CHAPTER 48 Fungal Rhinosinusitis
Fungal rhinosinusitis can be categorized as invasive or noninvasive on the basis of histopathology. These manifestations also depend on the host’s immunologic health. Acute invasive fungal rhinosinusitis occurs in patients with severe immunologic compromise, whereas chronic invasive and the noninvasive forms occur in patients with intact immune systems. Noninvasive forms of fungal rhinosinusitis include fungus balls (in which the immune system is neither over- nor under-responsive) and eosinophilic fungal sinus disease (which is secondary to an over-responsiveness, either allergic or nonallergic, to fungus). These noninvasive eosinophilic manifestations are subdivided into allergic fungal rhinosinusitis (AFRS) and nonallergic eosinophilic fungal rhinosinusitis (NA-EFRS). This latter category, introduced in the late 1990s, is controversial because its proponents contend that fungi mediate a nonallergic eosinophilic immunologic response that is the basis for almost all sinus disease (Table 48-1).
Table 48-1 The Manifestations of Fungal Rhinosinusitis According to Host Immunologic Status
| Host Immunologic Status | Manifestation of Fungal Rhinosinusitis |
|---|---|
| Immunodeficient | Invasive, acute Invasive, chronic |
| Immunocompetent | Invasive, granulomatous Fungus ball |
| Allergic or altered cell-mediated hyperresponsiveness | Allergic fungal rhinosinusitis (AFRS) Nonallergic eosinophilic fungal rhinosinusitis (NA-EFRS) |
Invasive Fungal Rhinosinusitis
Acute Invasive Fungal Rhinosinusitis
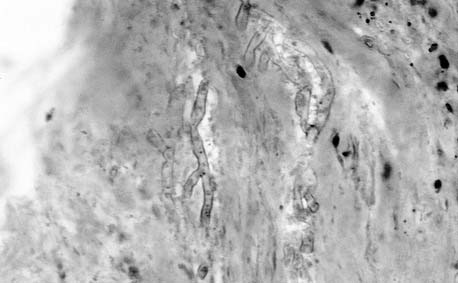
Also called fulminant or rapidly invasive fungal rhinosinusitis, acute invasive fungal rhinosinusitis is almost always confined to the patient with altered host defenses, such as a patient undergoing transplantation, a diabetic patient in ketoacidosis, or a patient with leukemia. As the name implies, the time course is rapid and on histopathologic inspection shows the fungus invading tissue (Fig. 48-1). Invasive fungal rhinosinusitis is suspected when the immunocompromised patient demonstrates a fever and localization of symptoms to the nose or paranasal sinus area, such as orbital swelling, facial pain, or nasal congestion. Nasal endoscopy may show necrosis of the nasal mucosa, which is indicative of mucormycosis, and, in rare situations, actual fungal sporulation. It is more usual to note only edema and changes indistinguishable from those seen in rhinosinusitis from nonfungal causes.
The most common invasive fungal species in both the acute invasive and the indolent or chronic invasive forms of fungal rhinosinusitis varies geographically but is usually an Aspergillus species, frequently Aspergillus fumigatus or Aspergillus flavus. However, many species can become invasive in the setting of immunocompromise, including Scedosporium apiospermum or Pseudallescheria boydii, Fusarium, the Zygomycetes (which cause mucormycosis), and even, rarely, Basidiomycetes (mushrooms).1 With mucormycosis, anesthesia of the nasal mucosa or cheeks, independent of topical anesthetics, is common and precedes the onset of ischemic darkened necrosis of the nasal cavity. The oral cavity should always be examined for invasion through the hard palate from the nose. If the diagnosis is suspected, sinus computed tomography (CT) should be obtained. Changes seen on sinus CT scans or plain radiographs usually are indistinguishable from those in other causes of rhinosinusitis, although in advanced disease, CT may show bony erosion or soft tissue invasion. Unfortunately, abnormal imaging findings are common in immunocompromised patients. Up to 42% of patients with leukemia in one series, for example, had abnormal sinus radiographic findings.2
Aspergillus
The Aspergillus species most commonly responsible for invasive disease in the United States is A. fumigatus. A. flavus is commonly associated with the more indolent, chronic invasive fungal disease seen primarily in the Sudan and in India, but it can also be responsible for fulminant invasive disease regardless of geographic location.3 Therapies and prognosis do not differ among Aspergillus species. Aspergillus species can be angioinvasive, but they do not cause the obliterative invasion seen with mucormycosis. Hemorrhagic infarcts can be seen if there is cerebral involvement.4
Mucormycosis
Mucormycosis is a term commonly used to designate all fungal species within the order Mucorales in the class of the Zygomycetes. The most virulent and common species is Rhizopus oryzae. Mucormycosis has earned the reputation as the most acutely fatal fungal infection known to humans. It is rapidly growing, and within 24 hours, cultures of Mucor species can grow to the top of the culture plate. It is important, if the diagnosis is suspected, that the suspicion be acted on immediately. Mucor has a propensity for vascular invasion and obliteration leading to ischemia. Unusual species in the family, such as Apophysomyces elegans, may afflict the immunocompetent patient, but usual treatment is curative.5,6
The growth of Mucor is facilitated by acidotic conditions, and as the fungus grows, it facilitates its propagation by this vascular invasion, leading to ischemia. The use of hyperbaric oxygen in this setting is theoretically attractive because it reduces the ischemia and acidosis, but no controlled studies have shown its efficacy. Hyperbaric oxygen is a relatively benign therapeutic option, and in these life-threatening situations it can be added to the therapeutic regimen. Patients with poorly controlled diabetes, particularly with diabetic ketoacidosis, are uniquely at risk for invasive mucormycosis. Normal human serum can inhibit the growth of Rhizopus (the most virulent of the species within the order Mucorales), but the serum of patients with diabetic ketoacidosis actually may enhance fungal growth.7,8 The mechanism of this increased susceptibility to mucormycosis may be attributable to altered transferrin binding in diabetic patients, which makes iron more readily available.9 Patients receiving renal dialysis and deferoxamine also are at higher risk for mucormycosis.10 The importance of iron in the physiology of invasive mucormycosis is demonstrated in clinical scenarios and in vitro studies, although the growth of Aspergillus or Candida is affected to a much lesser degree by the availability of iron.11 Other causes of immunocompromise also lead to mucormycosis, including defects or reduction in neutrophils and the immunosuppression caused by steroids. Unlike leukemia or bone marrow failure, diabetic ketoacidosis is readily reversed. The survival rates in those with invasive mucormycosis reflect the variation in ability to reverse the underlying predisposing cause. Up to 80% of diabetic patients survive the disease, whereas less than 50% of nondiabetic patients do so.12
Chronic or Indolent Invasive Fungal Rhinosinusitis
Chronic, also known as indolent, invasive fungal rhinosinusitis more frequently occurs in patients with no or with limited immunocompromise. Symptoms are slowly progressive over many weeks to months, in contradistinction to the rapidly fatal course of untreated acute invasive fungal rhinosinusitis. The diagnosis of chronic invasive rhinosinusitis should be suspected in patients with any element of immunocompromise or with complications of rhinosinusitis such as cranial neuropathy or orbital extension. Chronic invasive fungal rhinosinusitis is rare. It has been detailed most compellingly in articles from the Sudan, where the pathogenic organism was always A. flavus. The histologic picture is that of a granuloma in which giant cells contain the hyphae. In this setting, immunocompetent patients present with painless proptosis.13 Other fungal species that can cause an indolent invasive fungal rhinosinusitis with extension to the orbit or palate are A. fumigatus,14 Alternaria,15 P. boydii, Sporothrix schenckii,16 and Bipolaris species.16 The host is seemingly immunocompetent, and the disease course is variable. In some patients, surgical exenteration is curative, and in others, the disease is relentless despite multiple therapies, including systemic antifungal drugs and surgery, and may end in blindness, cerebral extension, or death.17 Patients who live in Africa or India are disproportionally afflicted with granulomatous invasive fungal rhinosinusitis.
Therapy and prognosis are currently the same for both granulomatous and nongranulomatous forms of chronic invasive fungal rhinosinusitis. Therapy usually involves surgery and antifungal therapy. Very few centers perform fungal cultures with determination of antifungal sensitivities. Culture specimens can be sent to the University of Texas Fungus Testing Laboratory at the University of Texas Health Science Center in San Antonio for determination of sensitivity to various antifungal agents. In the United States, nongranulomatous chronic invasive rhinosinusitis is more common, but still rare. Usually there is no identifiable immunodeficiency.15,18
Diagnosis
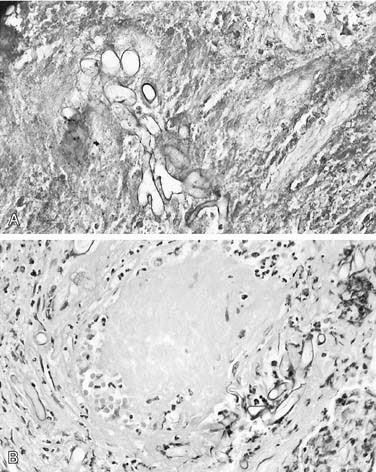
Biopsy of the suspected tissue for pathology and culture is critical to making the diagnosis of invasive fungal rhinosinusitis. Histopathologic findings of hyphae within tissue establish the diagnosis of invasive fungal rhinosinusitis, with detection enhanced by the use of special stains for fungus. Fungal culture specimens should be obtained, preferably before the initiation of systemic antifungal therapy. Initiation of therapy, prior to culture, decreases the likelihood that the fungus will grow on culture. It is critical that the diagnosis, once suspected, be made as quickly as possible. Therefore, a frozen section of the pathologic specimen or evaluation of the material submitted for culture by immediate fungal stains, such as calcofluor white (Fig. 48-2) should be requested, and if results of either of these examinations are positive for fungus, appropriate antifungal therapy and extended surgical resection can be initiated without delay.19

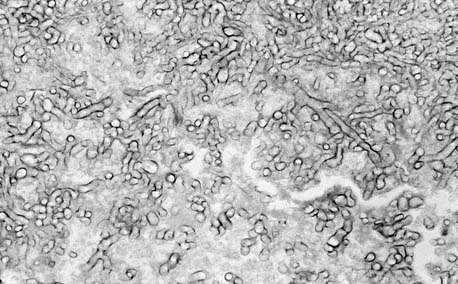
Neither frozen section of the involved tissue nor special stains for fungus will definitively distinguish between fungal species, although mucormycosis can be suspected if the fungal elements seen are broad ribbon–like (10 to 15 µm), irregular, and rarely septated (Fig. 48-3). The artifacts of frozen section may cause Aspergillus hypha elements to appear swollen and similar to those of mucormycosis. Generally, the distinction between mucormycosis and Aspergillus species can be made on permanent histopathologic sections. The Aspergillus species demonstrate more narrow hyphae with regular septations and 45-degree branching on histopathology (Fig. 48-4). Cultures are important for distinguishing Aspergillus species from less common pathogenic fungal species that are septated, such as Fusarium, Alternaria, and P. boydii.20
Therapy
Therapy of invasive fungal rhinosinusitis requires reversal of the underlying predisposing condition, appropriate systemic antifungal therapy, and surgical débridement. Of these, the most important is reversal of the underlying cause of immunocompromise.21 If the source of immunocompromise is profound and irreversible, the treatment will not be successful, and mutilating and painful adjuncts should be avoided. Some patients may benefit from infusion of granulocytes in an attempt to reverse immunocompromise, although reports of this procedure are anecdotal.
Invasive fungal rhinosinusitis in the immunocompetent patient is rare and the course is generally chronic, although it may still be lethal. The therapy for chronic invasive fungal rhinosinusitis, both granulomatous and nongranulomatous, is similar to that for acute invasive fungal rhinosinusitis, except for correction of immunodeficiency.16,22 Management includes endoscopic débridement, often on multiple successive occasions, combined with both systemic and topical antifungal therapies targeted to the sensitivities of the fungus isolated. This approach has largely replaced external surgical approaches. External débridement may be required for orbital exenteration or if bleeding precludes endoscopic diagnosis and débridement.23
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


