OVERVIEW
- The benefits of facial plastic surgery are improved appearance and self-confidence, improved facial function and cure from neoplastic disease
- Septorhinoplasty is indicated for elective improvement of nasal function, aesthetic and nasal deformity
- Septoplasty alone may not restore nasal airway function and additional bony and external nasal cartilage surgery may be necessary
- The operating surgeon should be skilled in the management of both nasal form and nasal function
- There are three features that need to be surgically corrected with pinnaplasty: unfurling of the anti-helix, deep conchal bowl and/or prominent ear lobe(s)
- Non-melanotic skin tumours (NMSTs) are basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (cSCC)
- The treatment of BCC depends on size and histology
- The treatment of cSCC is surgical, and must be followed up to detect recurrence and possible cervical nodal metastases
Facial plastic surgery encompasses the management of patients requesting/requiring aesthetic change and/or correction of functional, traumatic and neoplastic disorders of the skin, soft tissues and facial skeleton. In both groups these conditions may be congenital or acquired.
In the neoplastic group of conditions, management of non-melanotic skin tumours (NMSTs) forms a sizeable part of our workload. Bearing this in mind, the NMSTs tend to be treated within the broad confines of multidisciplinary clinics. Treatment is surgical and non-surgical.
Facial plastic surgery is performed by ENT surgeons, maxillofacial surgeons, general and plastic surgeons, oculoplastic surgeons and dermatologists.
Septorhinoplasty
Nasal anatomy
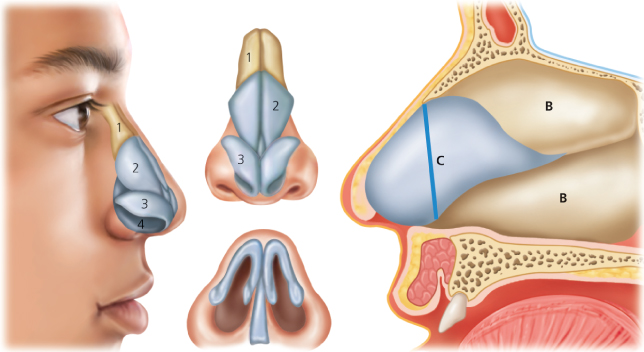
The skeleton of the nose is formed in the upper third by of the paired nasal bones and ascending processes of maxilla. The mid third of the nose is formed by the upper lateral cartilages which attach to the nasal bones and to the cartilaginous septum and contribute to the internal valve. The lower lateral cartilages give support and shape to the nasal tip and external valve. Underlying and supporting these cartilages is the anterior cartilaginous part of the nasal septum, without which the caudal two-thirds of the nose would collapse (Figure 15.1). The type and thickness of the skin soft-tissue envelope contributes to nasal aesthetics and may influence the results of functional and aesthetic surgery.
Figure 15.1 Left: Anatomy of the external nasal skeleton: 1, nasal bones; 2, upper lateral cartilages; 3, lower lateral cartilages; 4, septum (inside the nose). Right: Anatomy of the nasal septum: B, bone; C, cartilage, with the line of nasal support between keystone area superiorly and anterior nasal spine inferiorly shown in blue.
(Copyrighted to The Nose Clinic.)
Nasal function
The nasal valves
During inspiration the nasal valves are subject to collapsing forces due to the low pressure of the rapidly moving inspired air. The ability of the nares and external valve to withstand these collapsing forces depends upon the shape, resilience and position of the nasal tip cartilages. The internal valve normally measures approximately 10–15° and is measured between the septum medially and the caudal border of the upper lateral cartilage laterally. Surgery may require repositioning of these cartilages and grafting to strengthen and support them.
The septum and keystone area
The nasal septum is composed of the quadrilateral cartilage anteriorly, and the bony ethmoid plate, vomer and maxillary crest posteriorly and inferiorly. A deviation in the anterior and dorsal septal cartilage is a difficult surgical challenge as correction may require repositioning, reshaping and reconstruction of the entire cartilaginous septum and its associated upper lateral cartilages (Figure 15.2).
Figure 15.2 Preoperative (left) and postoperative (right) views of a patient with a twisted nose presenting with nasal obstruction due to combined deformity of the nasal bones, upper lateral cartilages and anterior septum. Relief of obstruction in this case requires septorhinoplasty.
(Copyrighted to J Rowe-Jones.)

Assessment
The patency of the nasal airway and the aesthetic appearance of the nose should be considered in all patients even though the presenting complaint may relate more to one of these than the other. This is because an operation to correct an aesthetic anomaly may affect the architecture of the nasal valves, and an operation to alleviate nasal obstruction may necessitate alteration to the nasal bones, upper and/or lower lateral cartilages, and hence the appearance of the nose (Table 15.1).
Table 15.1 Septorhinoplasty: indications and contraindications.
| Indications | Contraindications |
| Acute saddle nose following trauma | Pre-primary school age |
| Functional: combined nasal and septal deformity causing obstruction | Severe co-morbid conditions Major psychiatric illness or personality disorder |
| Aesthetic |
Important features to note at consultation are given in Box 15.1.
Nasal skeleton
- Assess the upper (bony) third, middle (cartilaginous) third and lower third (tip) of the nose for deformity
- Examine the nose from frontal, lateral, oblique and basal views (Figure 15.3)
Nasal valves
- Dimensions of internal and external valves
- Narrowing of the valve areas with inspiration
Nasal septum
- Malposition of the dorsal and caudal leading edges
- Twists, curves or other abnormalities of shape
Psychological
- Determine the primary concern of the patient and their expectations
- Exclude major psychological illness, body dysmorphia, and significant personality disorder
Figure 15.3 Pre-operative (above) and postoperative (below) views of a patient seeking cosmetic septorhinoplasty to correct her dorsal hump and her nasal tip. She has an asymmetric face with a nasal twist. Open approach enabled dorsal reduction, tip refinement and straightening of the nose.
(Copyrighted to J Rowe-Jones.)

Postoperative care and complications
- An external splint is required for 1 week postoperation.
- The appearance of a haematoma of the septum or external nose requires surgical review. An untreated haematoma may lead to collapse of the nose.
- Cutaneous infections may lead to visible scarring and contracture and need aggressive treatment and review.
- Secondary haemorrhage can occur up to 2 weeks after surgery
- Healing is protracted and patients often require support during this time. The final outcome of surgery may not be evident for 12 months or more.
Pinnaplasty
Prominent or “bat ears” can result in merciless teasing, which affects approximately 15% of the population and correction of this problem is very commonplace! The ideal age at which to undertake a pinnaplasty is preschool as the cartilage is still soft, allowing for easy remodelling.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


