and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Faden operationPosterior fixation sutureSixth nerve paresisHigh AC/A ratioFaden with Rectus recessionThe faden operation, also termed posterior fixation suture, is used to weaken the rotational force of a rectus muscle when the eye rotates towards the faden muscle. Faden is the German word for suture, so it is inappropriate to call the procedure “faden suture” (i.e., suture-suture).
20.1 How a Faden Works
The faden procedure is performed by suturing the rectus muscle to sclera, 12–14 mm posterior to the rectus muscle insertion. This pins the rectus muscle to the sclera, so when the eye rotates towards the fadened muscle, the arc of contact cannot unravel. The faden suture thus creates a new insertion posterior to the original insertion. This posterior insertion shortens the moment arm when the eye rotates towards the fadened muscle. Shortening the moment arm reduces the rotational force as the eye rotates towards the fadened muscle (Fig. 20.1).
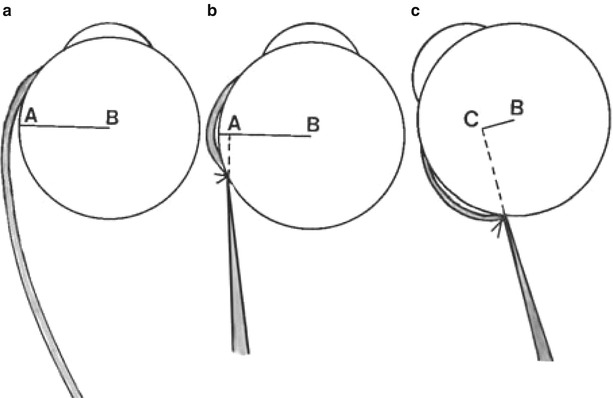
Fig. 20.1
(a) This drawing shows the normal length of the moment arm when the eye is in primary position (line A–B). The moment arm equals the radius of the eye. (b) A faden pinning a rectus muscle 12 mm posterior to the muscle’s insertion. The length of the moment arm remains unchanged with the eye in primary position (line A–B). (c) The eye rotated toward the fadened muscle. When the eye rotates towards the fadened muscle, the moment arm is significantly shortened (line C–B), because of the new posterior insertion site caused by the faden procedure. When the eye rotates away from the fadened muscle, the moment arm is the full radius of the eye. Thus the faden procedure only reduces rotational force when the eye moves towards the fadened muscle
20.2 Indications for Faden Operation
In most cases, the faden operation is combined with a recession, as the effect of the faden operation by itself is relatively small. The faden operation works best on the medial rectus muscle because the medial rectus muscle has the shortest arc of contact (6 mm). The short arc of contact of the medial rectus muscle is dramatically changed by a 12–14-mm faden. Alternatively, the lateral rectus muscle is not affected very much by the faden because the arc of contact is 10 mm, and pinning the muscle at 12–14 mm does not significantly change this naturally long arc of contact. Therefore, the faden operation is usually indicated to correct incomitance found with esotropia, by enhancing the effect of a medial rectus recession.
20.2.1 Sixth Nerve Paresis
An example of where the faden may be most effective is with a partial sixth nerve palsy. The standard surgery has historically been a recession of the medial rectus muscle and resection of the lateral rectus muscle on the paretic eye. This surgery helps to correct the esodeviation in primary position, but it does not address the large esotropia that occurs to the side of the paretic eye. A faden operation of the contralateral medial rectus muscle (yoke muscle to the paretic lateral rectus muscle) could improve this lateral incomitance. An alternative to the standard ipsilateral recession/resection is to add a small medial rectus recession with a faden to the contralateral medial rectus muscle. A faden to the contralateral medial rectus muscle helps correct the esotropia that increases to the side of the paretic lateral rectus muscle by decreasing the rotational force of the yoke medial rectus, thus matching the paretic lateral rectus muscle. Matching yoke muscles only works if there is good lateral rectus function, with only −1 to −2 limitation of abduction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


