![]() 17
17 ![]()
Glaucoma Associated with Intraocular Tumors
David J. Bene
Definition
What Is Glaucoma Associated with Intraocular Tumors?
Elevated intraocular pressure (IOP) may be the presenting sign of an intraocular tumor. Typically, this secondary and unilateral glaucoma is dependent on the type, location, and stage of the tumor. The trabecular meshwork can be compromised by several mechanisms resulting in open- or closed-angle glaucoma.
What Types of Intraocular Tumors May Be Associated with Glaucoma?
The most common tumors to be associated with glaucoma are uveal melanoma, retinoblastoma, and metastases to the iris, ciliary body, and choroid. Occasional reports of medulloepithelioma, lymphoma, leukemia, systemic hamartosis (neurofibromatosis, oculodermal melanocytosis, and encephalotrigeminal hemangiomatosis), juvenile xanthogranuloma, and nevus of Ota are found in the literature.1–10
When Does One Suspect that Glaucoma Is Secondary to an Underlying Intraocular Tumor?
Intraocular tumor is suspected if there is elevated IOP and asymmetry of the optic nerves. Shields et al2 established 23 mm Hg as the arbitrary lower limit for elevated IOP. A detailed history to elicit the presence of systemic cancer (especially breast, lung, or leukemia), skin lesions (neurofibromas, café-au-lait spots, or nevus of Ota), or buphthalmos may lead to the suspicion of ocular involvement. A clinical examination including slit-lamp biomicroscopy, gonioscopy, and indirect ophthalmoscopy may reveal the presence of an atypical mass.
Epidemiology and Importance
What Age Groups Develop Glaucoma Associated with Intraocular Tumors?
There are many intraocular tumors that develop during infancy and childhood that may be associated with glaucoma. Juvenile xanthogranuloma10 is usually apparent in infants and young children. It is rarely seen in adults. It is a benign histiocytic proliferation commonly of the skin with formation of Touton giant cells. However, the iris is the most common extracutaneous site and is frequently associated with hyphema. This tumor is a highly vascularized tan-yellow-to-brown lesion within the iris. Frequently, this is a self-limited tumor that may regress with time.
Retinoblastoma, the most common childhood intraocular malignancy, is associated with inactivation of both alleles of the retinoblastoma gene on the long arm of chromosome 13. Undetected at birth or in adults, retinoblastoma usually presents in unilateral cases at age 23 months and bilaterally at age 1 year.11 The cumulative lifetime incidence of retinoblastoma is approximately 1/15,000 individuals. Inheritance of retinoblastoma can be a result of somatic or germinal factors. However, the majority of retinoblastoma cases are sporadic in nature.12 Histologically, retinoblastomas are recognized by the presence of Flexner-Wintersteiner rosettes. Retinoblastoma has a strong propensity to invade optic nerve, choroid, and scleral emissary canals. Clinically, Ellsworth13 described leukocoria and strabismus as the most frequent initial presentations of retinoblastoma; glaucoma occurred initially in 7% of eyes.
Neurofibromatosis is the most common phakomatosis. This neuroectodemal tumor with autosomal dominant inheritance may involve multiple organs. Neurofibromatosis is classified as type I or type II. Neurofibromatosis type I is peripheral, mapped to chromosome17qll, and is associated with multiple cutaneous café-au-lait spots, presence of optic nerve glioma, multiple Lisch nodules, and inguinal and axiliary freckling.14 Neurofibromatosis type II is central, mapped to chromosome 22q22, and is associated with acoustic neuromas, peripheral nerve sheath tumors, and posterior subcapsular cataracts.15 Neurofibromatosis may present in the first year of life as a congenital glaucoma especially when associated with eyelid involvement or ipsilateral facial hemihypertrophy. François syndrome14 is a type of peripheral neurofibromatosis consisting of unilateral buphthalmos, homolateral facial hemihypertrophy, and homolateral plexiform neuroma of the eyelid.16,17
Medulloepithelioma is a rare congenital tumor typically diagnosed at 2 to 4 years of age, but it may appear in adults as well.18 Clinically, when medulloepithelioma involves the iris, a tan-to-pink mass replaces the normal peripheral iris and invades the angle. In contrast, when medulloepithelioma arises from the ciliary body, a tan-to-white lesion may be observed within the pupil by indirect ophthalmoscopy or slit-lamp examination. Absences of zonules, lens coloboma, and cataract have been associated findings.19 Histologically, this lesion is composed of primitive neuroectodermal cells arising from the non pigmented epithelium of the ciliary body. A variety of atypical histologic findings may be present including cartilage and striated muscle.
Nevus of Ota is a unilateral accumulation of melanocytes within the dermis and is associated with ipsilateral pigmentation of the lids and periorbita. This hamartoma is distributed in the ophthalmic and maxillary divisions of the fifth cranial nerve. Pigmentation may be present in the iris, cornea, fundus, optic disc, sclera, and conjunctiva. Most cases are sporadic; however, in some familial cases an autosomal recessive inheritance is present. There is a 4:1 female to male predilection for the occurrence of nevus of Ota.20 The associated glaucoma, more frequent in blacks and Orientals, usually develops in the age group of 20 to 40 years. As shown by Gonder et al,21 whites with nevus of Ota rarely develop glaucoma.
Iris melanocytoma is rare with only incidental case reports in the literature.7,8,21 This benign tumor tends to occur on the inferior iris typically in the fourth decade of life. However, this tumor may undergo malignant transformation. Melanocytomas are frequently present in black or dark-complexioned individuals. Ocular pain, injection, and keratitic precipitates may be the initial presenting signs. Histologically, this tumor is composed of large uniform polygonal cells with small, bland nuclei with intensely pigmented cytoplasm.8 Association with glaucoma has been reported by Shields et al19 in a 23-year-old and by Gonder et al21 in a 7-year-old white girl and in similar patients in their second and third decade of life.21 Croxatto et al22 reported a case of optic disc melanocytoma associated with angle-closure glaucoma in a 44 year old, and there are other reports in the literature.23–25 Iris melanomas usually develop in the fourth decade, whereas most posterior uveal melanomas are diagnosed in patients after the fifth decade.26
Systemic large-cell lymphoma occurs in middle-aged or older patients; it is a form of non-Hodgkin’s lymphoma and is a systemic malignancy. The eye is infrequently involved but can be associated with glaucoma.27 Clinically, large cell lymphoma presents as a bilateral nongranulomatous uveitis that is eventually recalcitrant to topical steroids. Lymphoma cells massively infiltrate the uveal tract and vitreous cavity.
Metastatic tumors are the most common intraocular malignancies. Approximately 10% of patients who die of cancer have evidence of ocular or orbital metastasis, with the choroid being the most common metastatic site.28,29 Metastasis occurs most frequently at ages 40 to 70 from primary cancer of the breast, lung, or gastrointestinal or genitourethral systems.30 However, metastatic cancer may present in children and adults from leukemia. Leonardy et al4 histologically examined the eyes from 135 patients who died of leukemia. Leukemic ocular infiltrates were found in 31.1% of the patients with the choroid as the most frequently involved site. Metastatic tumors may present to the iris but it is rare. Shields et al31 found that of 512 patients with uveal metastasis only 7.8% had iris involvement. Bronchial carcinoid, breast, and lung carcinomas were the most common primary malignancy. These patients complained of blurred vision, redness, and ocular pain. Clinically, iris metastases are fleshy, yellow-white friable masses that release tumor cells into the anterior chamber. It has been reported that the incidence of a secondary glaucoma is 38% with patients in iris metastasis. Iris metastasis is usually seen in adults, but metastatic neuroblastoma is seen in children.31
What Is the Incidence of Glaucoma Associated with Various Intraocular Tumors?
The association of glaucoma with intraocular tumors was reported as early as 1896 by Marshall.32 The prevalence of tumor-associated glaucoma is largely dependent on tumor type, location, and stage,7,33 as well as on the investigator’s study design. Comparison of various studies produces varied results often dependent on analysis of histologic specimens versus clinical data. Yanoff34 studied the histologic sections of 96 eyes enucleated for melanoma, comparing the 19 eyes with glaucoma (both open- and closed-angle forms) to the 77 without glaucoma. His data confirmed the increased risk of glaucoma in large posterior tumors with total retinal detachment, as well as the increased incidence of glaucoma with anterior (iris and ciliary body) melanomas. Ciliary body melanoma alone was not an increased risk factor for glaucoma.
Shields et al2 retrospectively evaluated the intraocular pressure of 2,704 eyes with intraocular tumors that were referred to Wills Eye Hospital from 1974 to 1986. Only those eyes with IOP elevation due to tumor and with pressures greater than 23 mm Hg were included in the study. Only 5% of the eyes with tumors presented with glaucoma (Table 17–1).
UVEAL MELANOMA
Of the 2,111 eyes with uveal melanoma in the series from Shields et al,2 3% had secondary glaucoma: 7% of iris melanomas, 17% of ciliary body melanomas, and 2% of choroidal melanomas. Allaire et al35 and others have described ring melanomas, a rare variant of melanoma involving diffuse, circumferential neoplastic invasion of the iris, ciliary body, and angle. Glaucoma is most often associated with ring melanoma and this secondary glaucoma is a result of direct neoplastic invasion of the chamber angle or neovascularization. Diagnosis of a ring melanoma might be delayed because there is no visible mass on slit-lamp examination, and an intraocular mass may not be detected with B-scan ultrasonography. Heterochromia iridis, increased pigmentation of the trabecular meshwork, and glaucoma are the most frequently reported clinical findings associated with ring melanoma. Although pigmentary dispersion glaucoma and ring melanoma both exhibit increased pigmentation of the trabecular meshwork, pigmentary glaucoma is usually a bilateral process. Krukenberg spindles (pigment on the endothelium) and iris transillumination defects are not clinical signs in ring melanoma.36 Limbal extrascleral nodules may be the first presenting signs of ring melanoma. Ultrasound biomicroscopy may be an important ancillary tool to define this anterior segment tumor. The incidence of ring melanoma is unknown, and therefore the incidence of glaucoma is difficult to determine.35 Studies on the prevalence of glaucoma in uveal melanoma report variable statistics. Some reports are reviews of histologic enucleated specimens versus the incidence of intraocular tumors presenting to a glaucoma or oncology clinic. As Shields et al2 indicate, large melanomas with glaucoma are most likely enucleated by the primary ophthalmologist, and only tumors amenable to irradiation are referred to their institution for further treatment. Recent statistics may also be altered by the widespread use of indirect ophthalmoscopy leading to earlier diagnosis of smaller tumors.
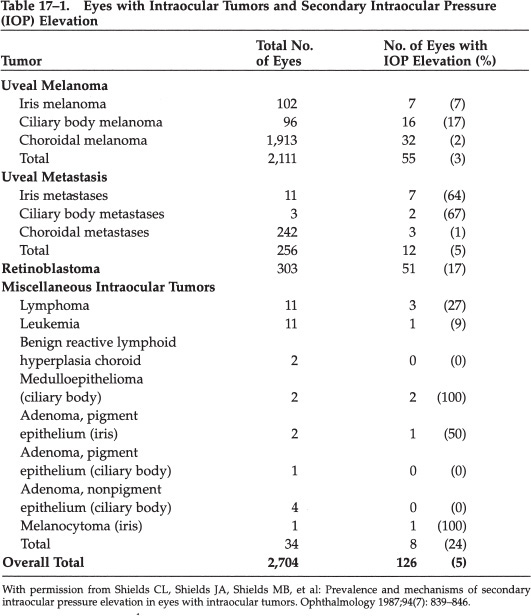
METASTASES
Metastases to the eye most commonly occur to the choroid centrally. In Shields et al’s2 series of 256 eyes manifesting uveal metastases, only 5% developed glaucoma. The majority of these uveal metastases associated with glaucoma involved the iris and ciliary body. Metastases to the iris and ciliary body were less frequent in occurrence but were increasingly associated with glaucoma in 64% and 67% of cases, respectively. In 242 cases of choroidal metastases, only 1% had elevated IOP greater than 23 mm Hg. Iris and ciliary body melanoma have elevated IOP secondary to direct tumor invasion of the angle; choroidal melanoma has elevated IOP resulting in angle closure from choroidal or retinal detachment.2
LYMPHOMA/LEUKEMIA
Sporadic case reports associate glaucoma with intraocular lymphoma, leukemia, metastatic melanoma, multiple myeloma, histiocytosis X, and myelodysplastic syndrome. In Shields et al’s2 survey, which consisted of 2,704 eyes with intraocular tumors, there were 11 eyes with lymphoma and leukemia each. Glaucoma was associated in 27% and 9% of the eyes with lymphoma and leukemia, respectively.
RETINOBLASTOMA
Reports of glaucoma associated with retinoblastoma vary from 2 to 23%.37,38 In Shields et al’s2 12-year study including 303 eyes with retinoblastoma, 17% developed glaucoma. Elevated IOP usually developed in advanced tumors occupying most of the vitreous cavity.
MEDULLOEPITHELIOMA
Broughton and Zimmerman18 described 56 cases of medulloepithelioma of which 46% were associated with glaucoma. Shields et al’s2 included two medulloepitheliomas among 2,704 intraocular tumors; both cases had elevated IOP.
MELANOCYTOMA
The incidence of melanocytoma complicated by glaucoma is unknown; there are case reports of iris melanocytoma and an even rarer association of optic nerve melanocytoma and glaucoma.8,22
NEUROFIBROMATOSIS
Neurofibromatosis is the most common phakomatosis and its frequency in the general population is approximately one in 3,500.39 Neurofibromatosis type I is more common, and its ophthalmic findings include Lisch nodules, plexiform neurofibromas of the eyelids, diffuse choroidal thickening, prominent corneal nerves, multifocal choroidal nevi, optic nerve gliomas, meningioma, and retinal astrocytic hamartoma. Sachsalber40 described the association of neurofibromatosis and glaucoma as early as 1897.
Congenital glaucoma may be present in patients with neurofibromatosis particularly with plexiform involvement of the eyelid.16 Neurofibromatosis may be associated with partial gigantism or segmentary hypertrophy, especially facial hemihypertrophy. The triad of unilateral buphthalmos, homolateral facial hemihypertrophy, and homolateral plexiform neuroma of the eyelid is known as François syndrome.17 This is the most common presentation of buphthalmos in neurofibromatosis.
NEVUS OF OTA
Case reports of glaucoma associated with nevus of Ota are found in the literature.20 The incidence may be as high as 10% of involved eyes.41
JUVENILE XANTHOGRANULOMA
Sporadic cases of juvenile xanthogranuloma of the iris, associated with glaucoma, are found in the literature.10 Diagnosis of juvenile xanthogranuloma is bimodal in nature: peak incidence occurs before 1 year of age and between 20 and 30 years. There is a male/female ratio of 4:1.42
Diagnosis and Differential Diagnosis
What Is the Differential Diagnosis and Distinguishing Features of Unilateral Glaucoma Not Associated with Intraocular Tumors?
Friedman1 characterized unilateral glaucoma by mechanism as open- and closed-angle forms. In the open-angle type, outflow was impaired either by accumulated material in the angle or from compromised angle structures. With hyphema, obstruction of the angle occurs by macrophages that have engulfed hemosiderin. Similarly, in uveitis inflammatory cells block the angle. Fuchs’ heterochromic iridocyclitis is typified by cataract, low-grade iridocyclitis, heterochromia, fine neovascularization of the angle, and glaucoma in a white, quiet-appearing eye. Phacolytic glaucoma characteristically occurs with a hypermature lens and is possibly associated with trauma; macrophages laden with lens material are seen as iritis or hypopyon. Pseudoexfoliation is an autosomal dominant disorder with incomplete penetrance and variable expressivity affecting patients 60 to 80 years of age. With gonioscopy, exfoliated debris can be seen on the iris surface and in the angle; iris transillumination defects and “hoarfrost” on the lens can be visualized. Pseudoexfoliation is unilateral 50% of the time and is associated with glaucoma in 70% of patients (Table 17–2).
Friedman1 further subdivided unilateral open-angle glaucoma into a subgroup with defective outflow channels. Hemosiderosis bulbi resulting from intraocular hemorrhage or siderosis bulbi resulting from retained iron containing intraocular foreign body may lead to heterochromia, glaucoma, and visual loss from retinal toxicity. Trauma may produce unilateral glaucoma by direct injury to the angle or angle recession (Table 17–3).
Hyphema Uveitis Iridocyclitis (e.g., Fuchs’ heterochromic) Glaucomatocyclitic crisis Phacolytic glaucoma Following lens rupture Hemolytic glaucoma Pigmentary glaucoma Malignant glaucoma Pseudoexfoliation |
With permission from Friedman AH: Clinicopathological correlations in unilateral glaucoma. Bull NY Acad Med 1979;55(3): 338–345. |
Hemosiderosis (or siderosis) bulbi Trauma Direct effect Postcontusion angle deformity With endothelialization Chymotrypsin induced Steroid induced Postinflammatory Associated with extraocular disease (e.g., cavernous sinus thrombosis) |
With permission from Friedman AH: Clinicopathological correlations in unilateral glaucoma. Bull NY Acad Med 1979;55(3): 338–345. |
Unilateral angle-closure glaucoma occurs in association with peripheral anterior synechiae (PAS). Rubeosis iridis, causing the formation of fibrous tissue in the angle, can result from underlying nonocular vascular diseases (carotid disease, aortic arch syndrome, giant cell arteritis, or carotid/cavernous fistula), inflammatory diseases (after endophthalmitis, irradiation, or uveitis), or primary retinal diseases (Coats’ disease, persistent hyperplastic primary vitreous, Norrie’s disease, retinopathy of prematurity, Leber’s disease, diabetes mellitus, or retinal detachment). With down-growth syndromes, epithelialization of the anterior chamber occurs following injury or surgery. When epithelial down-growth occurs, a thin, gray membrane may proliferate on the posterior corneal surface, within the anterior chamber angle and on the anterior iris surface. Additional sources of unilateral glaucoma are serous cysts of the iris, pearl growths, and endothelial cell growth (Table 17–4).
With rubeosis iridis Without rubeosis iridis Chronic angle-closure glaucoma Lens induced Swollen lens Dislocated lens Flat chamber Essential iris atrophy Chandler’s syndrome Iris nevus syndrome Epithelial invasion of the anterior chamber Endothelialization of the anterior chamber |
With permission from Friedman AH: Clinicopathological correlations in unilateral glaucoma. Bull NY Acad Med 1979;55(3): 338–345. |
What Are the Presenting Signs and Symptoms?
Iris melanomas are usually slow-growing, well-defined lesions that may be pigmented or amelanotic. The diffuse type of iris melanoma is associated with unilateral acquired heterochromia and ipsilateral glaucoma. Thickening of the iris stroma with angle invasion may be seen gonioscopically. Spontaneous hyphema may also occur.3
Necrotic iris melanocytoma also causes secondary glaucoma and heterochromia. Differentiation of iris melanocytoma from iris melanoma may be difficult clinically and require histologic confirmation.7
Ciliary body melanomas appear as brown masses in the ciliary body. These tumors may grow circumferentially extending around the ciliary body (ring melanoma). Ciliary body melanomas may present with either angle-closure, open-angle, or neovascular glaucoma.
Choroidal melanoma is a variably pigmented mass that may be mushroom-shaped and associated with retinal detachment. Angle closure may develop as the tumor enlarges; alternatively, rubeosis iridis and neovascular glaucoma may ensue.
Most commonly ocular metastases occur to the posterior pole as creamy-colored lesions with an overlying (nonrhegmatogenous) serous retinal detachment. Intractable angle-closure glaucoma can develop with diffuse involvement of the posterior uvea. The anterior uvea is much less frequently involved with metastases, but has greater propensity to develop glaucoma either of the closed-or open-angle forms. These anterior metastatic lesions appear as single or multinodular fleshy masses on the iris. They are friable, frequently seeding tumor cells into the angle, creating inflammation or pseudohypopyon. Rubeosis iridis is often associated. Ocular metastases may be the initial presentation of the malignancy Shields et al31 report that 32% of patients have no history of a primary cancer when the diagnosis of iris metastasis was made. Frequent clinical findings in metastatic iris tumors include secondary glaucoma (38%), prominent epibulbar injection (40%), irregular pupil (60%), hyphema (15%), pseudohypopyon (10%), and choroidal metastasis (35%). The size of metastatic iris tumors ranged from 1 × 1 × 0.5 mm to 12 × 6 × 3 mm. The most common primary sites are breast and lung followed by gastrointestinal tract, kidney, thyroid, and skin.29,31,43,44
Retinoblastoma may present as leukocoria, strabismus, or glaucoma. The differential diagnosis of retinoblastoma is listed in Table 17–5. Classically, retinoblastoma occurs in infants or very young children. However, it may also occur in older children and adults. In one review of 400 consecutive cases of retinoblastoma, 8.5% of the patients were 5 years or older at the time of diagnosis.45 Clinically, retinoblastoma may initially present as acute orbital cellulitis. Although the presence of intraocular calcium is suggestive of retinoblastoma, the absence of calcium does not exclude this tumor. Diffuse infiltrating retinoblastomas may not exhibit calcification or distinct mass.46,47 Both endo- and exophytic growth patterns may be associated with glaucoma that is usually seen only in the advanced stages of the tumor. Both angle-closure and neovascular glaucoma may develop.48,49
Medulloepithelioma of the iris or ciliary body appears as a solid or cystic grayish mass that is frequently associated with PAS and a shallow anterior chamber. Leukocoria or hyphema may also be observed. Glaucoma occurs from direct infiltration of the angle structures or rubeosis iridis. These tumors are seen at an older age than retinoblastoma and are typically not associated with calcification.6,18
Hereditary conditions
Developmental abnormalities
Inflammatory disorders
Tumors
Miscellaneous
|
With permission from Shields JA, Shields CL, Parsons HM: Review. Differential diagnosis of retinoblastoma. Retina 1991;11:232–243. |
What Are the Mechanisms for the Development of Secondary Glaucoma with Intraocular Tumors?
As with all glaucoma, either open- or closed-angle types can develop. Early studies published by Marshall32 in 1896 described angle closure in large choroidal tumors causing compression of the iris root into the angle and compromise of the angle structures by forward displacement of the lens/iris diaphragm. Other authors confirmed this mechanism of angle closure in ciliary body melanoma.50 Friedman1 noted PAS most frequently secondary to rubeosis iridis, as an invariable association to angle-closure glaucoma. Neoplastic sources of rubeosis iridis were uveal melanoma, retinoblastoma, and metastatic cancer. Yanoff34 studied the histopathology of 19 eyes with melanoma and associated glaucoma. In the group with angle closure, PAS was a consistent finding, whereas iris bombé, posterior synchiae, rubeosis iridis, and diffuse iris melanoma were variably present. In the group with open-angle glaucoma, aqueous drainage was obstructed. This occurred from seeding of tumor cells into the anterior chamber, by invasion of angle structures (as in ring melanomas), or by melanin-laden macrophages blocking the angle (melanomalytic glaucoma). Shields and Proia51 described neovascular glaucoma occurring with isolated rubeosis iridis in iris melanoma without direct tumor involvement of the angle. A secondary glaucoma associated with spontaneous hyphema may also occur (Fig. 17–1).
IRIS MELANOMA
Iris melanoma most frequently directly invades the trabecular meshwork, but tumor seeding, melanin granules, or macrophage laden with melanin may obstruct the angle; secondary glaucoma from hyphema or rubeosis iridis has also been reported.33,35 A case report of iris ring melanoma associated with unilateral glaucoma and mistaken for unilateral pigmentary glaucoma cautions one in diagnosing atypical but increased angle pigmentation.36
CILIARY BODY MELANOMA
Ciliary body melanoma may cause angle-closure glaucoma by compressing the iris root into the angle or by forward displacement of the lens-iris diaphragm by the expanding mass creating a pupillary block.52 Iris bombé subsequently develops followed by formation of PAS and a secondary angle closure. PAS and angle closure may also develop as a result of rubeosis iridis. Alternatively, invasion of the angle by tumor or seeding of neoplastic cells or melanin granules from necrotic tumors may lead to mechanical obstruction of the trabeculum and open-angle glaucoma.2
CHOROIDAL MELANOMA
Choroidal melanoma is associated with glaucoma by iris and angle neovascularization, tumor necrosis-induced inflammation, pigment dispersion, or anterior displacement of the lens-iris diaphragm. This is a mass effect of the tumors with or without a retinal detachment or swelling of the lens.2,53
IRIS AND CILIARY BODY METASTASES
Metastatic tumors to the iris and/or ciliary body produce glaucoma by invading the angle structures or by covering them with sheets of tumor cells. Other mechanisms include pigmentary dispersion and hemolytic, uveitic, and neovascular forms of glaucoma.
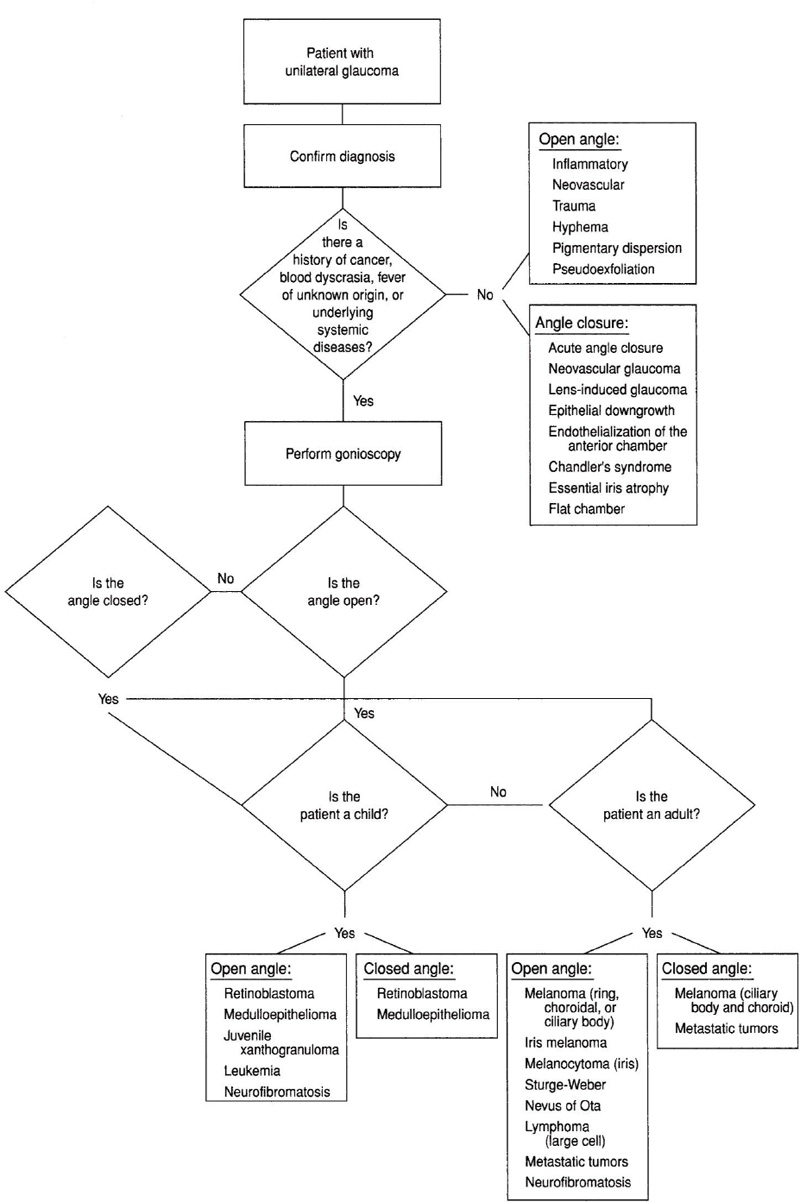
Figure 17–1. Differential diagnosis of a patient with glaucoma associated with intraocular tumors
CHOROIDAL METASTASES
In contrast, choroidal metastases affect IOP only with large mass size that is associated with choroidal or total retinal detachment. Subsequently, angle closure develops from displacement of the lens-iris diaphragm.2,44 The formation of PAS may also lead to angle closure.54
LEUKEMIA
Glaucoma may occur in leukemia by direct infiltration of angle structures, or be associated with hypopyon or hyphema.55 Massive subretinal or choroidal hemorrhage has reportedly been associated with cases of angle closure.2,4,56–58
LYMPHOMA
Intraocular lymphoma may directly infiltrate the uveal tract or be associated with a nongranulomatous uveitis causing a secondary IOP elevation.59
RETINOBLASTOMA
Many studies of retinoblastoma confirm that iris neovascularization is the most frequent cause of glaucoma.2 Angle closure from anterior displacement of the lens-iris diaphragm secondary to massive, exudative retinal detachment may occur. Less frequently, there is tumor seeding or shedding of necrotic tumor cells into the anterior chamber, uveitis, or hyphema.13,38
MEDULLOEPITHELIOMA
Histopathologic specimens of medulloepithelioma associated with glaucoma confirm the presence of rubeosis iridis, PAS, and shallow anterior chamber.18 Narrow-angle glaucoma may also be produced by the large mass effect posteriorly causing forward displacement of the lens-iris diaphragm. Direct infiltration of the angle by tumor cells or hyphema may cause a form of open-angle glaucoma.6,18
IRIS MELANOCYTOMA
Iris melanocytoma may be associated with glaucoma. Shedding of tumor cells or necrosis of the tumor with pigment dispersion into the anterior chamber compromises the trabecular meshwork.7,23,60 Rare reports of optic disc melanocytoma describe glaucoma resulting from the massive tumor size causing forward displacement of the lens-iris diaphragm and angle closure.22
JUVENILE XANTHOGRANULOMA
This tumor may be associated with either a vascular iris or ciliary body mass that produces glaucoma due to its hemorrhagic or inflammatory propensity. Open-angle glaucoma occurs from hyphema, uveitis, or even histiocytic invasion of the angle.18,61
STURGE-WEBER
This syndrome is characterized by cutaneous facial nevus flammeus in the trigeminal nerve distribution, ipsilateral diffuse cavernous hemangioma of the choroid, and ipsilateral meningeal racemose hemangioma. The choroidal hemangioma associated with Sturge-Weber is not the direct cause of the frequently associated glaucoma. The etiology of the glaucoma is equivocal and may be multifactoral. Possible mechanisms include vascular or mechanical etiologies. It has been possibly attributed to anomalous development of the angle, neovascularization of the trabecular meshwork, or small arteriovenous fistulas in the episcleral vessels causing elevated venous pressure.62–66 Histologic evidence reveals a poorly developed scleral spur and thickened uveal meshwork; the iris root is anteriorly inserted on the trabecular meshwork base.62 In addition, incomplete and posterior displacement of the Schlemm’s canal has been reported.63 It is hypothesized that the etiology of elevated IOP in Sturge-Weber is a result of combined developmental angle anomalies and elevated episcleral venous pressure mechanisms; ultimately, these mechanisms yield ultrastructural and functional changes in the trabecular meshwork.67
NEUROFIBROMATOSIS
In neurofibromatosis, glaucoma may occur by a variety of postulated mechanisms: (1) neurofibromas may infiltrate the angle, (2) increased secretion of the ciliary body may occur from paralysis of the ciliary nerves, (3) nodular thickening of the ciliary body and choroid may close the angle, (4) rubeotic-like tissue in the angle may create PAS, and (5) an anomalous angle may develop with aplastic or incompletely formed Schlemm’s canal. Buphthalmos may occur with normal IOP as a form of regional gigantism.17,68,69
NEVUS OF OTA
The ipsilateral open-angle glaucoma associated with oculodermal melanocytosis (nevus of Ota) may be secondary to tumor (melanoma of the iris, ciliary body, or choroid), inflammation, or melanocytic infiltration of the aqueous outflow channels.9,20
What Is Melanomalytíc Glaucoma?
Melanin from a necrotic melanoma is engulfed by macrophages that obstruct the trabecular meshwork. Additionally, melanin may be phagocytosed by trabecular endothelial cells.34,70,71
What Is the Differential Diagnosis of Heterochromia Associated with Unilateral Glaucoma and Intraocular Tumor?
Nevus of Ota, retinoblastoma, iris melanoma, iris metastases, ring melanoma, and iris medulloepithelioma present with heterochromia and unilateral glaucoma. Nevus of Ota is congenital in nature. Retinoblastoma and iris medulloepithelioma are commonly diagnosed in the first decade of life. In contrast, iris melanoma, ring melanoma, and iris metastases occur in adults.
What Factors Influence the Likelihood of Glaucoma Developing in Melanoma?
Yanoff52 reported on 19 eyes with melanoma and associated glaucoma. He concluded that the size and location of the tumor, the nature of the lesion, and associated retinal detachment were the risk factors for developing glaucoma. Increased prevalence of glaucoma occurred with anterior melanomas involving only the iris, combined iris, and ciliary body, or with large posterior tumors accompanied by total retinal detachment. In Shields and Klintworth’s33 review of 11 consecutive anterior uveal melanomas, there was a correlation between elevated IOP and tumor involvement of the iris and angle. Tumor necrosis with dispersion of melanin and/or melanin-laden macrophages predisposes to melanomalytic glaucoma. Furthermore, the presence of rubeosis iridis or PAS increases the risk of glaucoma. The importance of melanoma type is demonstrated by the consistent association of glaucoma in ring melanoma35 (Table 17–6).
What Diagnostic Modalities Are Important in the Evaluation and Examination of Glaucoma Secondary to Underlying Intraocular Tumor?
A thorough history, including breast masses, skin lesions, cough, lung tumor, gastrointestinal problems, changes in weight, and fever of unknown origin, is important to elicit. Previous surgeries, underlying systemic diseases or vascular problems, blood dyscrasias, tuberculosis, evidence of malignancy, and previous chemotherapy or other cancer treatment should be noted in the medical record. Previous ocular surgeries or problems must also be recorded.
To perform a full clinical examination in children, anesthesia may be necessary. The importance of the clinical exam is emphasized by Yanoff,52 who reports that melanorna of the iris associated with glaucoma usually can be diagnosed by clinical exam. Additionally, he cautions that an eye with opaque media and glaucoma not responding to conventional therapy must be suspect for undiagnosed melanoma. The ocular examination should include IOP measurements, biomicroscopy, gonioscopy, and dilated fundus exam. The exclusion of tumor associated with glaucoma or the risk of glaucoma with a known intraocular tumor needs to be assessed. All eyes with rubeosis iridis should undergo gonioscopy to exclude a mass lesion in the angle. The angle should be studied for patterns of pigmentation, configuration, depth, and evidence of previous inflammation such as PAS. The iris surface should be examined for rubeosis iridis, heterochromia, ectropion uveae, and mass lesions. Translucent, gelatinous nodules are typical of metastases; the hallmark of neurofibromatosis is the variably colored dome-shaped stromal iris elevations known as Lisch nodules. Variably pigmented iris lesions are present in melanoma and melanocytoma.
Open Angle
|
Angle Closure
|
With permission from Friedman AH: Clinicopathological correlations in unilateral glaucoma. Bull NY Acad Med 1979;55(3): 338–345. |
Stereo slit-lamp and fundus photographs are important for documentation and growth observation. B-scan ultrasound may aid in defining the solid or cystic nature of a lesion, the nodularity or dimensions, and the characteristic reflectivity. This technique may be used to exclude possible extension of an anterior chamber mass from the ciliary body. High-resolution (50 MHz) ultrasound biomicroscopy (UBM) has been used in eyes with impaired visualization of the anterior segment. Lanzl et al72 described the use of this technique in an eye with metastatic cancer, hypopyon, and elevated IOP. Excisional biopsy of an iris mass, by peripheral or sector iridectomy, with frozen sections may assist in the differentiation of iris nevus versus melanoma. Confirmation of melanin granules (from necrotic tumor) or tumor seeding into the anterior chamber can be obtained by aqueous aspiration and Papanicolaou stain. Two limbal nodules of extrascleral extension from a ring melanoma were biopsied by Allaire et al35 to confirm the diagnosis prior to enucleation. Fine-needle aspiration biopsy of iris ring melanoma was employed by Chaudhry et al36 and by others of ciliary body and choroidal melanoma for cytologic diagnosis. Additional tests to be considered are fluorescein angiography, computed tomography (CT), magnetic resonance imaging (MRI),53 and transillumination. The 32P test has been used as a diagnostic adjuvant in the differentiation of benign from malignant choroidal lesions. This test is based on the principle that malignant tumor cells incorporate and use phosphorus to a greater degree than do normal tissues.73 However, the 32P test is not frequently employed because other methods such as ultrasonography, fluorescein angiography, ophthalmoscopy, and fine-needle aspiration biopsy are more accurate. Various authors have encouraged a thorough evaluation of intraocular masses especially those associated with glaucoma and opaque media. Unnecessary surgery, risking tumor dissemination, should be avoided.53,73,74
RETINOBLASTOMA
The diagnosis of retinoblastoma is largely dependent on the clinical exam. Ultrasound, CT scan, MRI, and fluorescein angiography may be employed. Recently there has been little use of invasive techniques such as aqueous aspirates assessing lactic acid dehydrogenase levels to diagnose retinoblastoma. Vitrectomy and fine-needle aspirates are also contraindicated due to the risk of tumor dissemination.48
MALIGNANT LYMPHOMA AND LEUKEMIA
These tumors are largely diagnosed in the context of the systemic disease. Transocular fine-needle aspirate or vitreous biopsy with cytology may be helpful.
MEDULLOEPITHELIOMA
En bloc resection (by iridectomy or iridocyclectomy) will ultimately provide histologic diagnosis if the tumor is well localized. However, the clinician may utilize indirect ophthalmoscopy and slit-lamp biomicroscopy to facilitate the diagnosis. Most eyes with medulloepithelioma have been diagnosed and treated by enucleation with or without exenteration.6,18,75
MELANOCYTOMA
Melanocytoma of the iris may be investigated through the techniques of transillumination (to exclude a cystic structure), ultrasonography (demonstrating the solid tumor with low internal reflectivity), fluorescein angiography (blocked fluoresence), high-frequency ultrasound biomicroscopy, fine-needle biopsy, or excisional biopsy.8 Slit-lamp examination and gonioscopy are paramount; heterochromia and tumor necrosis may be present. Release of pigment from the necrotic melanocytoma stimulates an intense macrophagic response that infiltrates the trabecular meshwork. Although fine-needle aspiration biopsy may facilitate the diagnosis of intraocular tumors, Fineman et al7 caution that fine-needle biopsy may not diagnose an occult focus of melanoma, and a negative cytologic diagnosis for malignancy does not rule out an intraocular malignancy. Therefore, they recommend local resection of an iris tumor as preferable to biopsy.
JUVENILE XANTHOGRANULOMA
Biopsy of other skin lesions demonstrating foamy histiocytes may assist in the diagnosis of juvenile xanthogranuloma of the iris.
NEUROFIBROMATOSIS
Neurofibromatosis and François syndrome may be further diagnosed by CT and general physical examination looking for evidence of gigantism, café-au-lait spots, or neurofibromas. Lisch nodules of the iris are noted on slit-lamp examination more than 90% of the time.76,77 Fluorescein angiography may further delineate the chorioretinal hamartomas; visual field testing, color vision evaluation, and CT or MRI may be useful in evaluating optic nerve gliomas. Ultimately in the evaluation of all tumors, enucleation with histologic staining and scanning electronmicroscopy may be employed for definitive diagnosis (Fig. 17–1).
Treatment and Management
How Is Glaucoma Associated with Intraocular Tumors Treated?
IRIS MELANOMA
A newly diagnosed iris melanoma is often managed by observation, and the glaucoma is conservatively managed with medical therapy. Slit-lamp photography and gonioscopy are essential to document growth of the lesion. Laser trabeculoplasty to the uninvolved meshwork can be performed if more aggressive treatment is required.3 Shields and Proia51 describe regression of neovascular glaucoma after excision of an iris melanoma. A diffuse or large iris melanoma may require enucleation. Filtration surgery is contraindicated due to the risk of dissemination or extrascleral extension.
CILIARY BODY AND CHOROIDAL MELANOMA
Uveal melanomas associated with glaucoma are typically large, diffuse, and associated with a poor prognosis. Therefore, enucleation is usually the standard of care. Intraoperatively, care must be taken to avoid iatrogenic elevation in the IOP, thereby risking tumor dissemination.78–80 Several authors report that enucleation may decrease the patient’s prognosis for survival. Within the group of patients with uveal melanoma, peak mortality occurs 2 years after enucleation and is associated with a 12% mortality rate. In contrast, nonenucleated patients exhibited a mortality rate of 1% per year of life. Contrasting these two melanoma patients groups, the mortality rate of the enucleated group equals that of the nontreated group at 7 to 8 years. Fraunfelder et al81 have recommended the “no touch” technique during an enucleation to minimize the elevated IOP spike to 500 mm Hg, causing tumor cells to disseminate systemically and increasing the incidence of metastasis.81
Although glaucoma secondary to melanoma does not usually respond to medical treatment,52 a trial of glaucoma medications is warranted. In rare cases, local excision or irradiation techniques may be employed. Ophthalmic oncologists may best perform radioactive plaque therapy. Surgical treatment with filtering surgery is contraindicated due to the risk of dissemination, extrascleral extension, or even metastases.82 For intractable glaucoma that is medically uncontrollable, a cyclodestructive procedure or enucleation may be indicated for large melanomas. Kim et al83 utilized helium ion irradiation predominantly to treat mostly large uveal melanomas. Patients with large melanomas who received higher radiation doses tended to develop neovascular glaucoma in contrast to patients who received low irradiation doses.
The Collaborative Ocular Melanoma Study (COMS) is an ongoing international study to evaluate small, medium, and large melanomas. Large melanoma is a potential metastatic tumor associated with patient mortality; this randomized study will evaluate the mortality rate of patients treated with enucleation alone versus external beam radiation and subsequent enucleation.84 Prior to any surgical intervention, it is important to have the patient evaluated by a medical internist and to obtain some ancillary studies. These studies include a complete blood count, liver function studies, and chest x-ray. If the liver function studies are abnormal, CT, MRI, or fine-needle liver biopsy may be necessary to evaluate the presence of metastatic disease. Following treatment of an intraocular melanoma, the patient should be periodically evaluated systemically for potential metastatic disease.
METASTATIC CANCER AND LEUKEMIA
Treatment of metastatic cancer or leukemia with chemotherapy and possible local irradiation to the eye often results in resolution of the glaucoma. If the IOP remains elevated, the residual glaucoma can be treated medically, with cyclodestructive surgery or retrobulbar alcohol. Blind, painful eyes are enucleated. An incidental report describes washing necrotic tumor cells from the anterior chamber to treat glaucoma associated with leukemia.56 Semiconductor diode laser transscleral cyclophotocoagulation was described by El-Harazi et al.85 This case report described a patient with progressive infiltrative ductal carcinoma of the breast with metastasis to the brain, spine, liver, lung, and iris. This associated elevated IOP was refractory to maximal tolerated medications. The patient received contact transscleral semiconductor diode laser cyclophotocoagulation and subsequent external beam radiation; within 2 months the IOP was controlled, but the iris metastatic lesions did not resolve. In summary, diode laser has been used in refractory glaucoma but the risk of tumor dissemination is unknown.85
RETINOBLASTOMA
Glaucoma associated with retinoblastoma usually occurs in the context of a unilateral advanced and large tumor. Therefore, enucleation is performed when a long section of optic nerve is obtained for histologic examination for metastatic or direct extention. In the presence of bilateral retinoblastoma, episcleral plaque radiotherapy or external beam irradiation may be an alternative in selected cases. Because preservation of useful vision is imperative, consultation with an ophthalmic oncologist is prudent. A detailed family history and exam under anesthesia (EUA) with funduscopy is important prior to enucleation. A lumbar puncture, bone marrow aspirate, and bone marrow biopsy should be obtained during the EUA to exclude metastases via cerebrospinal fluid and hematogenous extention. Additional ancillary studies may include a bone scan to identify distant metastases and a CT to document the presence of intraocular calcium and pinealoblastoma. Genetic evaluation and counseling are important to determine if the form of retinoblastoma is of hereditary nature. Because retinoblastoma is associated with a deletion of the second allele of the long arm of chromosome 13 (13q14), tumor suppressor gene product is not produced and these individuals are susceptible to secondary tumors such as osteosarcoma, malignant melanoma, chondrosarcoma, rhabdomyosarcoma, glioma, neuroblastoma, squamous cell carcinoma, and sebaceous cell carcinoma.86–91
JUVENILE XANTHOGRANULOMA
This is a benign and often self-limiting disease that responds to topical, subconjunctival, and systemic steroids. Rarely, external beam irradiation is required. Trabeculectomy has not proven to be successful. Medical and not surgical treatment of the glaucoma should be attempted.92–94
MEDULLOEPITHELIOMA
Treatment of medulloepithelioma has not been standardized.6 These frequently blind and painful eyes undergo enucleation. Small, well-circumscribed tumors may be locally resected by cyclectomy, iridocyclectomy, or iridocyclotrabeculectomy.
MELANOCYTOMA
Melanocytoma treated with excisional biopsy may undergo normalization of the IOP.23 Shields et al23 described management of a case in this manner but caution that pigmented iris lesions associated with glaucoma may be difficult to differentiate from malignancy. Even benign tumors may undergo necrosis, and the decision to enucleate may be justifiable.
STURGE-WEBER
The glaucoma associated with Sturge-Weber syndrome may initially be managed medically but frequently requires more definitive surgery later. Filtering surgery is associated with increased frequency of complications such as choroidal effusion or even expulsive choroidal hemorrhage. Some authors recommend preplaced sclerostomies or combined trabeculectomy/trabeculotomy to reduce the chance for complications.95–97
NEUROFIBROMATOSIS
Neurofibromatosis associated glaucoma should be treated medically when possible, as the response to surgery is often poor.98
Future Considerations
Active research is being pursued in the treatment of retinoblastoma and choroidal melanoma in animal models and in limited human studies.
Murine models can be transgenically induced to produce retinoblastoma. Carney et al99 have suggested that frequent subconjunctival carboplatin may be effective. The total dose of this drug appears to be important in tumor control in the murine transgenic retinoblastoma model. These data may also have significant clinical implications for the treatment of childhood retinoblastoma. Furthermore, Cicciarelli et al100 studied the toxicity of subconjunctival injected carboplatin by monitoring the electroretinogram (ERG) and subsequent histologic changes in dwarf pigmented rabbits. This study suggests that subconjunctival carboplatin may be well tolerated in the treatment of retinoblastoma.
Stereotactic radiotherapy and radiosurgery may be beneficial in the treatment of uveal melanoma. Zehetmayer et al101 utilized stereotactic Linac-based radiotherapy (linear accelerator) to irradiate uveal melanoma. This treatment may play a role in the conservative management of uveal melanoma. Mueller et al102 studied the efficacy of stereotactic radiosurgery of uveal melanoma with the Leksell gamma knife. Although only 25 patients were included in this short-term study, results indicate that radiosurgery using the Leksell gamma knife was beneficial in medium-size and large choroidal body melanomas that otherwise would be enucleated. These studies did not specifically discuss the issue of glaucoma associated with retinoblastoma or melanoma. However, these future medical and surgical modalities may facilitate visual acuity preservation and control of elevated IOP.
References
9. Foulks G, Shields MB: Glaucoma in oculodermal melanocytosis. Ann Ophthalmol 1977;10:1299–1304.
10. Hadden OB: Bilateral juvenile xanthogranuloma of the iris. Br J Ophthalmol 1975;59:699–702.
25. Thomas CI, Purnell EW: Ocular melanocytoma. Am J Ophthalmol 1969;67:79–86.
26. Arentsen JJ, Green WR: Melanoma of the iris. Report of 72 cases treated surgically. Ophthalmic Surg 1975;6:23–37.
34. Yanoff M: Glaucoma mechanisms in ocular malignant melanomas. Am J Ophthalmol 1970;70:898–904.
39. Riccardi VM: Neurofibromatosis: past, present, and future. N Engl J Med. 1991;324:283–285.
45. Shields CL, Shields JA, Shah P: Retinoblastoma in older children. Ophthalmology 1991;98:395–399.
47. Bhatnagar R, Vine AK: Diffuse infiltrating retinoblastoma. Ophthalmology 1991;98:1657–1661.
55. Rosenthal AR: Ocular manifestations of leukemia, a review. Ophthalmology 1983;90:899–905.
60. Nakazawa M, Tamai M: Iris melanocytoma with secondary glaucoma. Am J Ophthalmol 1984;97:797–799.
66. Phelps CD: The pathogenesis of glaucoma in Sturge-Weber syndrome. Ophthalmology 1978;85:276–286.
92. Gass JDM: Management of juvenile xanthogranuloma of the iris. Arch Ophthalmol 1964;71:344–347.
93. Cadera W, Silver MM, Burt L: Juvenile xanthogranuloma. Can J Ophthalmol 1983;18:169–174.
98. Brownstein S, Little JM: Ocular neurofibromatosis. Ophthalmology 1983;90:1595–1599.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


