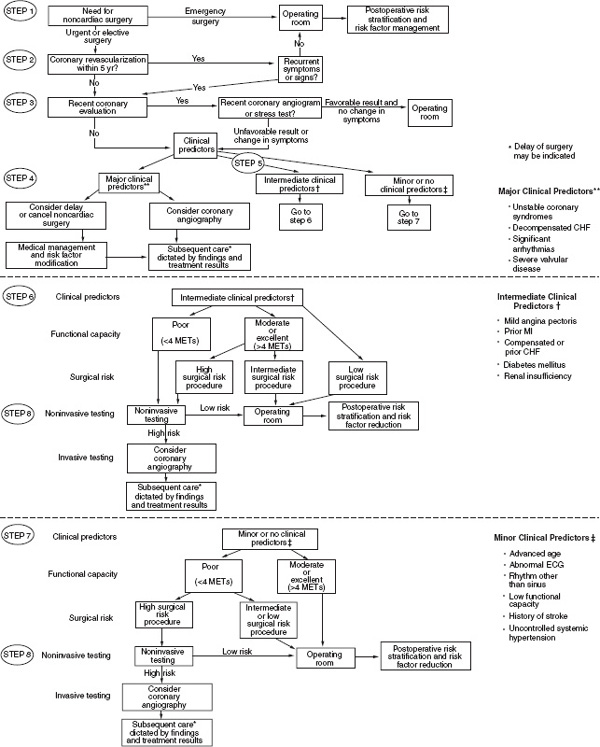
1 The breadth and complexity of ear, nose, and throat (ENT) surgery has increased dramatically in the last few decades. Procedures have become more intricate and delicate, and patients presenting for surgery are now medically more complex. Anesthesia care providers play an integral role in the preoperative evaluation, intra-operative management, and postoperative care of these patients. ■ Preoperative Assessment Preanesthetic evaluation is an essential step in preparing the surgical patient for surgery by assessing the patient’s overall medical condition, planning the appropriate anesthetic technique with informed consent, allaying any anxiety or specific fears, and premedicating the patient when appropriate.1 It is desirable to perform this evaluation prior to the day of surgery because information gathered may elicit the need for further testing. A preoperative evaluation begins with a thorough review of the patient’s chart and medical history, including any prior difficulties with anesthesia, a family history of malignant hyperthermia or pseudocholines-terase deficiency, drug allergies, current medications and medical problems, and a general review of organ systems. Physical examination should focus on the patient’s cardiopulmonary system, a thorough examination of the patient’s airway, and an examination of any other systems as guided by the patient’s medical history. No “routine” laboratory testing is necessary. Testing should be based on the patient’s history, physical examination, and proposed surgical procedure. Narr et al. reviewed the records of 56,119 patients who underwent surgery or a diagnostic test at the Mayo Clinic in 1994.2 Of those 56,119 patients, 5120 (97% of whom were considered healthy) had no laboratory tests done within 90 days of the procedure. Of these patients, 1044 were randomly selected, and their outcome was ascertained. Seventeen laboratory tests were done intraoperatively, and 42 blood tests were done postoperatively. The authors concluded that no test done subsequent to the induction of anesthesia substantially changed the surgical or medical management of these patients, and those patients who have been assessed by history and physical examinations need no preoperative test unless otherwise indicated. Narr et al. found in another study no harm to American Society of Anesthesiologists (ASA). I (healthy) patients by omitting all laboratory testing after an appropriate history taking and physical examination.3 Testing relying on the history and physical can also be applied to functionally intact elderly patients. Domoto et al. studied changes in patient management of 70 functionally intact patients residing at a chronic care facility. The patients underwent admission and yearly screening tests (3903 total tests).4 New “abnormal” (unknown to the managing physician) results were discovered in 13% of admission screenings and in 6% of all tests ordered. Of the 26 abnormal tests, only 4 (0.1%) led to what the authors concluded were minor changes in patient management. Unnecessary testing can be harmful to patients. Roizen et al. examined 386 chest x-rays performed on patients presenting for surgery. Potentially only one patient benefited from the radiographic study (an elevated hemidiaphragm), but three patients suffered harm when invasive tests were conducted on the basis of suspected lung nodules.5 One patient underwent an unnecessary thoracotomy, and the other two patients also suffered morbidity based on information obtained from the screening radiographic study. An unindicated laboratory test may uncover a patient who has mild to moderate hypokalemia (blood potassium between 3.0 and 3.4 mEq/L). The evidence is convincing that the patient who is not on a diuretic does not need a potassium level drawn prior to surgery. In fact, the treatment of mild to moderate hypokalemia is harmful. Approximately 0.5? of all patients given either oral or intravenous potassium supplementation suffer a life-threatening reaction or die as a consequence of potassium administration.6 Unfortunately, even when certain tests are agreed upon, 30 to 40% of patients do not receive them, whereas up to 40% of patients who do not fit criteria for agreed upon tests unnecessarily receive them.7 Medicolegal issues can arise when an unnecessary test is ordered and not followed up in a timely manner. In an era of increasing cost constraints the ordering of unnecessary tests is economically wasteful and potentially harmful to the patient. Tests should be based on history taking and physical examination because they are much more effective screening for disease than laboratory tests alone. Cardiovascular System The major issues when evaluating the cardiovascular system are the presence or absence of hypertension and ischemic coronary disease. Hypertension is the most commonly encountered cardiovascular pathology. An adult is considered to be hypertensive when the systolic blood pressure is 140 mm Hg or greater or when the diastolic pressure is 90 mm Hg or greater on at least two different occasions measured at least 1 to 2 weeks apart.8 Hypertension is a significant risk factor for ischemic heart disease, cerebral vascular disease, congestive heart failure, and end-stage renal disease. Essential hypertension, hypertension of unknown cause, accounts for greater than 95% of all cases.9 Secondary hypertension implies a known etiology of hypertension such as renal and endocrine causes. Preoperative evaluation for patients with hypertension includes determination of the adequacy of blood pressure control, a thorough review of antihypertensive medications, and evaluation for any end-organ manifestations. End-organ involvement maybe elicited by history and physical examination, evidence of ischemia on electrocardiogram (ECG), and evidence of abnormalities on renal function tests. All hypertensive medications except diuretics should be continued perioperatively. Blood pressure of 180/110 or greater is associated with perioperative ischemic events. Elective surgery in this population should be delayed until blood pressure is better controlled.8 Monitoring of all patients should include continuous ECG and frequent noninvasive blood pressure measurements. Depending on the complexity of the surgical procedure and end-organ involvement, invasive blood pressure monitoring and pulmonary artery catheter monitoring may be warranted. Coronary artery disease (CAD) is a major contributor to perioperative morbidity and mortality. The objective of the preoperative cardiac evaluation is to determine the type, severity, and physical limitations of the heart disease.1 Clinical predictors of increased perioperative cardiovascular risk can be found in Table 1–1.10 Fig. 1–1 provides current recommendations for a stepwise approach to preoperative cardiac assessment. Most ear and skull-based surgeries are intermediate- to low-risk procedures. All cardiac medications should be continued perioperatively. In addition, recent reports suggest that the addition of perioperative β-blockers to patients at risk may lower overall cardiac risk. These studies have been relatively small, however, and patients were selected rather than recruited. Current recommendations suggest that patients at intermediate cardiac risk or at high cardiac risk with negative noninvasive testing (stress test) should begin β-blockade up to 30 days prior to hospitalization and continue β-blockade up to 1 month postoperatively. Patients at high risk with positive noninvasive testing require more invasive intervention prior to elective surgery.11 FIGURE 1-1 Recommendations for stepwise approach for preoperative cardiac assessment. CHF, congestive heart failure; ECG, electrocardiogram; METs, multiples of basal metabolic rate; MI, myocardial infarction.(Reprinted with permission from Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative evaluation for non-cardiac surgery: executive summary. Anesth Analg 2002;94:1052-1064.) Respiratory System The disposition of patients presenting for surgery with an upper respiratory infection (URI) is controversial. Elective procedures in patients with a productive cough, purulent nasal drainage, fever, malaise, rhonchi, or abnormal chest x-ray should be postponed. Several studies have demonstrated that airway reactivity remains altered for up to 6 weeks following a URI.12 Patients who are afebrile and have only clear rhinorrhea pose a dilemma. A review by Tait et al. reports that with careful anesthetic management, pediatric patients with URI symptoms can undergo elective procedures without increased morbidity.12 Severity of symptoms, the patient’s respiratory history (reactive airway disease), the anesthetic technique, and the anesthesiologist’s comfort level should all play a role in determining whether to proceed with elective surgery. Few studies address the issue of adults with URI presenting for elective surgery. At present, there is little evidence suggesting increased morbidity and mortality for this patient population undergoing general anesthesia.13 Perioperative management of patients with asthma requires a thorough understanding of the disease process and the medications used to treat it. Intraoperative airway manipulation, especially tracheal intubation, can provoke life-threatening bronchospasm. Risk factors for the development of postoperative pulmonary complications in this patient population include frequency of “attacks,” recent use of antiasthma medications, history of recent hospitalization, and history of tracheal intubation.14, 15 Prior to elective surgery, patients should be free of wheezing, with a peak flow measured on spirometry greater than 80% of predicted.16
General Requirements for Anesthesia in Routine Ear and Skull Base Operations
Major Predictors
Intermediate Predictors
Minor Predictors
Acute or recent myocardial infarction
Mild angina
Advanced age
unstable angina
Previous myocardial infarction
Abnormal electrocardiogram
Decompensated congestive heart failure
Compensated congestive heart failure
Rhythm other than sinus
Significant arrythmia
Diabetes mellitus
Low functional capacity
Severe valvular disease
Renal insufficiency
History of stroke
Uncontrolled hypertension
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


