OVERVIEW
- Facial weakness or paralysis must always be investigated
- Important causes to exclude are:
- Middle ear disease: urgent treatment is necessary
- Parotid malignancy
- Middle ear disease: urgent treatment is necessary
- Idiopathic or ‘Bell’s palsy’ is the most common diagnosis but this can be suggested only when any other causes have been excluded
- The most effective treatment for Bell’s palsy is corticosteroids in the first 72 hours. Current evidence suggests that other treatments are ineffective
- Patients with herpes zoster oticus present with severe pain as well as facial weakness
- Other causes of facial palsy are uncommon but must be considered if the palsy progresses or does not improve
Definition
A facial palsy is weakness of the muscles of facial expression, from disease of the VIIth cranial nerve, or from disease in adjacent structures.
Anatomy
The facial nerve leaves the facial nucleus, in the brainstem, and passes through the internal auditory meatus beside the VIIIth cranial nerve. After the geniculate ganglion, it runs horizontally across the middle ear in the fallopian canal, just above the oval window, then turns vertically downward, where it supplies the stapedius muscle before leaving the temporal bone through the stylomastoid foramen. It enters the parotid gland where it divides into five main branches distributed to the muscles of facial expression. In the middle ear it also contains secretomotor fibres to the submandibular and sublingual salivary glands and taste fibres from the anterior two-thirds of the tongue, via the chorda tympani.
Presentation
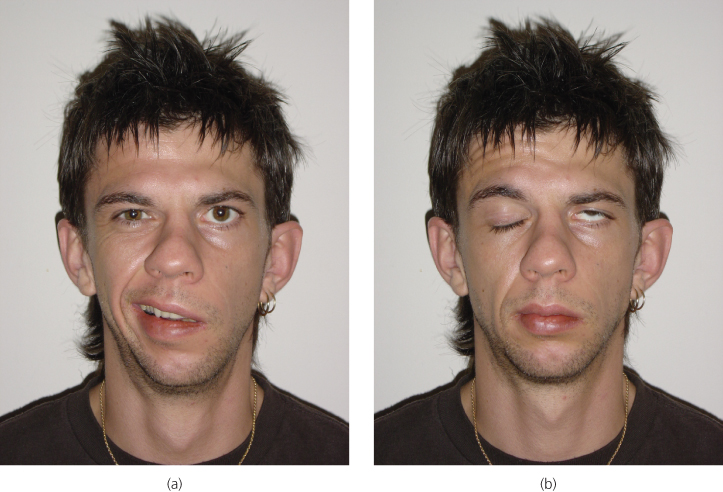
Patients present with weakness of the muscles of facial expression (Figure 9.1). The affected side of the face droops and they may be unable to close their eye. They may complain of hyperacusis due to paralysis of the stapedius muscle in the midde ear. In severe cases, there may be a metallic taste due to a change of taste sensation on one side of the tongue. Reduced lacrimation causes dryness of the affected eye. Poor mouth closure can cause drooling and difficulty with eating.
Figure 9.1 A left-sided lower motor neurone facial nerve palsy: (a) note generalized muscle weakness of left side of the face—forehead, cheek and mouth; (b) a positive Bell’s phenomenon when attempting to close the left eye.
The great majority of facial palsies are from lower motor neurone lesions. Upper motor neurone lesions arise from disease, such as strokes, in the brain. In upper motor neurone lesions, the patient can still move the upper part of the face (i.e. the forehead), because of crossover pathways in the brainstem, but the distinction may be difficult.
Clinical testing can sometimes help to localise the area of damage to the nerve. Schirmer’s test can be used to test lacrimation. A small strip of filter paper is hung from the lower eyelids and the flow of fluid compared. Normal lacrimation would suggest that the lesion is distal to the geniculate ganglion. Testing taste sensation on the anterior two-thirds of the tongue would indicate whether the chorda tympani was affected. The stapedius reflex can be measured. These tests are of limited value as they have poor correlation with the site of damage, and have been superseded by MRI when localisation is required.
Aetiology
Most facial palsies (nearly 75%) are of unknown origin (i.e. idiopathic), so-called ‘Bell’s palsy’. Aetiologies are listed in Table 9.1.
Table 9.1 Aetiologies of facial palsy.
| Lower motor neurone facial palsy | |
| Idiopathic | Bell’s palsy |
| Infection | Acute otitis media Chronic otitis media, especially cholesteatoma Herpes zoster (Ramsay Hunt Syndrome) Lyme disease |
| Neoplasm | Malignant parotid neoplasms Middle ear carcinoma Facial neuroma |
| Trauma | |
| Other | Sarcoidosis Wegener’s granulomatosis Multiple sclerosis Melkersson–Rosenthal syndrome |
| Upper motor neurone facial palsy | |
| CVAs | |
| Intracranial tumours |
Bell’s palsy
Bell’s palsy is an idiopathic, lower motor neurone facial palsy. The onset is over a few hours, commonly arising overnight. Patients often complain of an aching pain around the ear, often preceding the onset of the palsy. Severe otalgia suggests herpes zoster (see below). Patients may also complain of facial numbness, hyperacusis and altered taste. There is an annual incidence of 20–30 cases per 100 000 of the population. Individuals can be affected at any age, but young and middle-aged adults are the most likely to be affected. Pregnant women and individuals with diabetes are thought to be at greater risk.
Aetiology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


