26
Facial Reanimation and Eye Care
Facial appearance and expression are greatly emphasized in our society. Facial paralysis may be a devastating ordeal for the patient because it hinders mastication, speech production, and eye protection, but perhaps the most emotionally devastating loss is the ability to smile. The ability to restore symmetry and motion to patients afflicted with facial paralysis is one of the most rewarding skills of the reconstructive surgeon. Numerous reanimation techniques have been developed and utilized to rectify facial paralysis. This chapter discusses issues related to facial reanimation and eye care.
No one modality is universally appropriate for all afflictions of facial nerve function. Etiology of the paralysis, oncological status, type of injury, and location of injury all contribute to the selection of the most appropriate reanimation methods. Currently, reanimation techniques are classified into four types: neural methods, musculofascial transpositions, facial plastic procedures, and prosthetics.
Although no one treatment course is appropriate for restoration of facial nerve function following injury, as a general rule, the order of preference for restoration of function following total unilateral facial paralysis12 is as follows:
1. Spontaneous facial nerve regeneration (observation)
2. Facial nerve neurorrhaphy (facial nerve anastomosis)
3. Facial nerve cable graft (interposition grafts)
4. Nerve transposition (anastomosis to other motor nerves)
5. Muscle transposition
a. Dynamic musculofascial transpositions
b. Static musculofascial transpositions
6. Eyelid procedures and prosthetics
Realistic expectations must be established at the initial encounter and candidly discussed between the physician, the patient, and the family.3 Several points should be emphasized to the patient prior to onset of treatment. First, no reanimation technique will restore the face exactly to its preparalyzed condition. Second, the patient should understand that despite the most meticulous surgery, some degree of synkinesis and residual weakness might persist. Finally, it is also important to stress that the results of these reanimation techniques may be augmented by physical therapy and rehabilitation. Table 26–1 offers some guidelines in managing facial nerve dysfunction.
■ Location of Injury
Intracranial
Intracranial nerve injuries most commonly occur during resection of acoustic neuroma or other cerebellopontine angle (CPA) tumors. The incidence offacial nerve injury following CPA tumor surgery is reported to be 2.3%.1 In the event of facial nerve injury during CPA tumor surgery, immediate repair either by direct anastomosis or by graft is advisable. If added length is needed, careful rerouting of the tympanic and mastoid segments of the nerve may add enough length for an end-to-end anastomosis. Interposition grafts may be placed from the intracranial nerve segment to the temporal segment or from the intracranial nerve segment to the extracranial segment, thus bypassing the temporal bone (Fig. 26–1A,B). Despite the technical difficulties of intracranial repair of the facial nerve, it is a highly reliable technique to restore facial function. Arriaga and Brackmann report that 87.5% of patients undergoing this type of repair developed some degree offacial function, with 57% achieving House Brackmann grade IV or better.2
Problem | Prevention/Treatment |
|---|---|
Partial facial nerve function | Observation |
Delayed complete facial paralysis-both traumatic and postsurgical | Observation |
Delayed facial paresis progressing to paralysis | Serial electroneurography and exploration should there be greater than 95% nerve degeneration within 14 days |
Complete and immediate facial paralysis following surgery | Observe for several hours to rule out paresis secondary to the effect of local anesthetics If no return, explore for any signs of inadvertent, unnoticed facial nerve injury |
Recognized intraoperative facial nerve injury | Immediate neurorrhaphy |
Recognized facial nerve injury with adequate length for tension-free repair | Primary end-to-end nerve anastomosis |
Recognized facial nerve injury with questionable length for tension-free repair | Primary anastomosis using an interpositional cable graft |
Recognized facial nerve injury with no viable proximal nerve trunk | Nerve crossover anastomosis (i.e., hypoglossal-facial crossover) |
Recognized facial nerve injury with no viable proximal nerve trunk and no available ipsilateral donor motor nerve | Cross-facial nerve grafting |
Long-standing facial paralysis (>3 years) | Free muscle transfer (i.e., rectus abdominis or gracilis free flap) |
Facial paralysis with large ipsilateral facial soft tissue defect | |
Synkinesis | Consider Botox |
Eye care | Lubrication using artificial tears, ointment, and moisture chamber Surgical procedures including gold weight procedures, palpebral springs, canthoplasties, and lid resection |
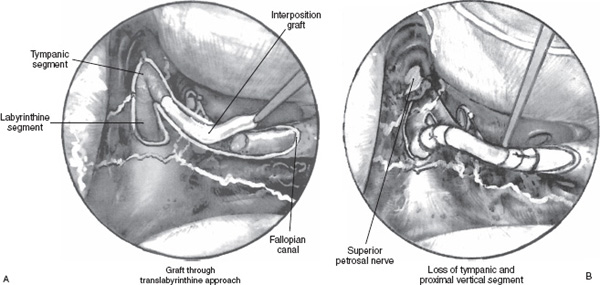
FIGURE 26-1 (A,B) In cases of loss of the tympanic and proximal vertical segment of the facial nerve, an interposition graft may be placed through a translabyrinthine approach.
Intratemporal
Intratemporal facial nerve injury is usually encountered in patients following external head trauma with skull base fractures or iatrogenic injury during or following otologic surgery. The majority of temporal bone fractures result from motor vehicle accidents and violent encounters. Seven to 10% of these fractures result in facial nerve dysfunction. In temporal bone trauma, facial nerve injury most often occurs in the perigeniculate and labyrinthine sections, with axonal degeneration extending a variable distance in both directions. Management of facial nerve injury following temporal bone trauma is controversial. It is accepted, in most cases, that patients who present with complete paralysis at the time of injury have a poorer prognosis than those with incomplete or delayed paralysis. Chang and Cass proposed a reasonable algorithm for management of intratemporal facial nerve injury in which patients with delayed onset or incomplete paralysis are observed.3 If the paralysis progresses from paresis, then serial electroneurography (ENoG) should be performed. Patients with immediate complete paralysis should be monitored with serial ENoG. If ENoG shows greater than 95% degeneration in the first 14 days postinjury, the patient should be offered the option of facial nerve exploration and decompression. During surgery the entire length of the nerve from the meatal foramen to the stylomastoid foramen should be exposed and inspected. Nerve repair should be accomplished via primary anastomosis or graft.3
Intratemporal nerve injury occurs in 0.6 to 3.6% of otologic procedures. Green et al found that mastoidectomy, with or without tympanoplasty, is the most common otologic procedure resulting in facial nerve injury.4 Facial nerve injury during tympanoplasty alone and during removal of exostoses has been reported. Patients with previous surgery, infection, tumor, or congenital anomalies of the ear are at a higher risk for inadvertent nerve injury.4 If the injury is recognized immediately, it should be repaired during the primary procedure. If the facial paralysis is recognized post-operatively and does not recover over several hours, it should be explored. Delayed-onset paralysis should be monitored with serial ENoG and explored if more than 90% degeneration occurs within the first week.
Extratemporal
Extratemporal injury to the facial nerve may occur during parotid surgery, temporomandibular joint procedures, or facelift procedures, or following traumatic lacerations of the face. The incidence of facial nerve paralysis following uncomplicated parotid procedures is reported at 20% for temporary palsy and 10% for permanent paresis of either the temporal or the mandibular branches. Patients at higher risk for facial nerve injury during parotid surgery include children and those undergoing a total parotidectomy.
If the nerve is resected due to tumor, clear nerve margins should be confirmed histologically prior to repair by direct anastomosis or graft.
Inadvertent transection of the nerve that is recognized during parotid surgery should be repaired immediately. Postoperative paralysis when the facial nerve is known to be intact will usually recover spontaneously within 6 months. These patients can be monitored initially with nerve function tests. If the response to stimulation is lost within the first 5 days, severe nerve injury has occurred, and surgical exploration should be considered. If the response to EMG remains normal, it can be assumed that the nerve is intact and recovery can be expected. Traumatic or iatrogenic transections involving the main trunk and segmental branches of the facial nerve should be explored and repaired as soon as they are recognized.
■ Facial Nerve Repair
Direct Nerve Repair
As a rule, direct neurorrhaphy is the most effective way to reanimate the paralyzed face. The interrupted neural pathway can be reestablished either by direct anastomosis or by inserting a graft between the disrupted segments. Some of the key points in nerve repair are early identification, evaluation of nerve condition, and tension-free anastomosis.
Facial Nerve Anastomoses
The best time to perform surgery is within the first 72 hours, before degeneration has occurred and while the distal nerve can still be stimulated. The disrupted nerve should be approximated with minimal tension. It may be necessary to reroute the nerve within the temporal bone or to gain extra length by releasing the nerve. Factors that influence the success of repair include tension, the character of the wound, the presence of scar tissue, and time lag to repair. The subject of radiation remains controversial. Some authors claim that there is no difference in the functional results in patients who have received a full dose of postoperative radiation.5 7 On the other hand, some authors state that radiotherapy results in a poorer outcome with reduced nerve function.8 If the injury is intratemporal, sutures are often unnecessary, and placing the nerve ends in contact is usually satisfactory.9, 10
The surgical suturing technique for nerve repair requires magnification, either with loupes or with a surgical microscope. The nerve endings should be freshened with a new scalpel blade.11 At this point, axoplasm may be seen oozing from the proximal stump. Number 9-0 or 10-0 nylon sutures with a 75 or 100 mm needle should be used.
If possible, three or four simple sutures should be placed about the circumference of the epineural layers to achieve adequate union. Although some authors have suggested the use of perineural, endoneurial, or intrafascicular repairs, these techniques have not proven advantageous. It is, however, important to maintain the size match between both surfaces. This must be inspected with magnification, and if a mismatch is evident, one end may be trimmed in a beveled fashion to obtain a better surface area match of the ends to be approximated.
Sutureless methods have been advocated, including the use of fibrin glues and tissue adhesives. Some authors have shown that neural anastomoses with tissue adhesives yield results similar to nerve suture.12 Others, however, have abandoned this method because of foreign body reaction-increased fibrosis and inferior results. Tubulization with alloplastic materials13 and trophic factors such as insulin-like growth factor14 are considered experimental at this time.
Facial Nerve Repair with Graft
In cases where patients have undergone prior surgery or if part of their facial nerve has been sacrificed or avulsed as a result of severe trauma, direct nerve repair is impossible, and interposition of a nerve graft is required. This technique is reserved for cases where direct nerve repair would result in excess tension or when there is loss of nerve tissue.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


