Glaucoma
9.1 PRIMARY OPEN-ANGLE GLAUCOMA
Symptoms
Usually asymptomatic until the later stages. Early symptoms may include parts of a page missing. Tunnel vision and loss of central fixation typically do not occur until late in the disease.
Signs
 Intraocular pressure (IOP): Although most patients will have an elevated IOP (normal range of 10 to 21 mm Hg), nearly half have an IOP of 21 mm Hg or lower at any one screening.
Intraocular pressure (IOP): Although most patients will have an elevated IOP (normal range of 10 to 21 mm Hg), nearly half have an IOP of 21 mm Hg or lower at any one screening.
 Gonioscopy: Normal-appearing, open anterior chamber angle on gonioscopic evaluation. No peripheral anterior synechiae (PAS).
Gonioscopy: Normal-appearing, open anterior chamber angle on gonioscopic evaluation. No peripheral anterior synechiae (PAS).
 Optic nerve: See Figure 9.1.1. Characteristic appearance includes loss of rim tissue (includes notching; increased narrowing superiorly, inferiorly, or nasally more than temporally; progressive narrowing over time), regional pallor, splinter or nerve fiber layer hemorrhage that crosses the disc margin (Drance hemorrhage), acquired pit, nerve fiber layer defect, cup/disc (C/D) asymmetry >0.2 in the absence of a cause (e.g., anisometropia, different nerve sizes), bayoneting (sharp angulation of the blood vessels as they exit the nerve), enlarged C/D ratio (>0.6; less specific), progressive enlargement of the cup, greater Disc Damage Likelihood Scale (DDLS) score (see Figure 9.1.2).
Optic nerve: See Figure 9.1.1. Characteristic appearance includes loss of rim tissue (includes notching; increased narrowing superiorly, inferiorly, or nasally more than temporally; progressive narrowing over time), regional pallor, splinter or nerve fiber layer hemorrhage that crosses the disc margin (Drance hemorrhage), acquired pit, nerve fiber layer defect, cup/disc (C/D) asymmetry >0.2 in the absence of a cause (e.g., anisometropia, different nerve sizes), bayoneting (sharp angulation of the blood vessels as they exit the nerve), enlarged C/D ratio (>0.6; less specific), progressive enlargement of the cup, greater Disc Damage Likelihood Scale (DDLS) score (see Figure 9.1.2).
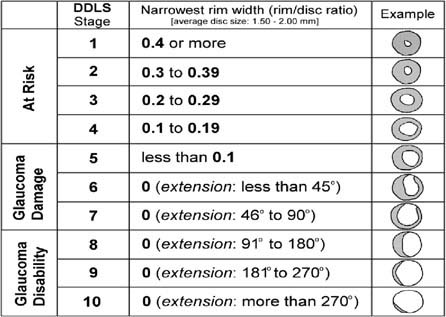
FIGURE 9.1.2. Disc Damage Likelihood Damage Scale.
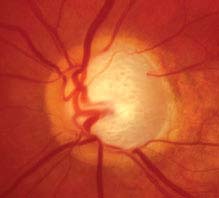
FIGURE 9.1.1. Primary open-angle glaucoma with advanced optic nerve cupping.
 Visual fields: Characteristic visual field loss includes nasal step, paracentral scotoma, arcuate scotoma extending from the blind spot nasally (defects usually respect the horizontal midline or are greater in one hemifield than the other), altitudinal defect, or generalized depression (see Figure 9.1.3).
Visual fields: Characteristic visual field loss includes nasal step, paracentral scotoma, arcuate scotoma extending from the blind spot nasally (defects usually respect the horizontal midline or are greater in one hemifield than the other), altitudinal defect, or generalized depression (see Figure 9.1.3).
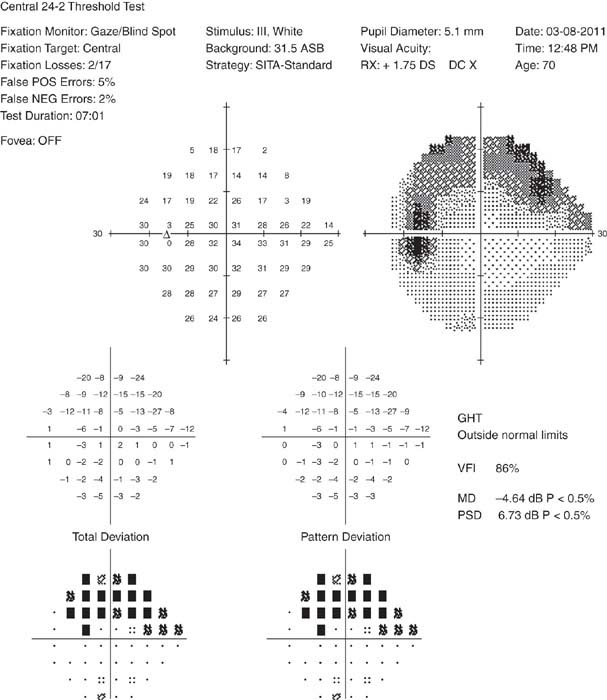
FIGURE 9.1.3. HVF showing a supero-nasal arcuate scotoma.
Other. Large fluctuations in IOP, absence of microcystic corneal edema, an uninflamed eye.
Differential Diagnosis
If Anterior Chamber Angle Open on Gonioscopy:
 Ocular hypertension: Normal optic nerve and visual field. See 9.3, Ocular Hypertension.
Ocular hypertension: Normal optic nerve and visual field. See 9.3, Ocular Hypertension.
 Physiologic optic nerve cupping: Static enlarged C/D ratio without rim notching or visual field loss. Usually normal IOP and large optic nerve (> about 2 mm). Often familial.
Physiologic optic nerve cupping: Static enlarged C/D ratio without rim notching or visual field loss. Usually normal IOP and large optic nerve (> about 2 mm). Often familial.
 Secondary open-angle glaucoma: Identifiable cause for open-angle glaucoma including lens-induced, inflammatory, exfoliative, pigmentary, steroid-induced, angle recession, traumatic (as a result of direct injury, blood, or debris), and glaucoma related to increased episcleral venous pressure (e.g., Sturge–Weber syndrome, carotid–cavernous fistula), intraocular tumors, degenerated red blood cells (ghost cell glaucoma), degenerated photoreceptor outer segments following chronic rhegmatogenous retinal detachment (Schwartz–Matsuo syndrome), or developmental anterior segment abnormalities. See specific sections.
Secondary open-angle glaucoma: Identifiable cause for open-angle glaucoma including lens-induced, inflammatory, exfoliative, pigmentary, steroid-induced, angle recession, traumatic (as a result of direct injury, blood, or debris), and glaucoma related to increased episcleral venous pressure (e.g., Sturge–Weber syndrome, carotid–cavernous fistula), intraocular tumors, degenerated red blood cells (ghost cell glaucoma), degenerated photoreceptor outer segments following chronic rhegmatogenous retinal detachment (Schwartz–Matsuo syndrome), or developmental anterior segment abnormalities. See specific sections.
 Low-pressure glaucoma: Same as primary open-angle glaucoma (POAG) except normal IOP. See 9.2, Low-Pressure Primary Open-Angle Glaucoma (Normal Pressure Glaucoma).
Low-pressure glaucoma: Same as primary open-angle glaucoma (POAG) except normal IOP. See 9.2, Low-Pressure Primary Open-Angle Glaucoma (Normal Pressure Glaucoma).
 Previous glaucomatous damage (e.g., from steroids, uveitis, glaucomatocyclitic crisis, trauma) in which the inciting agent has been removed. Nerve appearance now static.
Previous glaucomatous damage (e.g., from steroids, uveitis, glaucomatocyclitic crisis, trauma) in which the inciting agent has been removed. Nerve appearance now static.
 Optic atrophy: Characterized by disproportionally more optic nerve pallor than cupping. IOP usually normal unless a secondary or unrelated glaucoma is present. Color vision and central vision are often decreased. Causes include optic nerve, chiasmal, or tract tumors, syphilis, ischemic optic neuropathy, drugs, retinal vascular or degenerative disease, others. Visual field defects that respect the vertical midline are typical of intracranial lesions at or posterior to the chiasm.
Optic atrophy: Characterized by disproportionally more optic nerve pallor than cupping. IOP usually normal unless a secondary or unrelated glaucoma is present. Color vision and central vision are often decreased. Causes include optic nerve, chiasmal, or tract tumors, syphilis, ischemic optic neuropathy, drugs, retinal vascular or degenerative disease, others. Visual field defects that respect the vertical midline are typical of intracranial lesions at or posterior to the chiasm.
 Congenital optic nerve defects (e.g., tilted discs, colobomas, optic nerve pits): Visual field defects may be present but are static.
Congenital optic nerve defects (e.g., tilted discs, colobomas, optic nerve pits): Visual field defects may be present but are static.
 Optic nerve drusen: Optic nerves not usually cupped and drusen often visible. Visual field defects may remain stable or progress unrelated to IOP. The most frequent defects include arcuate defects or an enlarged blind spot. Characteristic calcified lesions can be seen on B-scan ultrasonography (US) and on computed tomography (CT).
Optic nerve drusen: Optic nerves not usually cupped and drusen often visible. Visual field defects may remain stable or progress unrelated to IOP. The most frequent defects include arcuate defects or an enlarged blind spot. Characteristic calcified lesions can be seen on B-scan ultrasonography (US) and on computed tomography (CT).
If Closed or Partially Closed Angle on Gonioscopy:
 Chronic angle-closure glaucoma (CACG): Shallow anterior chamber, blurred vision, headache. PAS present on gonioscopy. See 9.5, Chronic Angle-Closure Glaucoma.
Chronic angle-closure glaucoma (CACG): Shallow anterior chamber, blurred vision, headache. PAS present on gonioscopy. See 9.5, Chronic Angle-Closure Glaucoma.
Work-Up
1. History: Presence of risk factors (family history of blindness or visual loss from glaucoma, older age, African descent, diabetes, myopia, hypertension or hypotension)? Previous history of increased IOP or chronic steroid use? Refractive surgery including laser in situ keratomileusis (LASIK) in past (change in pachymetry)? Review of past medical history to determine appropriate therapy including asthma, chronic obstructive pulmonary disease (COPD), congestive heart failure, heart block or bradyarrythmia, renal stones, allergies?
2. Baseline glaucoma evaluation: All patients with suspected glaucoma of any type should have the following:
—Complete ocular examination including visual acuity, pupillary assessment for a relative afferent pupillary defect, confrontational visual fields using a red object (e.g., red top of a mydriatic drop), slit-lamp examination, applanation tonometry, gonioscopy, and dilated fundus examination (if the angle is open) with special attention to the optic nerve.
—Baseline documentation of the optic nerves (e.g., stereoscopic disc photos, red-free photographs, computerized image analysis [e.g., optical coherence tomography (OCT) or Heidelberg retina tomography (HRT)], or meticulous drawings) and formal visual field testing (preferably automated, e.g., Humphrey). Goldmann visual field tests may be helpful in patients unable to take the automated tests adequately. Color vision testing indicated in those suspected of a neurologic disorder (see Figure 9.1.4).
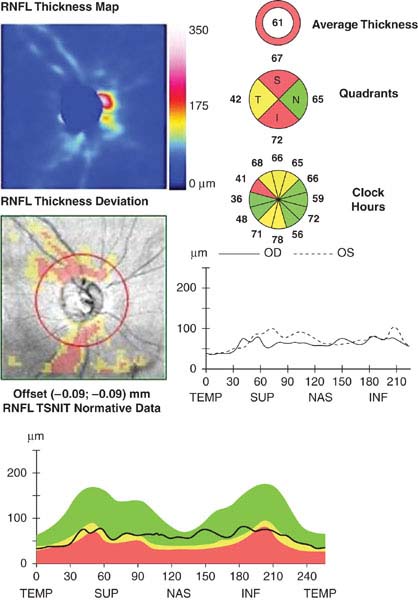
FIGURE 9.1.4. Optical coherence tomography of retinal nerve fiber layer thickness.
—Measure central corneal thickness (CCT). Corneal thickness variations affect apparent IOP as measured with applanation tonometry. Average corneal thickness is 530 to 545 microns. Thinner corneas tend to underestimate IOP, whereas thicker corneas tend to overestimate IOP, although the relationship between corneal thickness and measured IOP is not exactly linear. A thin CCT is an independent risk factor for the development of POAG.
—Further evaluation for other causes of optic nerve damage should be considered when any of the following atypical features are present:
 Optic nerve pallor out of proportion to the degree of cupping.
Optic nerve pallor out of proportion to the degree of cupping.
 Visual field defects greater than expected based on amount of cupping.
Visual field defects greater than expected based on amount of cupping.
 Visual field patterns not typical of glaucoma (e.g., defects respecting the vertical midline, hemianopic defects, enlarged blind spot, central scotoma).
Visual field patterns not typical of glaucoma (e.g., defects respecting the vertical midline, hemianopic defects, enlarged blind spot, central scotoma).
 IOP within the average range (<21 mm Hg) or symmetric between both eyes.
IOP within the average range (<21 mm Hg) or symmetric between both eyes.
 Unilateral progression despite equal IOP in both eyes.
Unilateral progression despite equal IOP in both eyes.
 Decreased visual acuity out of proportion to the amount of cupping or field loss.
Decreased visual acuity out of proportion to the amount of cupping or field loss.
 Color vision loss, especially in the red–green axis.
Color vision loss, especially in the red–green axis.
If any of these are present, further evaluation may include:
 History: Acute episodes of eye pain or redness? Steroid use? Acute visual loss? Ocular trauma? Surgery, systemic trauma, heart attack, dialysis, or other event that may lead to hypotension?
History: Acute episodes of eye pain or redness? Steroid use? Acute visual loss? Ocular trauma? Surgery, systemic trauma, heart attack, dialysis, or other event that may lead to hypotension?
 Diurnal IOP curve consisting of multiple IOP checks during the course of the day.
Diurnal IOP curve consisting of multiple IOP checks during the course of the day.
 Consider other laboratory work-up for nonglaucomatous optic neuropathy: heavy metals, angiotensin-converting enzyme, vitamin B12/folate, rapid plasma reagin, fluorescent treponemal antibody absorption, Lyme titer, antinuclear antibody. If giant cell arteritis (GCA) is a consideration, then check erythrocyte sedimentation rate, C-reactive protein, and complete blood count (CBC) with platelets [see 10.17, Arteritic Ischemic Optic Neuropathy (Giant Cell Arteritis)].
Consider other laboratory work-up for nonglaucomatous optic neuropathy: heavy metals, angiotensin-converting enzyme, vitamin B12/folate, rapid plasma reagin, fluorescent treponemal antibody absorption, Lyme titer, antinuclear antibody. If giant cell arteritis (GCA) is a consideration, then check erythrocyte sedimentation rate, C-reactive protein, and complete blood count (CBC) with platelets [see 10.17, Arteritic Ischemic Optic Neuropathy (Giant Cell Arteritis)].
 In cases where a neurologic disorder is suspected, obtain magnetic resonance imaging (MRI) of the brain and orbits with gadolinium and fat suppression if no contraindications are present or CT of the head and orbits with axial and coronal views, preferably with contrast if no contraindications are present.
In cases where a neurologic disorder is suspected, obtain magnetic resonance imaging (MRI) of the brain and orbits with gadolinium and fat suppression if no contraindications are present or CT of the head and orbits with axial and coronal views, preferably with contrast if no contraindications are present.
 Check blood pressure, fasting blood sugar, lipid panel, and CBC (screening for anemia). Refer to an internist for a complete cardiovascular evaluation.
Check blood pressure, fasting blood sugar, lipid panel, and CBC (screening for anemia). Refer to an internist for a complete cardiovascular evaluation.
Treatment
General Considerations
1. Who to treat?
The decision to treat must be individualized. Some general guidelines are suggested.
Is the glaucomatous process present?
Damage is present if the DDLS score is >5, there is visual field loss, there is the presence of an acquired pit or notched rims (irregularity of rims >0.1 rim-to-disc for <2 clock hours), IOP higher than 34 mm Hg, IOP asymmetry more than 10 mm Hg, or disc is <1.5 mm with a cup-to-disc of >0.3.
Is the glaucomatous process active?
Determine the rate of damage progression by careful follow-up. Certain causes of cupping may be static (e.g., prior steroid response). Disc hemorrhages suggest active disease.
Is the glaucomatous process likely to cause disability?
Consider the patient’s age, overall physical and social health, as well as an estimation of his or her life expectancy.
2. What is the treatment goal?
The goal of treatment is to enhance or maintain the patient’s health by halting optic nerve damage while avoiding undue side effects of treatment. The only proven method of stopping or slowing optic nerve damage is reducing IOP. Reduction of IOP by at least 30% appears to have the best chance of preventing optic nerve damage. An optimal goal may be to reduce the IOP at least 30% below the threshold of progression. If damage is severe, greater reduction in IOP may be necessary.
3. How to treat?
The main treatment options for glaucoma include medications, laser trabeculoplasty [both argon (ALT) and selective (SLT)], and guarded filtration surgery (e.g., trabeculectomy). Typically, medications are first-line therapy. Often ALT and SLT are also appropriate initial therapies, especially in patients at risk for poor compliance, with medication side effects, and who have significant posterior trabecular meshwork pigmentation. Surgery may be appropriate initial treatment if damage is advanced in the setting of a rapid rate of progression or difficult follow-up.
Additional treatment modalities, such as tube-shunt procedures, laser cyclophotocoagulation of the ciliary body [with yttrium aluminum garnet (YAG) laser, diode laser, or endolaser], cyclocryotherapy, and cyclodialysis, are typically reserved for IOP uncontrolled by other methods. Some surgeons, however, now use tube-shunt procedures as initial surgery. Other early surgical options include canaloplasty, deep sclerectomy, and trabectome trabecular ablation.
Medications
Unless there are extreme circumstances (e.g., IOP >40 mm Hg or impending loss of central fixation), treatment is started by using one type of drop in one eye (monocular therapeutic trial) with reexamination in 3 to 6 weeks to check for effectiveness.
—Prostaglandin agonists (e.g., latanoprost 0.005% q.h.s., bimatoprost 0.03% q.h.s., travoprost 0.004% q.h.s.) are to be used with caution in patients with active uveitis or cystoid macular edema (CME) and are contraindicated in pregnant women or in women wishing to become pregnant. Inform patients of potential pigment changes in iris and periorbital skin, as well as hypertrichosis of eyelashes. Iris pigment changes rarely occur in blue or dark brown eyes. Those at highest risk for irreversible iris hyperpigmentation are hazel, grey irides.
—Beta-blockers (e.g., levobunolol or timolol 0.25% to 0.5% q.d. or b.i.d.) should be avoided in patients with asthma, COPD, heart block, bradyarrythmia, unstable congestive heart failure, depression, or myasthenia gravis. In addition to bronchospasm and bradycardia, other side effects include hypotension, decreased libido, CNS depression, and reduced exercise tolerance.
—Selective a2-receptor agonists (brimonidine 0.1%, 0.15%, or 0.2% t.i.d. or b.i.d.) are contraindicated in patients taking monoamine oxidase inhibitors (risk of hypertensive crisis) and relatively contraindicated in children under the age of 5 (risk for cardiorespiratory and CNS depression). See 8.11, Congenital/Infantile Glaucoma. Apraclonidine may be used for short-term therapy (3 months), but tends to lose its effectiveness and has a high allergy rate.
—Topical carbonic anhydrase inhibitors (CAIs) (e.g., dorzolamide 2% or brinzolamide 1% t.i.d. or b.i.d.) should be avoided, but are not contraindicated, in patients with sulfa allergy. These medications theoretically could cause the same side effects as systemic CAIs, such as metabolic acidosis, hypokalemia, gastrointestinal symptoms, weight loss, paresthesias, and aplastic anemia. However, systemic symptoms from topical CAIs are extremely rare. There have been no reported cases of aplastic anemia from topical use. Corneal endothelial dysfunction may be exacerbated with topical CAIs and should be used with caution in Fuchs corneal dystrophy and post keratoplasty.
—Miotics (e.g., pilocarpine q.i.d.) are usually used in low strengths initially (e.g., 0.5% to 1.0%) and then built up to higher strengths (e.g., 4%). Commonly not tolerated in patients <40 years because of accommodative spasm. Miotics are usually contraindicated in patients with retinal holes and should be used cautiously in patients at risk for retinal detachment (e.g., high myopes and aphakes).
—Sympathomimetics (dipivefrin 0.1% b.i.d. or epinephrine 0.5% to 2.0% b.i.d.) rarely reduce IOP to the degree of the other drugs, but have few systemic side effects (rarely, cardiac arrhythmias). They often cause red eyes and may cause CME in aphakic patients.
—Systemic CAIs (e.g., methazolamide 25 to 50 mg p.o. b.i.d. to t.i.d., acetazolamide 125 to 250 mg p.o. b.i.d. to q.i.d., or acetazolamide 500 mg sequel p.o. b.i.d.) should usually not be given to patients with a sulfa allergy or renal failure. Potassium levels must be monitored if the patient is taking other diuretic agents or digitalis. Side effects such as fatigue, nausea, confusion, and paresthesias are common. Rare, but severe, hematologic side effects (e.g., aplastic anemia) and Stevens–Johnson syndrome have occurred.
NOTE: Every patient should be instructed to press a tissue into the inner canthus to occlude the punctum for 10 seconds after instilling a drop. Doing so will decrease systemic absorption and reduce allergic blepharitis. If unable to perform punctal occlusion, keeping the eyelids closed without blinking for 3 minutes after drop administration also reduces systemic absorption.
Argon Laser Trabeculoplasty
In some patients, as previously defined, ALT may be used as first-line therapy. It has an initial success rate of 70% to 80%, dropping to 50% in 2 to 5 years.
Selective Laser Trabeculoplasty
The IOP-lowering effect of SLT is equivalent to ALT. SLT utilizes lower energy and causes less tissue damage, which has led to the suggestion that it may be repeatable. This has not been proven.
Guarded Filtration Surgery
Trabeculectomy may obviate the need for medications. Adjunctive use of antimetabolites (e.g., mitomycin-C, 5-fluorouracil) may aid in the effectiveness of the surgery but increases the risk of complications (e.g., bleb leaks and hypotony).
Follow-Up
1. Patients are reexamined 4 to 6 weeks after starting a new b-blocker or prostaglandin or after ALT/SLT to evaluate efficacy. Topical CAIs, a-agonists, and miotics quickly reach a steady state, and a repeat examination may be performed at any time after 3 days.
2. Closer monitoring (e.g., 1 to 3 days) may be necessary when damage is severe and the IOP is high.
3. Once the IOP has been reduced adequately, patients are reevaluated in 3- to 6-month intervals for IOP and optic nerve checks.
4. Gonioscopy is performed yearly and after starting a new-strength cholinergic agent (e.g., pilocarpine).
5. Formal visual fields and optic nerve imaging (e.g., photographs, OCT, or HRT) are rechecked as needed, often about every 6 to 12 months. If IOP control is not thought to be adequate, visual fields may need to be repeated more often. Once stabilized, formal visual field testing can be repeated annually.
6. Dilated retinal examinations should be performed yearly.
7. If glaucomatous damage progresses, check patient compliance with medications before initiating additional therapy.
8. Patients must be questioned about side effects associated with their specific agent(s). They often do not associate eye drops with impotence, weight loss, lightheadedness, or other significant symptoms.
9.2 LOW-PRESSURE PRIMARY OPEN-ANGLE GLAUCOMA (NORMAL PRESSURE GLAUCOMA)
Definition
POAG occurring in patients without IOP elevation.
Symptoms
See 9.1, Primary Open-Angle Glaucoma.
Signs
Critical. See Signs in 9.1, Primary Open-Angle Glaucoma, except IOP is consistently below 22 mm Hg. There appears to be a greater likelihood of optic disc hemorrhages. Some believe visual field defects are denser, more localized, and closer to fixation. A dense nasal paracentral defect is typical. Average CCT is generally 510 to 520 microns.
Differential Diagnosis
NOTE: Determining that optic nerve changes are related to IOP and not another form of optic neuropathy is critical.
 POAG: IOP may be underestimated secondary to large diurnal fluctuations or thin corneas. See 9.1, Primary Open-Angle Glaucoma.
POAG: IOP may be underestimated secondary to large diurnal fluctuations or thin corneas. See 9.1, Primary Open-Angle Glaucoma.
 Shock optic neuropathy from previous episode of systemic hypotension (e.g., acute blood loss, myocardial infarction, coronary artery bypass surgery, arrhythmia). Visual field loss should be nonprogressive.
Shock optic neuropathy from previous episode of systemic hypotension (e.g., acute blood loss, myocardial infarction, coronary artery bypass surgery, arrhythmia). Visual field loss should be nonprogressive.
 Intermittent IOP elevation (e.g. angle-closure glaucoma, glaucomatocyclitic crisis).
Intermittent IOP elevation (e.g. angle-closure glaucoma, glaucomatocyclitic crisis).
 Previous glaucomatous insult with severe IOP elevation that has subsequently resolved. Nonprogressive (e.g., traumatic glaucoma, steroid-induced glaucoma).
Previous glaucomatous insult with severe IOP elevation that has subsequently resolved. Nonprogressive (e.g., traumatic glaucoma, steroid-induced glaucoma).
 Nonglaucomatous optic neuropathy and others. See Differential Diagnosis in 9.1, Primary Open-Angle Glaucoma.
Nonglaucomatous optic neuropathy and others. See Differential Diagnosis in 9.1, Primary Open-Angle Glaucoma.
Etiology
Controversial. Most investigators believe that IOP plays an important role in low-pressure POAG. Other proposed etiologies include vascular dysregulation (e.g., systemic or nocturnal hypotension, vasospasm, or loss of autoregulation), microischemic disease, accelerated apoptosis, and autoimmune disease.
Work-Up
See Work-Up in 9.1, Primary Open-Angle Glaucoma. Also consider:
1. History: Evidence of vasospasm (history of migraine or Raynaud phenomenon)? History of hypotensive crisis, anemia, or heart disease? Previous use of corticosteroids by any route? Trauma or uveitis in past? Has the vision loss been acute or chronic? GCA symptoms? Additional cardiovascular risk factors such as elevated cholesterol, hypertension, and systemic hypotension (including nocturnal “dippers” in the early morning hours)?
2. Check color plates.
3. Check gonioscopy to rule out angle closure, angle recession, or PAS.
4. Consider obtaining a diurnal curve of IOP measurements to help confirm the diagnosis.
5. Consider carotid dopplers to evaluate ocular blood flow. Check blood pressure (consider 24-hour automated blood pressure home monitor).
6. Consider CT or MRI to rule out compressive lesions of the optic nerve or chiasm.
Treatment
1. Research suggests that further lowering of IOP plays an important role in preventing progression of low-pressure POAG. Target IOPs are at least 30% lower than the level at which progressive damage was occurring. Therapies are those for POAG. See 9.1, Primary Open-Angle Glaucoma, for a more in-depth discussion of these therapies.
2. Ischemia to the optic nerve head may play a role in the pathogenesis of low-pressure POAG. Modification of cardiovascular risk factors is appropriate in managing general health, but has not proven beneficial in managing glaucoma. Refer to an internist for control of blood pressure, cholesterol, and optimal management of other comorbid conditions to maximize optic nerve perfusion. Avoid use of antihypertensive drugs at bedtime and use preferentially in the morning.
3. Vasospasm may play a role in the pathogenesis of low-pressure POAG. Some investigators advocate the use of systemic calcium channel blockers in the treatment of this condition. The benefit of these medications has not been well established. Although it may improve capillary perfusion to the optic nerve head, systemic hypotension associated with this therapy may conversely have the opposite effect on ocular blood flow.
Follow-Up
See 9.1, Primary Open-Angle Glaucoma.
9.3 OCULAR HYPERTENSION
Signs
Critical. IOP >2 (or 3) standard deviations (approximately 3 mm Hg) above the average (15 mm Hg in most populations). Normal-appearing, open anterior chamber angle with normal anatomy on gonioscopy. Apparently normal optic nerve and visual field.
Differential Diagnosis
 POAG. See 9.1, Primary Open-Angle Glaucoma.
POAG. See 9.1, Primary Open-Angle Glaucoma.
 Secondary open-angle glaucoma. See 9.1, Primary Open-Angle Glaucoma.
Secondary open-angle glaucoma. See 9.1, Primary Open-Angle Glaucoma.
 CACG: PAS are present on gonioscopy with glaucomatous optic nerve and visual field changes. See 9.5, Chronic Angle-Closure Glaucoma.
CACG: PAS are present on gonioscopy with glaucomatous optic nerve and visual field changes. See 9.5, Chronic Angle-Closure Glaucoma.
Work-Up
1. See 9.1, Primary Open-Angle Glaucoma.
2. If any abnormalities are present on formal visual field testing, consider repeat testing in 2 to 4 weeks to exclude the possibility of learning curve artifacts. If the defects are judged to be real, the diagnosis is glaucoma or ocular hypertension along with another pathology accounting for the field loss.
3. OCT and HRT may reveal glaucomatous optic nerve defects. These objective tests may show pathology earlier than visual field testing.
Treatment
1. If there are no suggestive optic nerve or visual field changes and IOP is <24 mm Hg, no treatment other than close observation is necessary.
2. Patients with an IOP >24 to 30 mm Hg (threshold varies per glaucoma specialist), but otherwise normal examinations are candidates for IOP-lowering therapy. A decision to treat a patient should be based on the patient’s choice to elect therapy and baseline risk factors such as age, CCT, initial IOP, horizontal and vertical C/D ratio, and family history. The results of the ocular hypertension treatment study (OHTS) showed that treatment reduced the development of visual field loss from 9.5% to 4.4% at 5 years, with a 20% average reduction of IOP. However, treatment also caused an increase in cataract and adverse psychological episodes. If treatment is elected, a therapeutic trial in one eye, as described for treatment of POAG, should be used. Some clinicians may elect to monitor these patients with close observation. Risk calculators have been developed to approximate the level of risk progression to glaucoma if left untreated. These may help guide clinicians and patients as to whether treatment should be initiated. See 9.1, Primary Open-Angle Glaucoma.
Follow-Up
Close follow-up is required for patients being treated and observed. All patients should initially be followed similarly to POAG; see 9.1, Primary Open-Angle Glaucoma. If there is no progression in the first few years, monitoring frequency can be decreased to every 6 to 12 months. Stopping medication should be considered.
Reference
Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of POAG. Arch Ophthalmol 2002;120:701–713.
9.4 ACUTE ANGLE-CLOSURE GLAUCOMA
Symptoms
Pain, blurred vision, colored halos around lights, frontal headache, nausea, and vomiting.
Signs
(See Figure 9.4.1.)

FIGURE 9.4.1. Acute angle-closure glaucoma with mid-dilated pupil and shallow anterior chamber.
Critical. Closed angle in the involved eye, acutely increased IOP, microcystic corneal edema. Narrow or occludable angle in the fellow eye if of primary etiology.
Other. Conjunctival injection; fixed, mid-dilated pupil.
Etiology of Primary Angle Closure
—Pupillary block: Apposition of the lens and the posterior iris at the pupil leads to blockage of aqueous humor flow from the posterior chamber to the anterior chamber. This mechanism leads to increased posterior chamber pressure, forward movement of the peripheral iris, and subsequent obstruction of the trabecular meshwork (TM). Predisposed eyes have a narrow anterior chamber angle recess, anterior iris insertion of the iris root, or shorter axial length. Risk factors include increased age, East Asian descent, female gender, hyperopia, and family history. May be precipitated by topical mydriatics or, rarely, miotics, systemic anticholinergics (e.g., antihistamines and antidepressants), accommodation (e.g., reading), or dim illumination. Fellow eye has similar anatomy.
—Angle crowding as a result of an abnormal iris configuration including high peripheral iris roll or plateau iris syndrome angle closure. See 9.13, Plateau Iris.
Etiology of Secondary Angle Closure
 PAS pulling the angle closed: Causes include uveitis, inflammation, laser trabeculoplasty. See 9.5, Chronic Angle-Closure Glaucoma.
PAS pulling the angle closed: Causes include uveitis, inflammation, laser trabeculoplasty. See 9.5, Chronic Angle-Closure Glaucoma.
 Neovascular or fibrovascular membrane pulling the angle closed: See 9.14, Neovascular Glaucoma.
Neovascular or fibrovascular membrane pulling the angle closed: See 9.14, Neovascular Glaucoma.
 Membrane obstructing the angle: Causes include endothelial membrane in iridocorneal endothelial syndrome (ICE) and posterior polymorphous corneal dystrophy (PPCD), and epithelial membrane in epithelial downgrowth (often follows penetrating and nonpenetrating trauma). See 9.15, Iridocorneal Endothelial Syndrome.
Membrane obstructing the angle: Causes include endothelial membrane in iridocorneal endothelial syndrome (ICE) and posterior polymorphous corneal dystrophy (PPCD), and epithelial membrane in epithelial downgrowth (often follows penetrating and nonpenetrating trauma). See 9.15, Iridocorneal Endothelial Syndrome.
 Lens-induced narrow angles: Iris–TM contact as a result of a large lens (phacomorphic), small lens with anterior prolapse (e.g., microspherophakia), small eye (nanophthalmos), or zonular loss/weakness (e.g., traumatic, advanced pseudoexfoliation, Marfan syndrome).
Lens-induced narrow angles: Iris–TM contact as a result of a large lens (phacomorphic), small lens with anterior prolapse (e.g., microspherophakia), small eye (nanophthalmos), or zonular loss/weakness (e.g., traumatic, advanced pseudoexfoliation, Marfan syndrome).
 Aphakic or pseudophakic papillary block: Iris bombe configuration secondary to occlusion of the pupil by the anterior vitreous. May also occur with anterior chamber intraocular lenses.
Aphakic or pseudophakic papillary block: Iris bombe configuration secondary to occlusion of the pupil by the anterior vitreous. May also occur with anterior chamber intraocular lenses.
 Topiramate and sulfonamide-induced angle closure: Usually after increase in dose or within first 2 weeks of starting medication. Usually bilateral angle-closure due to supraciliary effusion and ciliary body swelling with subsequent anterior rotation of the lens–iris diaphragm. Myopia is induced secondary to anterior displacement of ciliary body and lens and lenticular swelling.
Topiramate and sulfonamide-induced angle closure: Usually after increase in dose or within first 2 weeks of starting medication. Usually bilateral angle-closure due to supraciliary effusion and ciliary body swelling with subsequent anterior rotation of the lens–iris diaphragm. Myopia is induced secondary to anterior displacement of ciliary body and lens and lenticular swelling.
 Choroidal swelling: Following extensive retinal laser surgery, placement of a tight encircling scleral buckle, retinal vein occlusion, and others.
Choroidal swelling: Following extensive retinal laser surgery, placement of a tight encircling scleral buckle, retinal vein occlusion, and others.
 Posterior segment tumor: Malignant melanoma, retinoblastoma, ciliary body tumors, and others. See 11.36, Choroidal Nevus and Malignant Melanoma of the Choroid.
Posterior segment tumor: Malignant melanoma, retinoblastoma, ciliary body tumors, and others. See 11.36, Choroidal Nevus and Malignant Melanoma of the Choroid.
 Hemorrhagic choroidal detachment: See 11.27, Choroidal Effusion/Detachment.
Hemorrhagic choroidal detachment: See 11.27, Choroidal Effusion/Detachment.
 Aqueous misdirection syndrome. See 9.17, Aqueous Misdirection Syndrome/Malignant Glaucoma.
Aqueous misdirection syndrome. See 9.17, Aqueous Misdirection Syndrome/Malignant Glaucoma.
 Developmental abnormalities: Axenfeld–Rieger syndrome, Peters anomaly, persistent fetal vasculature/persistent hyperplastic primary vitreous, and others. See 8.12, Developmental Anterior Segment and Lens Anomalies/Dysgenesis.
Developmental abnormalities: Axenfeld–Rieger syndrome, Peters anomaly, persistent fetal vasculature/persistent hyperplastic primary vitreous, and others. See 8.12, Developmental Anterior Segment and Lens Anomalies/Dysgenesis.
Differential Diagnosis of Acute IOP Increase With an Open Angle:
 Glaucomatocyclitic crisis (Posner–Schlossman syndrome): Recurrent IOP spikes in one eye, mild cell, and flare with or without fine keratic precipitates. See 9.8, Glaucomatocyclitic Crisis/Posner–Schlossman Syndrome.
Glaucomatocyclitic crisis (Posner–Schlossman syndrome): Recurrent IOP spikes in one eye, mild cell, and flare with or without fine keratic precipitates. See 9.8, Glaucomatocyclitic Crisis/Posner–Schlossman Syndrome.
 Inflammatory open-angle glaucoma: See 9.7, Inflammatory Open-Angle Glaucoma.
Inflammatory open-angle glaucoma: See 9.7, Inflammatory Open-Angle Glaucoma.
 Retrobulbar hemorrhage or inflammation. See 3.10, Traumatic Retrobulbar Hemorrhage.
Retrobulbar hemorrhage or inflammation. See 3.10, Traumatic Retrobulbar Hemorrhage.
 Carotid–cavernous fistula: See 7.7, Miscellaneous Orbital Diseases.
Carotid–cavernous fistula: See 7.7, Miscellaneous Orbital Diseases.
 Traumatic (hemolytic) glaucoma: Red blood cells in the anterior chamber. See 3.6, Hyphema and Microhyphema.
Traumatic (hemolytic) glaucoma: Red blood cells in the anterior chamber. See 3.6, Hyphema and Microhyphema.
 Pigmentary glaucoma: Characteristic angle changes, (4+ posterior trabecular meshwork band); pigment cells floating in the anterior chamber; pigment line on the posterior lens capsule or anterior hyaloid face; radial iris transillumination defects (TIDs). See 9.10, Pigment Dispersion Syndrome/ Pigmentary Glaucoma.
Pigmentary glaucoma: Characteristic angle changes, (4+ posterior trabecular meshwork band); pigment cells floating in the anterior chamber; pigment line on the posterior lens capsule or anterior hyaloid face; radial iris transillumination defects (TIDs). See 9.10, Pigment Dispersion Syndrome/ Pigmentary Glaucoma.
Work-Up
1. History: Risk factors including hyperopia or family history? Precipitating events such as being in dim illumination, receiving dilating drops? Retinal problem? Recent laser treatment or surgery? Medications (e.g., topical adrenergics or anticholinergics, oral topiramate, or sulfa medications)?
2. Slit-lamp examination: Look for keratic precipitates, posterior synechiae, iris atrophy or neovascularization, a mid-dilated and sluggish pupil, a swollen lens, anterior chamber cells and flare or iridescent particles, and a shallow anterior chamber. Glaukomflecken (small anterior subcapsular lens opacities) and atrophy of the iris stroma indicate prior attacks. Always carefully examine the other eye and compare.
3. Measure IOP.
4. Gonioscopy of both anterior chamber angles. Corneal edema can be cleared by using topical hyperosmolar agents (e.g., glycerin). Gonioscopy of the involved eye after IOP is reduced is essential in determining whether the angle has opened and whether neovascularization is present.
5. Careful examination of the fundus looking for signs of central retinal vein occlusion, hemorrhage, optic nerve cupping, or spontaneous arterial pulsations. If cupping is pronounced or if there are spontaneous arterial pulsations, treatment is more urgent.
6. When secondary angle-closure glaucoma is suspected, B-scan US or US biomicroscopy (UBM) may be helpful.
Treatment
Depends on etiology of angle closure, severity, and duration of attack. Severe, permanent damage may occur within several hours. If visual acuity is hand motions or worse, IOP reduction is usually urgent, and medications should include all topical glaucoma medications not contraindicated, intravenous acetazolamide, and in some cases intravenous osmotic (e.g., mannitol). See 9.14, Neovascular Glaucoma, 9.16, Postoperative Glaucoma, 9.17, Aqueous Misdirection Syndrome/Malignant Glaucoma.
1. Compression gonioscopy is essential to determine if the trabecular blockage is reversible and may break an acute attack.
2. Topical therapy with b-blockers [(e.g., timolol 0.5%) caution with asthma or COPD], a-2 agonist (e.g., brimonidine 0.15%), prostaglandin analogs (e.g., latanoprost 0.005%), and CAIs (dorzolamide 2%) should be initiated immediately. In urgent cases, three rounds of these medications may be given, with each round being separated by 15 minutes.
3. Topical steroid (e.g., prednisolone acetate 1%) may be useful.
4. Systemic carbonic anhydrase inhibitors [e.g., acetazolamide, 250 to 500 mg intravenously (i.v.), or two 250-mg tablets p.o. in one dose if unable to give i.v.] if IOP decrease is urgent or if IOP is refractory to topical therapy. Do not use in topiramate- or sulfonamide-induced angle closure.
5. Recheck the IOP and visual acuity in 1 hour. If IOP does not decrease and vision does not improve, repeat topical medications and give mannitol 1 to 2 g/kg i.v. over 45 minutes (a 500-mL bag of mannitol 20% contains 100 g of mannitol).
6. When acute angle-closure glaucoma is the result of:
a. Phakic pupillary block or angle crowding: Pilocarpine, 1% to 2%, every 15 minutes for two doses, and pilocarpine, 0.5% to 1.0%, in the contralateral eye for one dose.
b. Aphakic or pseudophakic pupillary block or secondary closure of the angle: Do not use pilocarpine. Consider a mydriatic and a cycloplegic agent (e.g., cyclopentolate, 1% to 2%, and phenylephrine 2.5% every 15 minutes for four doses) when laser or surgery cannot be performed because of corneal edema, inflammation, or both.
c. Topiramate- or sulfonamide-induced secondary angle closure: Do not use CAIs. Immediately discontinue the inciting medication. Consider cycloplegia to induce posterior rotation of the ciliary body (e.g., atropine 1% b.i.d. or t.i.d.). Consider hospitalization and treatment with intravenous hyperosmotic agents and intravenous steroids (methylprednisolone 250 mg i.v. every 6 hours) for cases of markedly elevated IOP unresponsive to other treatments. Peripheral iridectomy and miotics are not indicated.
7. In phacomorphic glaucoma, the lens should be removed as soon as the eye is quiet and the IOP controlled, if possible. See 9.12.4, Phacomorphic Glaucoma.
8. Address systemic problems such as pain and vomiting.
9. For pupillary block (all forms) or angle crowding: If the IOP decreases significantly (less than the fellow eye) and the angle is open by gonioscopy, definitive treatment with laser (YAG) peripheral iridotomy or surgical iridectomy is performed once the cornea is clear and the anterior chamber is quiet, typically 1 to 5 days after attack. Patients are discharged on the following medications and followed daily:
 Prednisolone acetate 1% may be helpful.
Prednisolone acetate 1% may be helpful.
 Acetazolamide 500 mg sequel p.o. b.i.d.
Acetazolamide 500 mg sequel p.o. b.i.d.
 Topical b-blocker b.i.d. and/or a-agonist b.i.d.
Topical b-blocker b.i.d. and/or a-agonist b.i.d.
 If phakic, pilocarpine 1% to 2% q.i.d.
If phakic, pilocarpine 1% to 2% q.i.d.
NOTE: Some believe that once the attack is broken, only pilocarpine and prednisolone acetate are necessary if the angle is open.
If IOP does not decrease after two courses of maximal medical therapy, a laser (YAG) PI should be considered if there is an adequate view of the iris. If IOP still does not decrease after a second attempt at a laser PI, then a laser iridoplasty or surgical PI is needed and, in some cases, a guarded filtration procedure.
NOTE: If affected eye is too inflamed initially for laser PI, perform laser PI of the fellow eye first. An untreated fellow eye has a 40% to 80% chance of acute angle closure in 5 to 10 years. Repeated angle-closure attacks with a patent PI may indicate plateau iris syndrome. See 9.13, Plateau Iris.
10. For secondary angle closure: Treat the underlying problem. Consider argon laser gonioplasty to open the angle, particularly in cases that are the result of extensive retinal laser surgery, a tight scleral buckle, or nanophthalmos. Goniosynechialysis can be performed for chronic angle closure of <6 months’ duration. Systemic steroids may be required to treat serous choroidal detachments secondary to inflammation.
Follow-Up
After definitive treatment, patients are reevaluated in weeks to months initially, and then less frequently. Visual fields and stereo disc photographs are obtained for baseline purposes.
NOTE:
1. Cardiovascular status and electrolyte balance must be considered when contemplating osmotic agents, CAIs, and b-blockers.
2. The corneal appearance may worsen when the IOP decreases.
3. Worsening vision or spontaneous arterial pulsations are signs of increasing urgency for pressure reduction.
4. Since one-third to one-half of first-degree relatives may have occludable angles, patients should be counseled to alert relatives to the importance of screening.
5. Angle-closure glaucoma may be seen without an increased IOP. The diagnosis should be suspected in a patient who had pain and reduced acuity and is noted to have:
—An edematous, thickened cornea in one eye.
—Normal or markedly asymmetric pressure in both eyes.
—Shallow anterior chambers in both eyes.
—Occludable anterior chamber angle in the fellow eye.
9.5 CHRONIC ANGLE-CLOSURE GLAUCOMA
Symptoms
Usually asymptomatic, although patients with advanced disease may present with decreased vision or visual field loss. Intermittent eye pain, headaches, and blurry vision may occur.
Signs
(See Figure 9.5.1.)
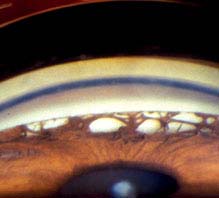
FIGURE 9.5.1. Chronic angle-closure glaucoma with peripheral anterior synechiae.
Critical. Gonioscopy reveals broad bands of PAS in the angle. The PAS block visualization of the underlying structures of the angle. Glaucomatous optic nerve and visual field defects.
Other. Elevated IOP.
Etiology
Prolonged acute angle-closure glaucoma or multiple episodes of subclinical attacks of acute angle closure resulting in PAS, often in superior angle.
 Previous uveitic glaucoma with development of PAS, often in inferior angle.
Previous uveitic glaucoma with development of PAS, often in inferior angle.
 Regressed neovascularization of the anterior chamber angle resulting in the development of PAS.
Regressed neovascularization of the anterior chamber angle resulting in the development of PAS.
 Previous laser to the TM, typically seen with small peaked PAS.
Previous laser to the TM, typically seen with small peaked PAS.
 Previous flat anterior chamber from surgery, trauma, or hypotony that resulted in the development of PAS.
Previous flat anterior chamber from surgery, trauma, or hypotony that resulted in the development of PAS.
NOTE: While acute angle closure is less common in those of African descent, chronic angle closure is more commonly seen in these patients.
Work-Up
1. History: Presence of symptoms of previous episodes of acute angle closure? History of proliferative diabetic retinopathy, retinal vascular occlusion, or ocular ischemic syndrome? History of trauma, hypotony, uveitis, or laser treatment?
2. Complete baseline glaucoma evaluation. See 9.1, Primary Open-Angle Glaucoma.
Treatment
See 9.1, Primary Open-Angle Glaucoma.
1. Laser trabeculoplasty contraindicated in CACG prior to PI and can induce greater scarring of the angle.
2. If patient has angle closure with pupillary block, perform laser peripheral iridotomy to prevent further angle-closure episodes. The TM may have sustained enough damage that the IOP will still be elevated despite a patent iridotomy, necessitating continued use of medications to lower the IOP.
3. Laser iridoplasty may be performed to attempt to decrease the formation of new PAS. This may not be effective, or may serve as a temporary measure; if successful it may be repeated. If iridoplasty fails and other medical therapy has been maximized, the patient may need additional surgery.
Follow-Up
See 9.1, Primary Open-Angle Glaucoma.
9.6 ANGLE-RECESSION GLAUCOMA
Symptoms
Usually asymptomatic. Late stages have visual field or acuity loss. A history of hyphema or trauma to the glaucomatous eye can often be elicited. Glaucoma due to the angle recession (not from the trauma that caused the angle recession) usually takes 10 to 20 years to develop. Typically unilateral.
Signs
(See Figure 9.6.1.)

FIGURE 9.6.1. Angle-recession glaucoma with increased width of the ciliary body band.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


