Fungal Keratitis in Contact Lens Wearers
Brett A. Levinson
Kristin M. Hammersmith
Elisabeth J. Cohen
Contact lenses are widely used for correction of refractive error and for cosmetic purposes. Over 30 million Americans use contact lenses, and the risk of infection, while low, is well known to eye care professionals.1 Infections secondary to contact lens use are most commonly associated with bacterial pathogens. Fungal keratitis, while less common, is an increasingly recognized risk of contact lens use, and often with devastating visual outcomes. Recently, increased attention has been focused on fungal infections due to an outbreak of Fusarium keratitis associated with one brand of a multipurpose contact lens solution. However, in addition to the recent Fusarium outbreak, an overall increase in rates of fungal keratitis has been noted in the past several years. This chapter will review fungal keratitis associated with contact lens wear.
Fungi may be commensal organisms of the ocular surface, and studies of normal eyes have found fungal isolates in 3% to 28% of conjunctival cultures. Fungal keratitis is less common than bacterial keratitis, comprising 6% to 20% of infectious keratitis cases, depending on the study. Fungal keratitis is more common in subtropical or tropical climates, such as southern Florida and India. In the temperate areas of the United States, Candida sp. and Aspergillus sp. have been the most common isolates with Fusarium sp. more common in the south.2 However, recently, an increase in Fusarium related infections due to contact lens use have been reported across the country and worldwide.
Clinically, fungal keratitis can present similarly to other types of microbial keratitis with an epithelial defect, stromal infiltration and edema, conjunctival hyperemia, and anterior chamber reaction and hypopyon, but often with a more indolent course, at least initially. Several characteristic findings of filamentous fungi include elevated, branching, grey-white ulcers, feathery margins, satellite lesions, and endothelial plaques (Fig. 1). Yeasts can appear clinically similar to bacterial infections. The onset of fungal keratitis is typically subacute compared to the acute onset of bacterial keratitis.2
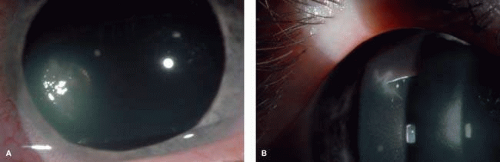 FIGURE 1. A. Left eye of 21-year-old soft contact lens user (2-week replacement), history of ReNu with MoistureLoc use, with Fusarium keratitis. Note the satellite lesions. Patient treated with topical voriconazole with resolution of infection and residual peripheral scarring. Final vision 20/20. B. Right eye of same patient, photo taken on the same day. Note the variability in clinical presentation in this patient with bilateral Fusarium keratitis. Resolution with topical voriconazole. Final vision 20/20. |
Trauma has been reported as the most common cause of fungal keratitis from filamentous organisms, whereas Candida is more common in eyes with chronic disease and in immunocompromised patients. A review of fungal keratitis cases seen between 1982 and 1992 at the Bascom Palmer Eye Institute in Miami examined 125 cases of fungal keratitis, of which 44% were due to trauma. In this series, Fusarium was the most common isolate and was seen in 62% of the patients.3 A study in Singapore examined 29 cases of fungal keratitis seen between 1991 and 1995. Over half of the cases were associated with trauma, whereas only two patients had a history of contact lens use.4 A review of fungal keratitis at the New York Eye and Ear Infirmary between 1987 and 2003 identified 61 cases, of which 29 (48%) were due to Candida albicans, and nine other cases due to other Candida species. The most common risk factors in this study included HIV positivity and chronic ocular surface disease, whereas trauma as an etiology was less common. In contrast to studies in Miami, Fusarium was uncommon, accounting for only six of 61 cases.5
Historically, fungal keratitis has been infrequently associated with contact lens use. In a review of fungal keratitis from 1972 to 1987, Wilhemus reported that four of 90 patients (4%) wearing cosmetic contact lenses and four of 15 patients (27%) wearing therapeutic contact lenses developed fungal infections.6 A review of cases seen at Bascom Palmer between 1969 and 1977 found only three cases of contact-lens-associated fungal keratitis.7 A follow-up study at the same institution reviewed 573 cases of infectious keratitis from 1977 to 1982. Of the 64 culture-positive cases associated with contact lens use, only two (3%) were caused by fungi. In contrast, of the 264 culture-positive cases not associated with contact lens use, 63 (24%) were caused by fungal organisms. This finding led the authors to postulate that contact lenses may have a protective effect against the development of fungal keratitis.8 Similarly, between 1982 and 1992, only five cases of fungal keratitis associated with contact lens use was noted at Bascom Palmer. Four patients wore extended wear contact lenses, and one patient had a therapeutic bandage lens.3
A retrospective study at Wills Eye Hospital in Philadelphia examined records from 1991 to 1999 and found 24 cases of fungal keratitis, of which seven cases were associated with contact lens use. Five patients were using planned replacement hydrophilic soft contact lenses, one patient was wearing a daily-wear rigid gas permeable, and one patient was wearing a bandage contact lens. All patients in the study using contact lenses for correction of refractive errors developed Fusarium keratitis. This study found Candida to be the most common fungal isolate overall, whereas Fusarium was the most common filamentous species.9
Koidou-Tsiligianni et al. reviewed 658 cases of ulcerative keratitis at Bascom Palmer. No fungal keratitis was found in the contact lens group as compared to 40 cases (17%) in the noncontact lens group. (Koidou-Tsiligianni, 1989) In a case-controlled study published in 1997 comparing bacterial keratitis to fungal keratitis, Wong et al. reported that bacterial keratitis was more likely to be associated with contact lens use, whereas fungal keratitis was significantly more likely to be associated with ocular trauma and less likely to be associated with contact lens use.10
Studies from the 1980s examined the susceptibility of extended wear soft contact lenses to fungal growth. Yamaguchi et al. exposed contact lenses with water-contents of 45% and 73.5% to Fusarium solani and Aspergillus flavus on Sabouraud agar. Penetration of the contact lenses occurred in both types of lenses, but the fungi grew more vigorously in the lenses with the higher water content.11 (Current soft lenses have higher water contents than the prior generation of lenses.) Wilson and Ahearn described fungal growth on 11 extended wear contact lenses, which in most cases were known to have been contaminated while on the eye.12 A follow-up study examining these 11 contact lenses with electron microscopy found that a contact lens with greater than 55% water content created a suitable environment for saprophytic fungi. In vitro tests of these lenses demonstrated that fungi could penetrate the lens in 4 to 7 days of continuous exposure.13
ReNu with MoistureLoc Fungal Keratitis
Recently, however, a paradigm shift has occurred in the thinking about fungal keratitis and contact lens use in part due to an outbreak in contact lens-associated Fusarium keratitis. An insurgence of Fusarium keratitis in Singapore was first recognized in February 2006, at which point, 54 patients were identified over the previous 12 months.14 The Centers for Disease Control (CDC) first received a report from a New Jersey ophthalmologist about three patients in March of 2006 with contact-lens-associated Fusarium keratitis. An association between cases and use of a particular multipurpose solution, ReNu with MoistureLoc (Bausch & Lomb, Rochester, NY) was noted, prompting an investigation of Bausch & Lomb’s manufacturing plant, and a review of contact lens related Fusarium cases. After the initial reports from the Pacific Rim, several physicians from geographically diverse locations in the United States began to report an increasing incidence of contact lens-related Fusarium keratitis. Similar to the reports from East Asia, the incidence was significantly out of proportion to previously noted rates of disease.14,15
Khor et al. reviewed the experience of Fusarium keratitis in Singapore from March 2005 to May 2006. During this time period 42 (64%) of patients were known users of ReNu with MoistureLoc. Five patients required emergent penetrating keratoplasty. Contact lens hygiene was noted to be suboptimal in over 80% of patients including the use of contacts past the replacement date, overnight use of daily lenses, and swimming with lenses. A cluster of 33 patients with contact lens-associated Fusarium keratitis was also reported in Hong Kong, and Bausch & Lomb suspended sale of the ReNu brand solutions in the Pacific Rim in February 2006.14
In the United States, Alfonso et al. reported 34 cases between January 2004 and April 2006 at Bascom Palmer.16 Bernal et al. documented four cases during a 5-week period in 2006 at the University of California, San Francisco.17 Gorscak et al. reported on 11 cases of contact lens-associated Fusarium keratitis between October 2005 and April 2006 at the University of Medicine and Dentistry of New Jersey and the Wills Eye Hospital.18 Jeng et al. reported three cases of contact lens related Fusarium keratitis in MoistureLoc users in Cleveland, Ohio, from November 2005 to March 2006.19 Twenty cases were noted in Puerto Rico between October 2005 and April 2006.20
In a pivotal paper in the Journal of the American Medical Association, physicians from the CDC reviewed cases of contact lens-associated Fusarium cases between June 2005 and July 2006 and identified 164 confirmed cases, of which 55 (34%) required corneal transplantation (Fig. 2). The only statistically significant association found after multivariable analysis was use of MoistureLoc multipurpose solution in the month prior to symptom onset. MoistureLoc was manufactured in one location for distribution to the United States, Hong Kong, and Singapore. No evident cause of contamination in the production of MoistureLoc was noted. No fungus was cultured from the bottles of MoistureLoc at the site of production or from bottles submitted by patients with Fusarium keratitis in the CDC investigation.15
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


