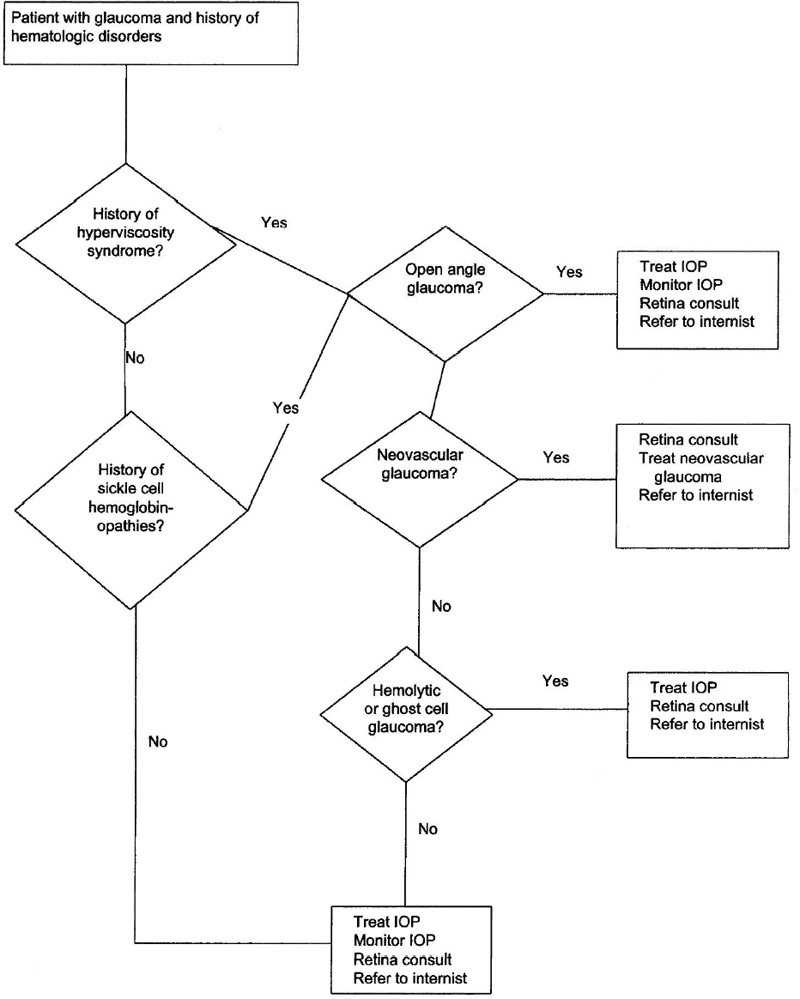
Figure 16–6. Management of a patient with glaucoma and hematologic discorders.
Does Blood Viscosity Play a Factor in the Etiology of Primary Open-Angle Glaucoma (POAG)?
There are some studies that suggest blood hyperviscosity may play a role in the etiology of POAG.96,97 However, its role and significance is not fully understood.
By What Mechanisms Can Sickle Cell Hemoglobinopathies Produce Glaucoma?
The sickle cell hemoglobinopathies refer to a group of diseases in which normal adult hemoglobin A is transformed into hemoglobin S, C, or O (Arab) through exchange of a single amino acid in its molecule. The main clinical entities are sickle cell anemia (HbSS), sickle cell trait (HbAS), sickle cell C disease (HbSC), and sickle cell S/O(Arab) disease [HbSO(Arab)]. In sickle cell thalassemia (HbSThal) synthesis of the hemoglobin molecule is impaired.
Under hypoxic conditions the red blood cells in these disorders develop a sickle configuration occluding small blood vessels.98,99 Both proliferative and nonproliferative sickle cell retinopathy can develop in the peripheral retina mainly in patients with sickle cell C disease and sickle cell thalassemia. Central retinal artery occlusion and central retinal vein occlusion can occur in conjunction with sickle cell anemia. Neovascular glaucoma can develop secondarily in these patients, mainly in patients with HbSC.100,101 Elevation of IOP might also occur secondary to a blood clot obstructing Schlemm’s canal.102,103 In addition, vitreous hemorrhage secondary to sickle cell retinopathy can cause hemolytic or ghost cell glaucoma.
Introduction of sickle cell erythrocytes into the anterior chamber causes sickling and may result in a large rise of IOP.104–106 The erythrocytes in the aqueous tend to sickle at a higher rate than in the circulation due to a higher level of ascorbate,107 or a fall in the pH or Po2 secondary to the hyphema.108 The sickled red blood cells clog the trabecular meshwork and reduce the facility of outflow.109
Patients with the sickle cell hemoglobinopathies are particularly susceptible to central retinal artery occlusion with mild elevation in the IOP110 or trauma.111,112
Epidemiology and Importance
How Often Are the Hyperviscosity Syndromes Associated with Glaucoma?
In one series, 6 out of 15 young patients were diagnosed with blood hyperviscosity associated with central retinal vein occlusion.95
How Often Is Sickle Cell Disease Associated with Glaucoma?
Approximately 8 to 10% of African Americans are asymptomatic carriers of one gene for sickle cell disease, and 0.3% carry two genes and therefore have the full-blown disease.98,99 Individuals with sickle cell disease seem to be more prone to have retinal disease and neovascular glaucoma100; however, individuals with sickle cell trait are at a significantly higher risk to develop ocular complications after trauma.113
Is Sickle Cell Disease a Risk Factor for Chronic Open-Angle Glaucoma?
Sickle cell disease by itself does not seem to be a risk factor for chronic open-angle glaucoma.114,115
Diagnosis and Differential Diagnosis
Every black patient presenting with a traumatic hyphema should be screened for sickle cell disease.116
Treatment and Management
How Is Glaucoma Associated with Hyperviscosity Syndromes Treated?
Neovascular glaucoma secondary to the hyperviscosity syndromes is treated with cycloplegics, topical steroids, aqueous suppressants, and retinal laser photocoagulation (see Chapter 14). Open-angle glaucoma secondary to thrombosis in Schlemm’s canal can be treated medically with aqueous suppressants.
How Is Neovascular Glaucoma in Patients with Sickle Cell Disease Treated?
Neovascular glaucoma secondary to the sickle cell hemoglobinopathies can be treated medically and with retinal laser photocoagulation. Proliferative sickle cell retinopathy is treated with laser photocoagulation to the involved quadrant; a central retinal artery occlusion or central retinal vein occlusion is treated with panretinal photocoagulation. Filtering surgery or implantation of a drainage device might be necessary (see Chapter 14).
How Is Ghost Cell Glaucoma Treated?
Ghost cell glaucoma secondary to associated vitreous hemorrhage is initially treated medically. However, a vitrectomy might be necessary to remove the cause of the ghost cell glaucoma, a nonresorbing vitreous bleed.
Is Glaucoma Secondary to Trauma Treated Differently in Patients with Sickle Cell Disease?
Certain precautions must be taken when treating elevated IOP secondary to hyphema in sickle cell hemoglobinopathy patients.116,117 Because mild elevation in IOP can produce irreversible visual loss, aggressive treatment of increased IOP in sickle cell hemoglobinopathy patients must be undertaken. Anterior chamber paracentesis might be warranted.110,118,119 However, certain medications should be avoided. Acetazolamide can increase the concentration of ascorbic acid in the aqueous, leading to increased sickling of red blood cells in the anterior chamber. Acetazolamide also acts on the kidneys, leading to a metabolic acidosis with secondary increased intravascular sickling and to increased blood viscosity due to its diuretic side effects. It also increases the ascorbic acid levels in the anterior chamber.107 Methazolamide is much less likely to cause these adverse side effects. Hyperosmolar agents may also increase serum viscosity, leading to vascular compromise in the eye. Epinephrine, apraclonidine, and brimonidine probably should be avoided due to their vasoconstrictive properties reducing anterior chamber oxygenation.120–122 In these patients, if the IOP averages greater than 24 mm Hg for any 24-hour period or if there are any spikes in IOP greater than 30, consideration should be given to draining the hyphema by either paracentesis (small hyphemas) or surgically (larger hyphemas).117,123–126
Future Considerations
The topical use of aminocaproic acid seems to be promising to prevent complications such as rebleeding in the treatment of patients with traumatic hyphema.127,128
GLAUCOMA ASSOCIATED WITH AMYLOIDOSIS
Definition
What Is Amyloidosis?
The term amyloidosis describes a group of disorders characterized by extracellular deposition of a substance called amyloid in various tissues. Amyloid consists of delicate protein fibrils that are able to bind Congo red and show green birefringence in polarized light. The relative lack of solubility of these fibrils in physiologic solvents and their resistance to normal digestion is of primary importance. Amyloid deposits may occur in various tissues and organs throughout the body (systemic amyloidosis) or at one specific site (localized or organ-limited).129,130 For management, see Figure 16–7.
How Does Amyloidosis Cause Glaucoma?
Glaucoma has primarily been associated with primary familial amyloidosis.129 In this condition, vitreous opacities are the main ocular finding. Amyloid is also found deposited in the eyelids, lacrimal glands, orbit, orbital nerves, extraocular muscles, conjunctiva, cornea, uveal tract, and retinal vessels. Secondary glaucoma may develop due to deposition of amyloid material in the trabecular meshwork.131–134 Orbital deposition of amyloid causing an increase of episcleral venous pressure has been shown in one case to cause secondary glaucoma.135
A high percentage of patients with familial amyloidosis (Finnish type) with lattice corneal dystrophy (Meretoja’s syndrome) also have glaucoma.136 In these eyes amyloid has also been found in the trabecular meshwork, explaining glaucoma in these patients.137
Epidemiology and Importance
How Often Is Amyloidosis Associated with an Increased IOP and/or Glaucoma?
In different series, glaucoma has been associated with primary familial amyloidosis in 5%,138 6.6%,139 and four out of 15 cases.133 In one series of patients with Meretoja’s syndrome, glaucoma was found in 23%.136
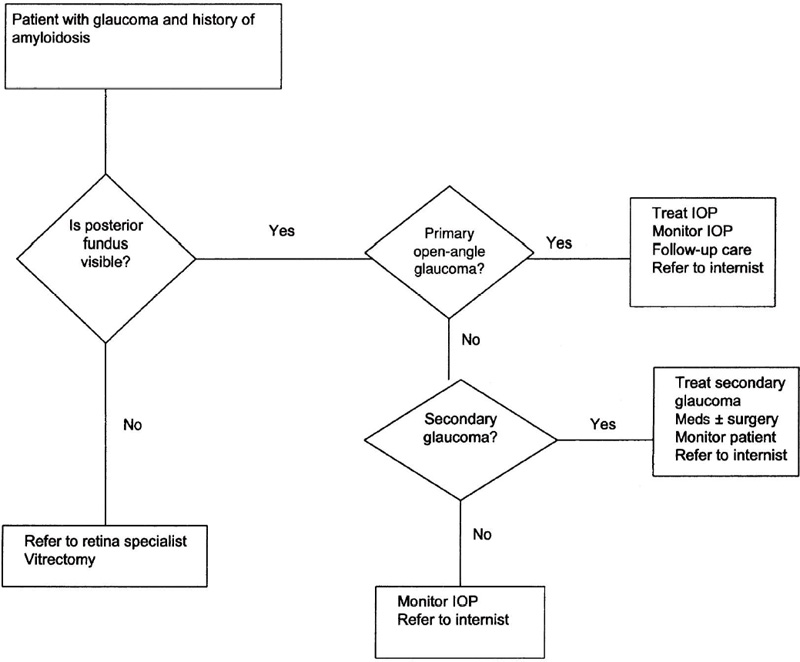
Figure 16–7. Management of a patient with glaucoma and amyloidosis.
Diagnosis and Differential Diagnosis
How Is Glaucoma Associated with Amyloidosis Diagnosed?
Tsukahara and Matsuo133 examined the eyes of 15 patients with primary familial amyloidosis and found four patients with glaucoma. These glaucomatous patients all had the following in common: (1) systemic symptoms of primary familial amyloidosis, (2) an older age with a longer duration of the disease, (3) vitreous opacities, (4) open angles with pigment deposition in the angles, (5) white flocculent material in the pupillary margin, and (6) a flaky substance on the anterior lens surface, resembling pseudoexfoliation.
Treatment and Management
How Is Glaucoma Associated with Amyloidosis Treated?
Glaucoma secondary to primary familial amyloidosis is treated like open-angle glaucoma with medical therapy followed by surgery for recalcitrant cases.
However, these cases are difficult to follow as the vitreous opacities obscure visualization of the optic nerve head and may hamper interpretation of the visual fields. Vitrectomy can be used to establish the diagnosis and to improve visual function and better visualize the posterior pole. Unfortunately, Doft et al140 found that 17% of eyes requiring vitrectomy for vitreous amyloidosis were complicated by the development of glaucoma requiring filtration surgery. The conjunctiva might be rather fragile in these eyes, requiring very delicate surgical technique.134 Epstein141 noted that survival of filtering blebs may be complicated by the deposition of amyloid within the bleb.
Future Considerations
Amyloidosis is still poorly understood. Further genetic studies will help in the understanding of this group of diseases and gene therapy might be available some day to prevent deposition of amyloid material in organ tissue and thus prevent organ damage such as glaucoma.
GLAUCOMA ASSOCIATED WITH IRRADIATION
Definition
How Is Glaucoma Associated with Irradiation Defined?
Major radiation complications to the eye include radiation cataract, neovascular glaucoma (NVG), retinopathy, and scleral necrosis (in descending order of incidence).142,143 Radiation to the eye will cause damage to the retinal, choroidal, and iris vascular, resulting in capillary hypoperfusion and eventually neovascularization of the anterior chamber angle.144 Elevation of the IOP may follow and, with damage of the optic nerve, cause NVG. For management see Figure 16–8.
Epidemiology and Importance
How Often Is Irradiation Associated with an Increased IOP and/or Glaucoma?
The incidence of NVG after irradiation of periocular malignancies is 7%. The onset of symptoms occurred a median of 22 months after irradiation (50 Gy).145
In studies that had a follow-up period of less than 6 months, the incidence of glaucoma was less than 2%.146,147 However, 5 years after plaque radiotherapy of 136 eyes with ciliary body melanomas, 21% of eyes had developed NVG. In this study the development of NVG was significantly related to iris involvement with the ciliary body tumor.142 Including all uveal melanomas treated with plaque radiotherapy, 15 to 19% of eyes treated with a median apical tumor dose of approximately 100 Gy developed NVG after 5 to 10 years.148,149 If treated with low-dose radiation (20 Gy) for choroidal hemangiomas, one out of 51 eyes developed NVG.150
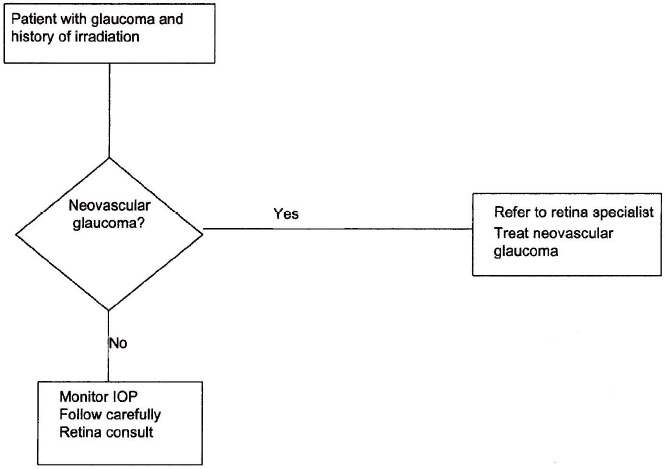
Figure 16–8. Management of a patient with glaucoma and history of irradiation.
Diagnosis and Differential Diagnosis
How Is Glaucoma Associated with Irradiation Diagnosed?
Because neovascular glaucoma can occur months to years after irradiation of the eye, regular careful examination of the iris and anterior chamber angle for neovascularization is of paramount importance. The differential diagnosis includes all other causes of neovascular glaucoma (see Chapter 14).
Treatment and Management
How Is Neovascular Glaucoma Associated with Irradiation Treated?
The treatment of neovascular glaucoma is described in Chapter 14.
Future Considerations
Early detection of intraocular tumors and advanced radiation techniques with concentration of treatment inside the tumor will be beneficial in decreasing long-term ocular complications.
GLAUCOMA ASSOCIATED WITH SYSTEMIC VIRAL DISEASE
Definition
How Is Glaucoma Associated with Viral Diseases Defined?
Viral ocular infections are a significant source of patient morbidity throughout the world. No part of the eye is immune to viral invasion. Viral infections can give rise to keratitis, scleritis, and/or uveitis, which then can lead to decreased aqueous outflow and thus elevated IOP and glaucoma. For management, see Figure 16–9.
HERPESVIRUS
Herpesviruses are DNA viruses. They can infect a variety of animals, including humans. More than 50 different viruses are known; however, only five of this group can cause ocular disease in humans. These are herpes simplex virus type 1 (HSV-1), herpes simplex virus type 2 (HSV-2), varicella-zoster virus (VZV), cytomegalovirus (CMV), and Epstein-Barr virus (EBV).151 Secondary to the viral infection a keratitis, scleritis, and/or uveitis may occur, which can give rise to an elevated IOP and thus glaucoma.
Herpes Simplex Virus Herpes simplex virus (HSV) infection may present as superficial keratitis, disciform keratitis, necrotic stromal keratitis, neurotrophic ulcer, and retinitis. Increased IOP in ocular herpes infection associated with uveitis varies from 28 to 40%, but only 10% have secondary glaucoma.152,153 Disciform and necrotic stromal keratitis is more commonly associated with increased IOP. In severe cases the incidence can reach 80%.152 Obstruction of the trabecular meshwork with inflammatory products, trabeculitis,152,154 and acute155 and chronic156 angle closure are the most common cause for IOP elevation in herpetic uveitis. Most recently, HSV has been identified in the trabecular meshwork of a patient with keratitis and glaucoma requiring filtering surgery.157
The initial management of elevated IOP is directed at controlling viral replication. Oral and/or topical acyclovir and topical trifluridine are most effective because they penetrate the ocular tissues easily. Topical cycloplegics are helpful to control ciliary spasm, and topical corticosteroids may be used if inflammation is severe or persists despite the antiviral treatment. Topical steroids alone can reactivate or aggravate the herpetic infection. They therefore should never be used without initial antiviral coverage. IOP usually returns to normal levels when the inflammation subsides. Aqueous suppressants are effective if IOP needs to be controlled. About 10% of patients who have persistent IOP elevation despite medical treatment may require surgery.152
Varicella-Zoster Virus VZV is the etiologic agent of the most common primary infectious childhood disease, varicella or chickenpox. In its recurrent form it may cause herpes zoster or shingles, as it reactivates from the latent stage established during primary illness. Ninety percent of the population in the United States are seroconverted by age 60. When VZV reactivates from its latent form involving the first branch of the trigeminal nerve, it is referred to as herpes zoster ophthalmicus (HZO).158 VZV reactivates as zoster in one out of five people during the course of a lifetime. Skin lesions involving the side or the tip of the nose suggest ocular involvement because of involvement of the nasal branch of the nasociliary nerve (Hutchinson’s sign). HZO is rare in children; it tends to be short-lived, not as painful as in adults, and leaves little to no scarring. In some cases it may be the initial presentation of AIDS; any young person presenting with HZO should be tested for human immunodeficiency virus (HIV) infection.
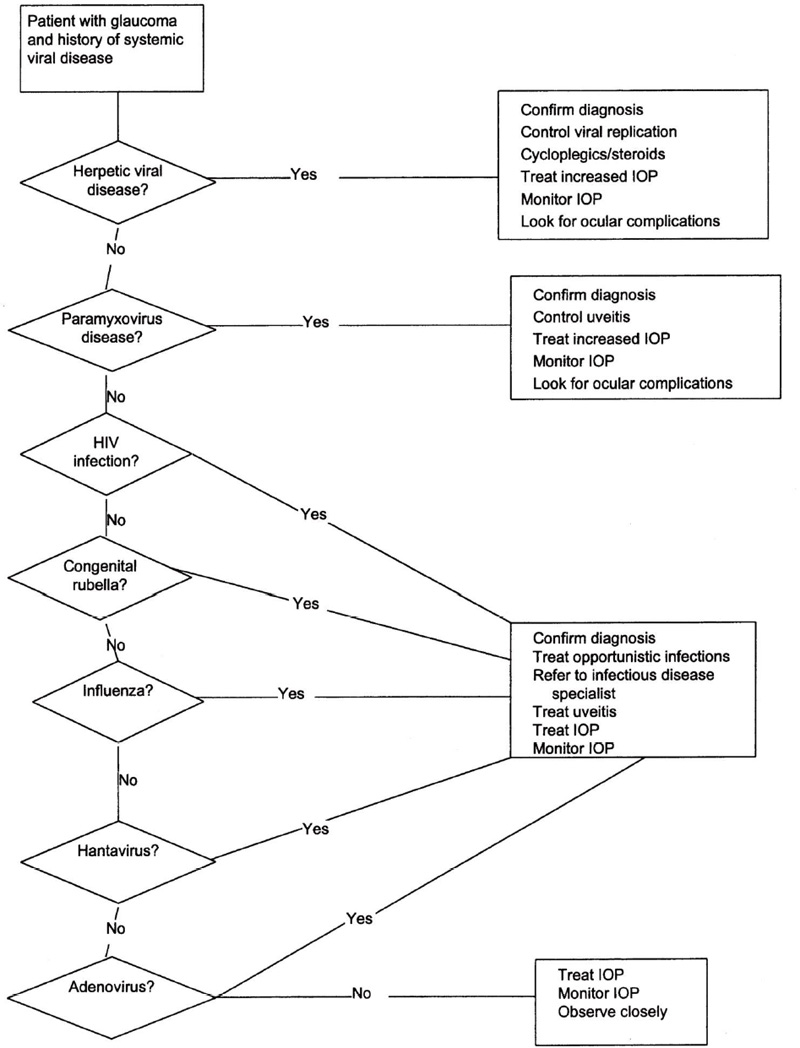
Figure 16–9. Management of a patient with glaucoma and systemic viral disease.
Ocular involvement occurs in two-thirds of patients with HZO. This might include conjunctivitis, superficial keratitis, stromal keratitis, neurotrophic keratitis, uveitis, scleritis, retinitis, choroiditis, and optic neuritis. Elevation of IOP and glaucoma occurs in 16 to 50% of cases if the keratitis and uveitis is associated with corneal involvement.159–161 Decreased outflow facility due to trabeculitis and inflammatory debris in the trabecular meshwork is thought to cause the IOP elevation.162,163 Oral acyclovir given early in the course of the disease seems to reduce the risk of complications, such as uveitis and associated elevated IOP.164 Later in the course of the disease uveitis is no longer due to viral replication, but rather to ischemia.165
Uveitis and IOP should then be treated with topical corticosteroids, mydriatics, and aqueous suppressants as indicated.
Cytomegalovirus Infection with cytomegalovirus (CMV) is very common among the general population, but in most cases the disease is not clinically apparent. In immunocompromised patients and neonates, it is the cause of significant morbidity and mortality. In older children and young adults, CMV can cause a syndrome resembling infectious mononucleosis and can be associated with a nonspecific follicular conjunctivitis. Infection in patients with AIDS will present as a retinitis. It is the most common ocular infection in patients with AIDS in the United States.166
Epstein-Barr Virus Epstein-Barr virus (EBV) is the most common cause of infectious mononucleosis with the classic triad of fever, sore throat, and lymphadenopathy. Seropositivity in the general population is over 90% and transmission occurs primarily through saliva, but also through blood transfusions. It can cause oculoglandular syndrome, follicular conjunctivitis, keratitis, uveitis, retinitis, and papillitis. Treatment consists of oral acyclovir.167,168 IOP elevation may occur, but glaucoma has not been documented.
PARAMYXOVIRUS
Measles Measles causes an acute infection characterized by fever, cough, coryza, and conjunctivitis. Ocular findings are initially limited to the conjunctiva. During this prodromal phase, virus is spread throughout the reticuloendothelial system and within the subepithelial conjunctival lymphoid tissue, resulting in conjunctivitis. A watery-mucoid discharge is usually present. The conjunctivitis is self-limiting and usually resolves as fever defervesces.
Measles can affect the cornea, resulting in a superficial punctate keratitis, initially involving the limbus with later spread to the central cornea. Lesions of the cornea appear to peak after the appearance of the measles rash. Postmeasles blindness (PMB) is a significant complication of measles, as a result of optic neuritis, chorioretinitis, or complications of corneal origin. In Africa 14 to 33% of childhood blindness is due to measles.169 Complicating this is the increased susceptibility of PMB in patients with vitamin A deficiency, concomitant herpes simplex infection, and/or the use of folk remedies.169,170 Ocular therapy is mainly supportive, unless bacterial superinfection is evident. Vitamin A supplementation may be useful in those deemed deficient.
HUMAN IMMUNODEFICIENCY VIRUS (HIV)
Ocular manifestations of HIV infection include noninfectious microangiopathy (HIV retinopathy), opportunistic ocular infections, ocular adnexal neoplastic involvement, and neuro-ophthalmic lesions. Opportunistic ocular infections such as CMV retinitis, VZV retinitis, fungal retinitis, and pneumocystosis can all cause secondary uveitis and lead to IOP elevation and thus glaucoma. Bilateral angle closure has been associated with HIV infection.171–176 Choroidal effusion with secondary anterior rotation of the ciliary body at the scleral spur could be diagnosed with ultrasound biomicroscopy.171,173 Treatment consists of application of aqueous suppressants, cycloplegics, and topical steroids.
CONGENITAL RUBELLA
The last rubella epidemic in the United States occurred in 1964. An estimated 10% of pregnant women were exposed to the virus; 2% of women developed clinical rubella, 40% of those in the first trimester. Approximately 10% of mothers with clinical rubella had children with the congenital rubella syndrome.177 In the U.S., at least 10,000 infants were born with moderate to severe manifestations during that epidemic.178 In a 20-year follow-up study, ocular disease was noted in 78% of patients, sensorineural hearing loss in 66%, psychomotor retardation in 62%, cardiac abnormalities in 58%, and mental retardation in 42%.179 Ocular consequences of the congenital rubella syndrome are not limited to abnormalities noted in the neonatal period. Additional abnormalities may appear years and even decades after birth. In a series of 34 rubella patients, 29 (85%) of patients had a cataract, in 21 of these they were bilateral. Microphthalmia was present in 28 of these of infants (82%), and it was bilateral in 22. Glaucoma occurred in 32% (11 cases). In 11 eyes of six of these patients, glaucoma occurred months to years after cataract surgery.180 In a series of 13 patients, glaucoma was diagnosed 3 to 22 years after birth. The eyes involved were microphthalmic in all but two cases. In all cases the lens had been removed early in life due to cataract.181
Congenital rubella syndrome, especially when associated with microphthalmia, was found to be a risk factor for development of glaucoma after cataract surgery in childhood.179,182
INFLUENZA
Influenza is an acute febrile illness characterized by malaise, headache, and myalgias. The illness lasts 2 to 7 days. Recovery is complete unless secondary bacterial infections occur. Influenza can be serious and may cause cardiopulmonary complications or death in elderly or debilitated patients. Ocular involvement with influenza includes conjunctivitis, a mild iritis, interstitial keratitis, dacryoadenitis, and retinitis.183 Primary angle-closure glaucoma has been reported in three cases.184
HANTAVIRUS INFECTIONS
Viruses of the Hantavirus genus (HTV) chronically infect rodents without apparent disease, but when they are spread by aerosolized excreta to humans, two major clinical syndromes result: hemorrhagic fever with renal syndrome (HFRS) and Hantavirus pulmonary syndrome (HPS). Both diseases appear to be immunopathologic, and inflammatory mediators are important causing clinical manifestations. In HPS, T cells act on heavily infected pulmonary endothelium, and it is suspected that γ-interferon and tumor necrosis factor are major agents of a reversible increase in vascular permeability that leads to severe, noncardiogenic pulmonary edema. HFRS has prominent systemic manifestations. The retroperitoneum is a major site of vascular leak, and the kidneys suffer tubular necrosis. Both syndromes are accompanied by myocardial depression and hypotension or shock. HFRS is primarily a Eurasian disease and is caused by the Puumala, Hantaan, and Seoul viruses, whereas HPS appears to be confined to the Americas. The Sin Nombre and New York-1 viruses have been implicated as the etiologic agent.185,186 Ophthalmic symptoms have been reported with Puumala virus infections in 82% of patients with HFRS; 41% reported photophobia and 50% impaired vision.187 In another study, frontal headache or periocular pain was noted in 76%, blurred vision in 54%, and photophobia in 11% of patients; 41% were noted to have a myopic shift, and 14% had signs of anterior uveitis. A decrease of the IOP was found in 66% of patients.188 One patient was described to have a myopic shift secondary to thickening of the lens and forward displacement of the iris-lens diaphragm, and low IOP probably secondary to electrolyte imbalance.189 Angle-closure attack has also been reported.190,191
ADENOVIRUS
Adenovirus can produce a wide range of ocular infections, ranging from follicular conjunctivitis to severe keratoconjunctivitis with corneal opacities. Adenovirus 8 and 19 are commonly implicated with epidemic keratoconjunctivitis and types 3, 4, 7, and 14 with pharyngoconjunctival fever. The risk of visual impairment is greater with the epidemic form of keratoconjunctivitis. Elevated IOP has been described with adenovirus type 10 keratoconjunctivitis.192
Future Considerations
Advances in antiviral therapy will make it possible to better treat ocular viral infections and thus prevent a complication such as glaucoma. Multiple agents for the treatment and prevention of viral illnesses have been developed during the past few years. This has been to a great extent in direct response to the HIV virus type 1 epidemic.193,194 In addition, gene therapy might soon be available to treat viral diseases.195
GLAUCOMA ASSOCIATED WITH PARASITIC DISEASE
Definition
What Parasitic Diseases Can Cause Glaucoma?
Parasitic infections of the eye can be caused by protozoans and by helminthes. In response to the ocular infection, a keratitis, scleritis, or uveitis can occur, which subsequently can cause the IOP to rise and eventually can lead to uveitic glaucoma. Among the protozoans Toxoplasma gondii, ameba (Acanthamoeba), Leishmania, and Plasmodium have been shown to cause elevated IOP and/or glaucoma. Among the helminthic diseases Onchocerca, Toxocara, Cysticercus, Echinococcus, Loa loa, Schistosoma, Trichinella, and others have been shown to cause ocular infections that may lead to glaucoma. For management, see Figure 16–10.
GLAUCOMA CAUSED BY PROTOZOAN DISEASES
Definition
What Is Toxoplasmosis and How Does It Affect the Eye?
Toxoplasmosis is an infectious disease characterized by fever, weight loss, and lymphadenopathy. It is caused by T. gondii, which is an obligate intracellular protozoan found in most parts of the world. The cat or its close feline relatives appear to be the definite hosts. The oocysts, which are excreted in cat feces, are highly resistant and may remain infective for more than 1 year. Usually only young cats are infective for a short period of time. The infected cat is not the primary source of infection for humans, but it is a very important cause of contamination of the environment.196 Ocular toxoplasmosis is usually considered a recurrence of a congenital infection, but can also be acquired postnatally.197,198 In the eye, the retinal tissue and adjacent choroid are the site of infection. The typical ocular lesion is a localized necrotizing retinitis or satellite lesion of an existing scar. Cells are present in the overlying vitreous causing the characteristic appearance of a “headlight in the fog.”
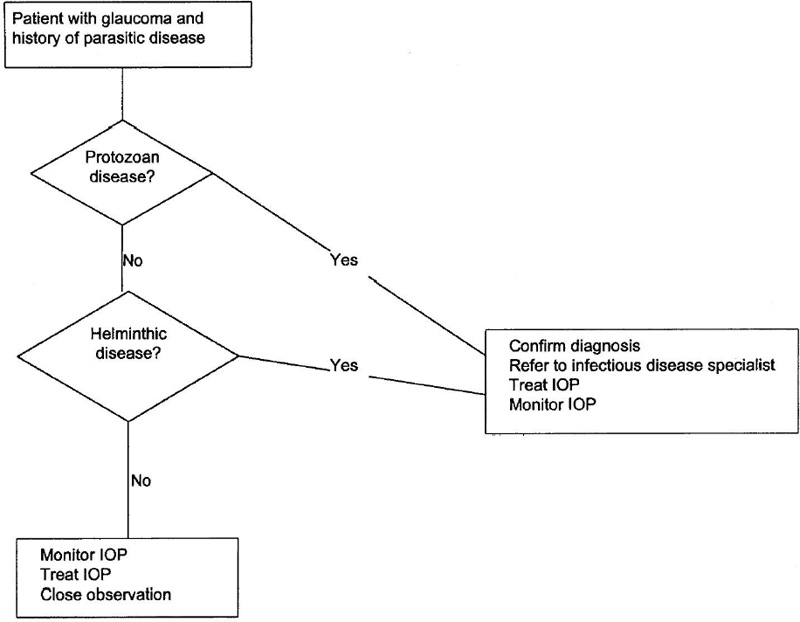
Figure 16–10. Management of a patient with glaucoma and parasitic disease.
What Is Acanthamoebiasis and How Does It Affect the Eye?
Acanthamoeba species are an important cause of microbial keratitis that may cause severe ocular inflammation and visual loss. Like other protozoa, Acanthamoeba are unicellular and can exist in two forms: active trophozoite and dormant cyst. The trophozoite is motile, proliferates, and feeds on bacteria, fungi, and other unicellular organisms and cells, like corneal epithelium.199
What Is Leishmaniasis and How Does It Affect the Eye?
Leishmania protozoa are obligate intracellular parasites and are transmitted by bites of infected sand flies. Leishmaniasis presents as either cutaneous or visceral (kala-azar or dumdum fever) leishmaniasis depending on the Leishmania species and immune status of the patient. In ocular disease, the adnexae are most commonly involved,200 but anterior uveitis with elevated IOP and glaucoma have been reported.201–204
What Is Malaria and How Does It Affect the Eye?
Malaria is caused by infection with the protozoans Plasmodium falciparum, vivax, malariae, and ovale. It is transmitted through a bite by the female mosquito of the genus Anopheles. Malaria is characterized by fever with sweats, myalgia, headaches, malaise, and sometimes rigors.
Ocular complications occur especially with cerebral malaria. They include retinal hemorrhages, disc swelling, and retinal edema.205
What Is Trypanosomiasis and How Does It Affect the Eye?
African trypanosomiasis (African sleeping sickness) is caused by Trypanosoma brucei and transmitted by bites of the tsetse fly. American trypanosomiasis (Chagas’ disease) is caused by Trypanosoma cruzi or wrangle. Chagas’ disease has multiple modes of transmission: vector-borne (reduviid bugs) by contamination of the bite wound with vector feces, congenital, and transfusional.206 Intraocular involvement is rare and may consist of retinal pigment epithelial changes.207
Epidemiology and Importance
How Common Is Toxoplasmosis?
Toxoplasmosis is the most common cause of posterior uveitis. In the U.S. approximately 3,000 infants are infected annually.208 In an adult population the annual incidence for ocular involvement is approximately 0.3 per 100,000 population,209 and 3% of patients with acquired toxoplasmosis have ocular disease.210
How Common Is Glaucoma in Toxoplasmosis?
Transient open-angle glaucoma occurs in about 13% of patients.211
How Common Is Acanthamoeba Keratitis?
Acanthamoeba is a ubiquitous, free-living protozoan that is found in all types of liquid media, including tap water, swimming pools, hot tubs, and contaminated contact lens solution. The organism’s prevalence seems to peak during warmer weather. The first cases of Acanthamoeba keratitis were recognized in 1975, but the disease remained very rare until the 1980s, when an increase in incidence mainly associated with contact lens wear was reported.199
How Common Is Glaucoma in Acanthamoeba Keratitis?
Secondary uveitic glaucoma has been reported but is rarely a problem.212,213
How Common Is Leishmaniasis?
Leishmaniasis is a worldwide disease. Kala-azar (visceral leishmaniasis) has reemerged from near eradication. The annual estimate incidence and prevalence of kala-azar cases worldwide is 0.5 million and 2.5 million, respectively. Of these, 90% of the confirmed cases occur in India, Nepal, Bangladesh, and Sudan.214
How Common Is Glaucoma in Leishmaniasis?
Intraocular involvement in leishmaniasis is rare, but probably underdiagnosed.
How Common Is Malaria?
Malaria is the most important infectious disease in the world with 300–500 million cases and approximately 2 million deaths per year.215
How Common Is Glaucoma in Malaria?
Glaucoma is a rare complication of malaria. There are only two reports in the literature about glaucoma secondary to malaria.216,217
How Common Is Trypanosomiasis?
In Africa 60 million people are at risk of infection with human African trypanosomiasis or sleeping sickness, with about 300,000 new cases each year. However, only 10% of cases are probably diagnosed and treated.218 In Central and South America, Chagas’ disease is of great epidemiologic importance; 100 million persons are at risk of infection, approximately 18 million are infected, and 50,000 deaths annually can be attributed to the disease.219 The reservoir for the protozoa T. cruzi involves over 175 species.206
How Common Is Glaucoma in Trypanosomiasis?
Glaucoma has not been reported, but a marked postural drop of the IOP has been noted, possibly secondary to changes in the autonomic innervation secondary to the parasitic infection.220
Diagnosis and Differential Diagnosis
How Is Toxoplasmosis Diagnosed?
Classic ocular toxoplasmosis is diagnosed clinically. The typical ocular lesion is a localized necrotizing retinitis or satellite lesion of an existing chorioretinal scar. Cells are present in the overlying vitreous causing the characteristic appearance of a “headlight in the fog.” The anterior segment of the eye may also be involved in the inflammatory process. An anterior uveitis, which can be either granulomatous or nongranulomatous in character, can be seen only in an eye with an active toxoplasmosis lesion of the retina. Therefore, all patients presenting with an anterior uveitis should have a dilated examination of the retina to rule out an underlying disorder of the posterior segment.221
Laboratory tests can be used to help confirm the clinical diagnosis. More and more, polymerase chain reaction techniques are replacing the Sabin-Feldman test, which uses live Toxoplasma organisms, complement fixation, and enzyme-linked immunosorbent assays.222
What Are the Ocular Complications of Toxoplasmosis?
Complications of ocular toxoplasmosis occur in approximately one-third of patients and include chronic iridocyclitis, cataracts, band keratopathy, cystoid macular edema, retinal detachment, and optic atrophy. Transient open-angle glaucoma occurs in about 13% of patients.211 An interesting association with Fuchs’ heterochromic iridocyclitis has been reported; however, its causal relationship is unproven and controversial.223–225
How Does Acanthamoeba Keratitis Present and How Is It Diagnosed?
The clinical picture is often characterized by severe pain with an early superficial keratitis that is often treated as herpes simplex infection. Subsequently, a characteristic radial perineural infiltration may be seen, and ring infiltration is common. Limbitis and scleritis are frequent.226 Laboratory diagnosis is primarily by culture of epithelial samples inoculated onto agar plates spread with bacteria. Recently, Hartmannella has also been shown to cause amebic keratitis.227
How Is Leishmaniasis Diagnosed?
In endemic areas the diagnosis is made on clinical grounds. A definite diagnosis of leishmaniasis is made by documenting the parasite in smears of bone marrow, splenic aspirates, or in biopsies from cutaneous lesions.228 Ocular leishmaniasis is diagnosed by the temporal relationship to the systemic manifestation. However, the parasite has also been isolated from the anterior chamber.203,204
What Are the Ocular Complications of Leishmaniasis?
Most commonly the ocular adnexae are involved,200 but anterior uveitis with elevated IOP and glaucoma have been reported.201–204
How Is Malaria Diagnosed?
The diagnosis is made by demonstrating plasmodia in thick blood smears of suspected individuals.229
What Are the Ocular Complications of Malaria?
The Plasmodium causes hemolysis with anemia, which can lead to blotchy retinal hemorrhages,216 disc swelling, and vitreous hemorrhage.205 Bilateral iridocyclitis with elevated IOP217 and bilateral panuveitis with uveitic glaucoma216 have been reported.
How Is Trypanosomiasis Diagnosed?
Patients with African trypanosomiasis present with irregular fevers, enlarged lymph nodes, delayed sensation to pain, and skin rash. Definitive diagnosis depends on the demonstration of the parasite in blood, lymph node aspirates, bone marrow, and cerebrospinal fluid.
Acute Chagas’ disease should be suspected in any individual from endemic areas with acute febrile illness with lymphadenopathy and myocarditis. Definitive diagnosis is made through documentation of the parasite in the blood.
What Are the Ocular Complications of Trypanosomiasis?
If in Chagas’ disease the route of inoculation is through the conjunctiva, Romaña’s sign (periorbital edema, conjunctivitis, and dacryocystitis) may be present.230 A marked postural drop of the IOP has been noted, possibly secondary to changes in the autonomic innervation secondary to the parasitic infection.220
Treatment and Management
The treatment of ocular complications of protozoan diseases has to be directed against the underlying parasitic infection. Topical symptomatic therapy (i.e., corticosteroids, cycloplegics, and aqueous suppressants) can be initiated as indicated.
How Is Glaucoma Associated with Toxoplasmosis Treated?
The treatment of ocular toxoplasmosis remains controversial, in particular due to side effects. Some lesions, if far enough in the ocular periphery of an immunocompetent host, can simply be followed up. The most commonly used treatment regimens consist of pyrimethamine, sulfadiazine, and corticosteroids, or pyrimethamine, clindamycin, and corticosteroids. Treatment usually lasts for 3 to 4 weeks, with careful attention to platelet counts if pyrimethamine is used, even though folinic acid is always added to the treatment regimen. Treatment of patients with AIDS cannot be stopped. More recently, atovaquone has been introduced as a therapeutic alternative.231
How Is Acanthamoeba Keratitis Treated?
A variety of topically applied therapeutic agents are thought to be effective, including propamidine isethionate, clotrimazole, polyhexamethylen biguanide, and chlorhexidine. Penetrating keratoplasty is preferably avoided in inflamed eyes, but may be necessary in severe cases to preserve the globe or, when the infection has resolved, to restore corneal clarity for optical reasons.226
How Is Glaucoma Associated with Leishmaniasis Treated?
The standard therapy for the underlying systemic infection consists of pentavalent antimonials (e.g., sodium stibogluconate or meglumine antimoniate).232 In addition, liposomal amphotericin B has recently been approved by the United States Food and Drug Administration for treatment as well.233 The associated uveitic glaucoma can be treated with topical corticosteroids, cycloplegics, and aqueous suppressants as indicated.201,202
How Is Glaucoma Associated with Malaria Treated?
Concomitant to systemic antimalarial therapy,215,229 topical corticosteroids, cycloplegics, and aqueous suppressants can be given as indicated.216,217
How Is Trypanosomiasis Treated?
All drugs currently used to treat African trypanosomiasis are very toxic and require prolonged administration. They include eflornithine, suramin, pentamidine isethionate, melarsoprol, and nifurtimox. Two percent of patients treated for central nervous system (CNS) disease experience relapse.
Although numerous drugs have been tried, including those used to treat African trypanosomiasis and leishmaniasis, few have proven to be effective for therapy of Chagas’ disease. Nifurtimox and benznidazole have both been tried in conjunction with allopurinol.234
Future Considerations
Treatment of uveitic glaucoma secondary to infectious diseases ultimately has to be directed against treatment and prevention of the underlying infection. Vector control,159 prevention of infection,215 development of vaccines,214,235 and development of new chemotherapeutic agents236,237 are all important in achieving this goal.
GLAUCOMA CAUSED BY HELMINTHIC DISEASES
Definition
What Is Onchocerciasis (River Blindness)?
Onchocerciasis is caused by the parasite Onchocerca volvulus. The parasite is spread through bites of the black fly genus Simulium. After infection with the larva into connective tissue, it matures to filiform adults and may remain in tissues for years. Clinical manifestations vary according to the parasitic load, previous immunity, and duration of infection. A distressing, pruriginous dermatitis and subcutaneous nodules, which are produced by the inflammatory reaction to dying parasites, are very typical. Female adults produce large amounts of microfilaria that migrate through skin and connective tissue. Once an infected host is bitten, the infectious larvae develop again in the female Simulium black fly and the life cycle is completed.238
How Does Onchocerciasis Affect the Eye?
Infection with this tissue nematode may cause keratitis with corneal scarring chorioretinitis, optic neuritis, and uveitis with and without glaucoma.
What Is Toxocariasis?
Toxocara canis and cati are common intestinal parasites of dogs and cats with humans as natural hosts. Toddlers are usually affected by contact with puppies or eating dirt soiled by infected animals. In infected humans, the larvae spread hematologically and are found in multiple organs. The larvae migrate throughout the body for months or years before they complete their full life cycle, therefore the name visceral larva migrans for the disorder.
How Does Toxocariasis Affect the Eye?
Granuloma formation in the posterior segment and diffuse endophthalmitis represent the ocular manifestations. Rare larval migration within the anterior segment can lead to granulomatous uveitis and glaucoma.239–244
What Is Cysticercosis and How Does It Affect the Eye?
Cysticercosis results from infection with ingested eggs of the tapeworm Taenia solium. Oncospheres are released from the hatching eggs and migrate into the intestinal wall and disseminate via blood and lymph vessels and form fluid-filled bladder worms (cysticerci) throughout the body.245,246 Intraocular involvement can cause uveitis and secondary IOP elevation.
Epidemiology and Importance
How Common Is Onchocerciasis?
The habitat of the Simulium black fly is around rivers and streams in western and central Africa, central and northern South America, and the Arabian Peninsula. Onchocerciasis is the fourth leading cause of worldwide blindness and is responsible in endemic areas for blindness in millions.247 Infection in travelers is rare but is being recorded on a regular basis.238
How Often Is Onchocerciasis Associated with an Increased IOP and/or Glaucoma?
In Sierra Leone, uveitic glaucoma was reported in 11 of 1,625 individuals with onchocerciasis.248 In an endemic area for onchocerciasis in Nigeria, optic nerve disease was found in 9% of the population. In 50% of these cases onchocerciasis was thought to be the etiology either through direct involvement of the optic nerve or less likely secondary to uveitic glaucoma.
How Common Is Toxocariasis?
In puppies 2 to 6 months of age, the prevalence of T. canis is reported to be 80%. In the U.S. the disease is more prevalent in the south central and southeastern regions. From 10 to 30% of soil samples from public playgrounds and parks are contaminated with T. canis eggs.241
How Common Is Cysticercosis?
Infection most commonly occurs in areas where pigs and people are in close contact, hygienic standards are low, and undercooked pork is eaten. In some rural areas of Central America, the prevalence of Taeniasis is up to 9.8% of the total population, and autopsy data suggest that up to 3.6% of the population of Mexico have neurocysticercosis.245,246 Two to seven percent of individuals with cysticercosis have ocular involvement.249
Diagnosis and Differential Diagnosis
How Is Onchocerciasis Diagnosed?
Onchocerciasis has traditionally been diagnosed by skin snipping and parasitologic examination; however, screening for palpable skin nodules has been found to be a reliable method to identify communities at serious risk for the disease.250
How Is Toxocariasis Diagnosed?
Diagnosis is made clinically with the help of enzyme-linked immunosorbent assays and cytologic diagnosis of intraocular aspirates.241–243
How Is Cysticercosis Diagnosed?
Cysticercosis can be diagnosed by documenting parasites in biopsy specimen or fine needle aspirates of palpable subcutaneous nodules. Stool examinations positive for adult T. solium constitute supporting evidence. In addition, the diffuse “millet seed” appearance of soft tissue calcifications are also pathognomonic for cysticercosis.245,246,251
Treatment and Management
How Is Onchocerciasis Treated?
Until 1987, suramin and diethylcarbamazine were the only drugs available for the treatment of onchocerciasis, and they could not be used for community therapy because of their toxicity and the dosage schedules required. The introduction of annual oral treatment with ivermectin and the donation of this drug by Merck & Co. provided a new opportunity for the safe treatment and control of the disease. Data indicate a significant reduction of microfilarial loads and regression of early lesions of the anterior segment, including iridocyclitis and sclerosing keratitis. Ivermectin was also found to have a beneficial effect on optic-nerve disease and visual field loss.252
Concurrent uveitis and elevated IOP is treated with topical antiinflammatory agents and aqueous suppressants as indicated.
How Is Ocular Toxocariasis Treated?
Treatment of ocular toxocariasis can be very difficult. Eradication of the parasite without damage to the ocular tissue due to the dying parasite is the goal. This can be achieved by combining medical therapy (i.e., oral thiabendazole or albendazole) with surgical removal of the parasite. Topical corticosteroids, cycloplegics, and aqueous suppressants are given as indicated to control inflammation and IOP.241–243
How Is Cysticercosis Treated?
Treatment consists of medical therapy with praziquantel or albendazole. However, in cases of neurocysticercosis and intraocular involvement, surgical removal of the parasite should be attempted before initiating medical therapy because a severe inflammatory reaction can occur due to the dying parasite. Resulting uveitic glaucoma can be treated with topical steroids, cycloplegics, and aqueous suppressants as indicated.245,246,253–255
ADDITIONAL HELMINTHIC INFECTIONS
Many other parasites can infest ocular and intraocular tissues and thus can cause inflammation and secondary IOP elevation with glaucoma. The following parasites have been isolated from intraocular tissues: Echinococcus multilocularis,256–258 Loa loa,259,260 Schistosoma,261 Gnathostoma,262,263 Dracunculus,264 Wucheria,265,266 and Paragonimus,267,268 Several nematodes, including Baylisascaris and Toxocara, have been found as a causative agent in diffuse unilateral subacute neuroretinitis.269–272
Future Considerations
Screening of communities at risk for parasitic disease, vector and parasite control,159,244 and education,273 along with development and supply of new medications to endemic regions worldwide, will be needed to significantly decrease these diseases’ incidence and morbidity274–279
GLAUCOMA ASSOCIATED WITH DERMATOLOGIC DISORDERS
Definition
How Can Dermatologic Disorders Cause Glaucoma?
Several dermatologic conditions also affect the ocular structures involved in aqueous outflow, which can cause elevation of the IOP and thus glaucoma if optic neuropathy occurs. Some conditions can cause uveitis and associated elevated IOP with possible resulting uveitic glaucoma. For management, see Figure 16–11.
Which Dermatologic Disorders Can Cause Glaucoma?
ROSACEA
Rosacea is a dermatologic condition that frequently affects the eyes. It is characterized by meibomian gland dysfunction and recalcitrant chronic blepharitis. Rosacea can cause keratitis, episcleritis, and iridocyclitis, which in return can cause secondary obstruction of the outflow pathways with resulting elevated IOP.280
VOGT-KOYANAGI-HARADA SYNDROME
Vogt-Koyanagi-Harada (VKH) syndrome is associated with bilateral panuveitis and neurologic and dermatologic manifestations. Uveitic glaucoma occurs in every third patient with VKH syndrome281 (see Chapter 8).
BEHÇET’S DISEASE
Behçet’s disease, which presents with acute hypopyon, iritis, aphthous and genital ulcers, and erythema nodosum in young adults, can also cause uveitic glaucoma in a significant number of adults.
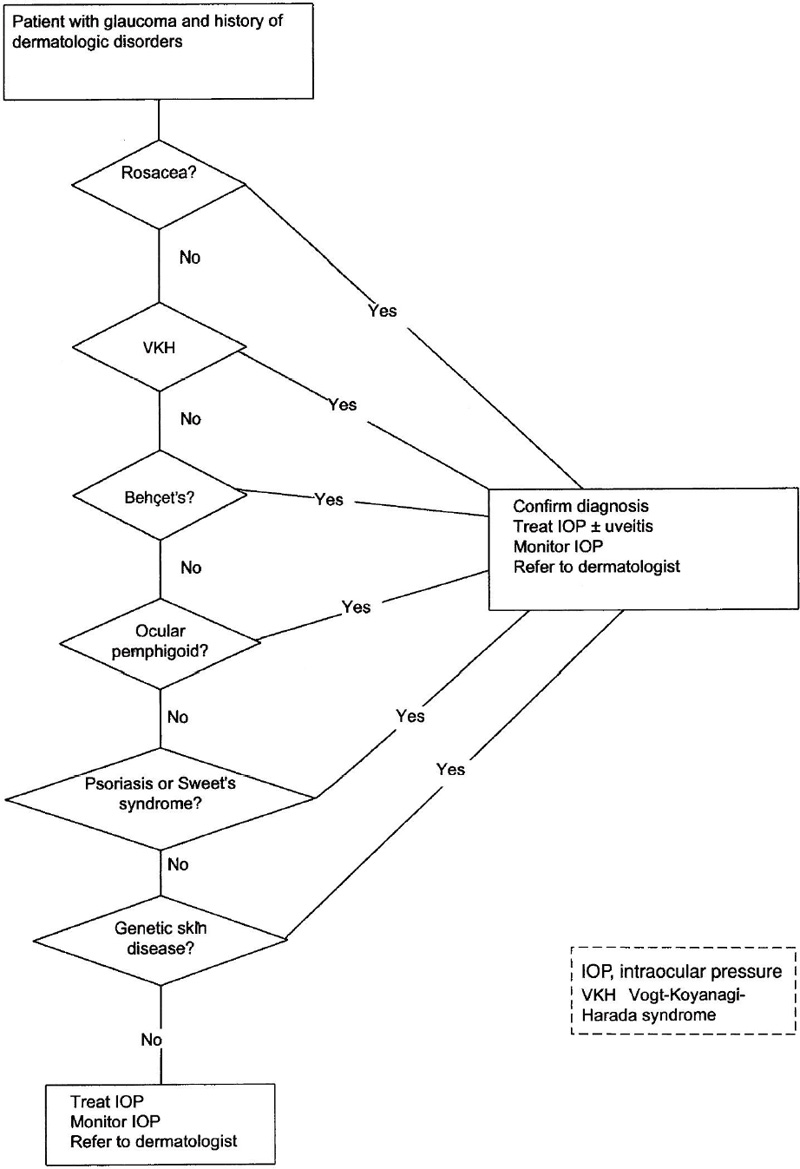
Figure 16–11. Management of a patient with glaucoma and dermatologic disorder.
OCULAR CICATRICIAL PEMPHIGOID
Ocular cicatricial pemphigoid has also been associated with glaucoma282; however, in many cases the disease is probably secondary to the topical antiglaucoma medications used.283
PSORIASIS AND SWEET’S SYNDROME
Psoriasis284 and Sweet’s syndrome285 have been found to cause intraocular inflammation and uveitic glaucoma.
Are There Any Genetic Skin Disorders that Cause Glaucoma?
Rothmund-Thomson syndrome is a rare autosomal recessive disorder with the characteristic skin changes of poikiloderma congenitale, small stature, mental deficiency, and a higher than expected incidence of malignancy. Ocular findings include juvenile cataracts and glaucoma.286–288 In a series of 22 cases with cutis marmorata, two infants were reported to have glaucoma.289
In several phacomatoses, especially Sturge-Weber syndrome, glaucoma can be seen (see Chapter 1).
Are There Other Dermatologic Conditions Known to Cause Glaucoma?
Local and systemic scleroderma,290–292 oculodermal melanocytosis (nevus of Ota),293 and juvenile xanthogranuloma (see Chapter 17) are known to cause glaucoma.
Treatment and Management
How Is Glaucoma Associated with Dermatologic Disorders Treated?
Therapy is primarily aimed at the underlying dermatologic condition, if possible. Uveitic glaucoma is treated with antiinflammatory agents and aqueous suppressants as indicated. Infantile glaucoma is generally treated surgically; however, aqueous suppressants may play a role as well.
GLAUCOMA ASSOCIATED WITH NEUROLOGIC DISORDERS
Definition
Certain neurologic disorders may be associated with glaucoma. For management, see Figure 16–12.
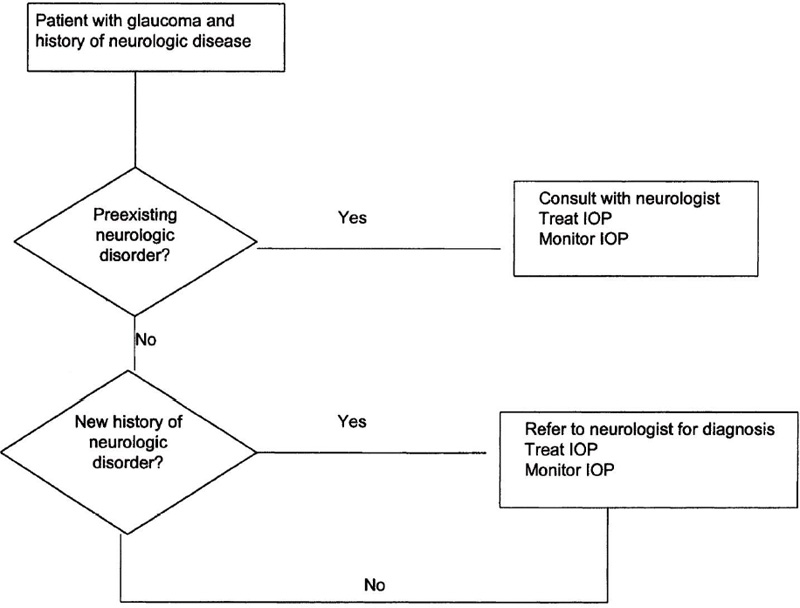
Figure 16–12. Management of a patient with glaucoma and neurologic disorders.
Does the Central Nervous System Regulate the IOP?
A central nervous system influence on the regulation of the IOP has been studied extensively. However, the full extent of its regulatory role has not been established. The IOP can be regulated by neural and/or humoral influences on the rate of aqueous humor formation.294,295 The role of the hypothalamus in this regulatory process has been studied extensively.296 A hypothalamic center sensitive to osmotic pressure has been thought to regulate the IOP by efferent optic nerve fibers.297 Their full role still remains unclear.298 In addition to that, injection of oxytocin into the cat hypothalamus raises the IOP.299
The sympathetic nervous system clearly influences aqueous humor dynamics by influencing the diurnal rhythm of aqueous flow.300 Autonomic dysfunction in glaucoma has been postulated.301,302 Centrally acting Il-imidazoline receptor agonists have been shown to lower the IOP.303 In rabbits, the suprachiasmatic nucleus seems to be involved in the diurnal regulation of the IOP.304
In myotonic dystrophy ocular hypotony is quite common.305 It is controversial whether this is due to a central effect through elevated endogenous circulating gonadotropins resulting in elevated cyclic adenosine monophosphate (AMP) and decreased aqueous humor production306 or to locally increased uveoscleral outflow.307
Epidemiology and Importance
Is Glaucoma Associated with Any Neurologic Disorders?
Although it seems clear that the central nervous system exerts some influence on the regulation of the IOP, no neurologic disorder per se is known to cause glaucoma by the mechanism of IOP elevation. A significant number of patients with Alzheimer’s disease also have glaucoma. Again, a causal relationship has not been established.308 Diurnal IOP variations seem to be higher in patients with open-angle glaucoma.309
References
6. Kass MA, Sears ML: Hormonal regulation of intraocular pressure. Surv Ophthalmol 1977;22:153–176.
9. Ray S, Mehra KS, Misra S, et al: Plasma cortisol in glaucoma. Ann Ophthalmol 1977;9:1151–1154.
14. Ohrloff C, Stoffel C: Intraocular pressure in Cushing’s syndrome. Exp Eye Res 1975;20:170–176.
23. Mitchell P, Smith W, Chey T, et al: Open-angle glaucoma and diabetes: the Blue Mountains eye study, Australia. Ophthalmology 1997;104:712–718.
26. Katz J, Somber A: Risk factors for primary open-angle glaucoma. Am J Rev Med 1988;4:110–114.
28. Armstrong J: The incidence of glaucoma in diabetes mellitus. Am J Ophthalmol 1960;50:55–63.
29. Bankes JL: Ocular tension and diabetes mellitus. Br J Ophthalmol 1967;51:557–561.
38. Smith JP: Angle closure glaucoma and acute hyperglycemia. Arch Ophthalmol 1987;105:454–455.
55. Sperduto RD, Hiller R, Chew E, et al: Risk factors for hemiretinal vein occlusion: comparison with risk factors for central and branch retinal vein occlusion: the eye disease case-control study. Ophthalmology 1998;105:765–771.
60. Carter JE: Chronic ocular ischemia and carotid vascular disease. Stroke 1985;16:721–728.
68. Kanski JJ: Anterior uveitis in juvenile rheumatoid arthritis. Arch Ophthalmol 1977;95:1794–1797.
69. Kanski JJ: Uveitis in juvenile chronic arthritis. Clin Exp Rheumatol 1990;8:499–503.
73. Matsui M: [Ophthalmological aspects of systemic vasculitis]. Nippon Rinsho 1994;52:2158–2163.
84. Burn RA: Intraocular pressure during hemodialysis. Br J Ophthalmol 1973;57:511–513.
87. Broekema N, van Bijsterveld OP, de Bos Kuil RJ: Intraocular pressure during hemodialysis. Ophthalmologic 1988;197:60–64.
98. Steinberg MH: Management of sickle cell disease. N Engl J Med 1999;340:1021–1030.
116. Jeffers JB: Traumatic hyphema management. Curr Concepts Ophthalmol 1995;3:34–38.
117. Liebmann JM: Management of sickle cell disease and hyphema. J Glaucoma 1996;5:271–275.
118. Goldberg MF: The diagnosis and treatment of sickled erythrocytes in human hyphemas. Trans Am Ophthalmol Soc 1978;76:501–507.
122. Robin AL: The role of alpha-agonists in glaucoma therapy. Curr Opin Ophthalmol 1997;8:42–49.
130. Gorevic PD, Rodrigues MM: Ocular amyloidosis. Am J Ophthalmol 1994;117:529–532.
143. Finger PT: Radiation therapy for choroidal melanoma. Surv Ophthalmol 1997;42:215–232.
149. Bacin F, Kwiatkowski F, Dalens H, et al: [Long-term results of cobalt 60 curietherapy for uveal melanoma]. J Fr Ophtalmol 1998;21:333–344.
181. Boger WP III: Late ocular complications in congenital rubella syndrome. Ophthalmology 1980;87:1244–1252.
193. Zerr DM: Advances in antiviral therapy. Curr Opin Pediatr 1999;1–21.
196. Rothova A: Ocular involvement in toxoplasmosis. Br J Ophthalmol 1993;77:371–377.
200. Sodaify M, Aminlari A, Resaer H: Ophthalmic leishmaniasis. Clin Exp Dermatol 1981;52:481–483.
202. Dechant W, Rees PH, Kager PA, et al: Post kala-azar uveitis. Br J Ophthalmol 1980;64:680–683.
210. Perkins ES: Ocular toxoplasmosis. Br J Ophthalmol 1973;57:1–17.
214. Bora D: Epidemiology of visceral leishmaniasis in India. Natl Med J India 1999;12:62–68.
215. Baird JK, Hoffman SL: Prevention of malaria in travelers. Med Clin North Am 1999;83:923–945.
216. Biswas J, Fogla R, Srinivasan P, et al: Ocular malaria. Ophthalmology 1996;103:1471–1475.
226. Illingworth CD, Cook SD: Acanthamoeba keratitis. Surv Ophthalmol 1998;42:493–508.
232. Davidson RN: Practical guide for the treatment of leishmaniasis. Drugs 1998;56:1009–1018.
235. Tonui WK: Leishmania transmission-blocking vaccines: a review. East Afr Med J 1999;76:93–96.
238. Okhuysen PC: Onchocerciasis in an expatriate living in Cameroon. J Travel Med 1997;4:11–13.
239. Liesegang TJ: Atypical ocular toxocariasis. J Pediatr Ophthalmol 1977;14:349–353.
241. Shields JA: Ocular toxocariasis. A review. Surv Ophthalmol 1984;28:361–381.
242. Molk R: Ocular toxocariasis: a review of the literature. Ann Ophthalmol 1983;15:216–231.
245. Kitchen LW: Case studies in international medicine. Am Fam Physician 1999;59:3040–3044.
246. Yamashita P, Kelsey J, Henderson SO: Subcutaneous cysticercosis. J Emerg Med 1998;16:583–586.
251. Khurana N, Jain S: Cytomorphological spectrum of cysticercosis—a review of 132 cases. Indian J Pathol Microbiol 1999;42:69–71.
260. Renard G: [Ocular manifestations of loiasis]. J Fr Ophtalmol 1978;1:86.
264. Verma VK: Ocular dracontiasis. Int Surg 1968;50:508–509.
267. Wang WJ, Xin YJ, Robinson NL, et al: Intraocular paragonimiasis. Br J Ophthalmol 1984;68:85–88.
268. Verin P, Comte P: [A case of ocular paragonimiasis]. Bull Soc Ophtalmol Fr 1984;84:997–999.
280. Browning DJ, Proia AD: Ocular rosacea. Surv Ophthalmol 1986;31:145–158.
283. Liesegang TJ: Conjunctival changes associated with glaucoma therapy: implications for the external disease consultant and the treatment of glaucoma. Cornea 1998;17:574–583.
284. Knox DL: Psoriasis and intraocular inflammation. Trans Am Ophthalmol Soc 1979;77:210–224.
296. Waitzmann MB: The hypothalamus and ocular pressure. Surv Ophthalmol 1971;16:1.
298. Trzeciakowski JP: Central control of intraocular pressure. J Ocul Pharmacol 1987;3:367–378.
300. Potter DE: Adrenergic pharmacology of aqueous humor dynamics. Pharmacol Rev 1981;33:133–153.
305. Dreyer RF: Ocular hypotony in myotonic dystrophy. Int Ophthalmol 1983;6:221–223.
309. David R, Zangwill L, Briscoe D, et al: Diurnal intraocular pressure variations: an analysis of 690 diurnal curves. Br J Ophthalmol 1992;76:280–283.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


