26 Fungal Sinus Disease • Inhaled fungi can cause both acute and chronic rhinosinusitis • Fungal colonization of the sinuses is common and is rarely of clinical consequence • Acute invasive (fulminant) fungal sinusitis • Chronic invasive fungal sinusitis • Granulomatous invasive fungal sinusitis • Fungal balls (mycelium mass) • Allergic fungal rhinosinusitis • Saprophytic fungi of the mucoracious molds (Mucor, Rhizopus, Absidia) • <4 weeks duration in immunocompromised patients (DM, HIV, neutropenia, chemotherapy) • Rare, high mortality rate—50% with CNS or cavernous sinus involvement • Invades soft tissue and vessels causing local thrombosis, infarction, and necrosis • Patients very unwell with fever, nasal discharge, headache, mental state changes • Necrotic black areas on septum, turbinates, or palate, CN involvement and proptosis • CT—to assess extent and bony involvement (Fig. 26.1), MRI—vascular/intracranial involvement • Requires urgent treatment with surgery (FESS and surgical debridement until normal tissue identified) and high-dose systemic antifungal treatment (amphotericin B or posaconazole, which is the drug of choice) • Treat underlying immune deficiency if possible • Aspergillus fumigatus, dematiaceous molds (Bipolaris, Curvularia, Alternaria) • Locally invasive disease >3 months duration, usually have DM or on corticosteroids • Orbit and CNS invasion less common than in acute type • Presents with chronic sinusitis ± symptoms of local invasion (eye swelling, decrease in vision and eye movement—orbital apex syndrome) • CT of paranasal sinuses—hyperdense soft tissue, demonstrates bony involvement • MRI—hypointense on T1 and very hypointense on T2, intracranial extension • Diagnosis confirmed on biopsy revealing invasion into the surrounding tissues • Histology—bone necrosis with lymphocytes, neutrophils, eosinophils, Langhans cells • Treatment involves urgent surgery (FESS/surgical debridement), systemic antifungals (amphoteracin B—change to itraconazole once controlled, continue for up to 1 year) • Long-term follow-up required as this condition tends to recur • Aspergillus flavus • North Africa, India, Pakistan • Locally invasive disease over at least 3 months duration, immunocompetent • Present with chronic sinusitis and proptosis or enlarging mass in affected sinus • Histology—non-caseating granuloma, foreign body/Langhans giant cells with necrosis • Surgical debridement is required followed by systemic antifungal medication • Recurrence is less common and prognosis good
26.1 Types of Fungal Sinusitis
26.1.1 Invasive
26.1.2 Non-invasive (Majority)
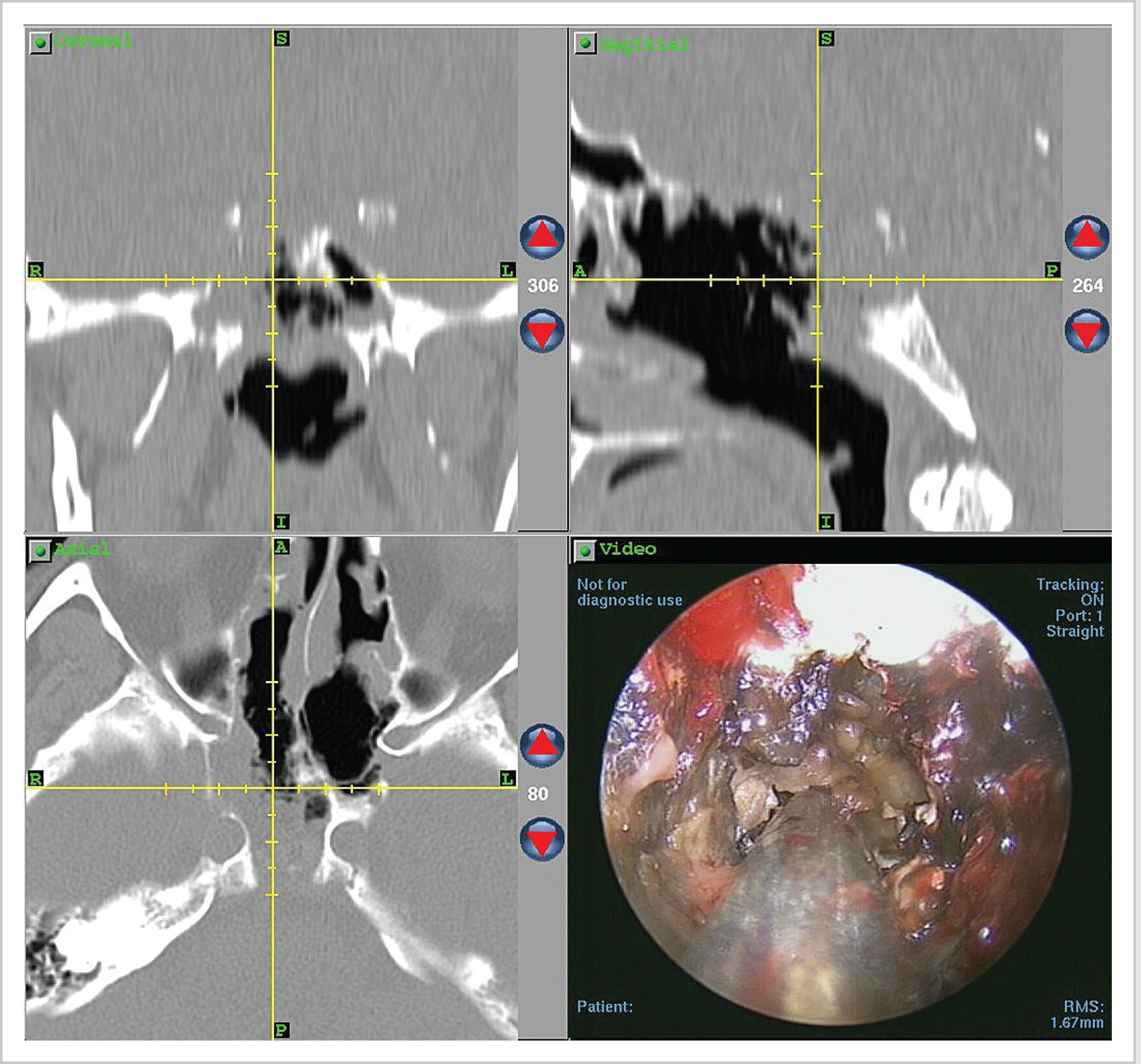
26.2 Acute Invasive (Fulminant) Fungal Sinusitis
26.3 Chronic Invasive Fungal Sinusitis
26.4 Granulomatous Invasive Fungal Sinusitis
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


