Chapter 30 Facial Nerve Tumors
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
Tumors of the facial nerve are rare causes of facial paralysis.1–5 The two most common tumors are facial nerve neuromas, which are intrinsic to the nerve, and facial nerve hemangiomas, which are extraneural in origin. This chapter focuses on these two types of facial nerve tumors. The techniques discussed can also be applied to other facial nerve neoplasms.
Because of their subtle presentation, facial nerve tumors may be difficult to diagnose and require a high degree of clinical suspicion.6,7 The presenting symptoms vary with the tumor location, size, and histology. Facial nerve neuromas that arise in the internal auditory canal (IAC) and cerebellopontine angle may manifest with a progressive sensorineural hearing loss similar to that caused by an acoustic tumor,8 and the true diagnosis may be established only at surgery.9,10 In a patient with a suspected acoustic tumor, the presence of coexisting facial nerve symptoms (rare with acoustic tumors) should warn the surgeon that a facial nerve tumor may be present.11,12
Facial nerve neuromas usually do not cause symptoms until they are fairly large and may manifest initially with hearing symptoms.12–14 Tumors arising in the middle ear may contact the ossicles and cause conductive hearing loss.15 In such cases, when a mass behind the tympanic membrane is invisible, the patient may be thought to have otosclerosis, and the correct diagnosis is made during tympanotomy for stapedectomy.6 When a middle ear mass is encountered in such a situation, a biopsy must not be done because a facial nerve paralysis is likely to develop postoperatively (see section on pitfalls of surgery).1,6,13,16,17
If the tumor erodes into the labyrinth (typically, the lateral semicircular canal at the external genu), the patient may present with dizziness.3 On examination, the fistula test result may be positive.
Facial nerve hemangiomas characteristically cause severe symptoms when very small.18,19 Similar to facial nerve neuromas, hemangiomas can occur in the IAC and manifest as acoustic tumors.20 They usually cause a sensorineural hearing loss that is severe for the size of the tumor. Extremely small hemangiomas of the geniculate ganglion can cause profound facial nerve symptoms.21–23 Hemangiomas are extraneural and cause paralysis by compression,24 but the small size of the tumor can make diagnosis by imaging studies very difficult. A high degree of clinical awareness is required.25
Patients with either tumor type may present with facial nerve symptoms. Typically, these patients have recurrent Bell’s palsy, although the facial nerve recovery is less complete with each episode.14 Facial nerve twitching can be present in some patients, and others may have facial paralysis with no recovery or a slowly progressive facial paralysis.26,27 When evaluating a patient with atypical facial nerve symptoms, one must always suspect facial nerve tumor.
Electric testing can help establish the diagnosis of a facial nerve tumor. Electroneuronographic results may be abnormal in patients with facial nerve tumors, even in the face of clinically normal function. Facial electromyography may show a pattern of simultaneous denervation and reinnervation in patients with tumors.18 This pattern is seen in slowly progressive, pathologic processes, and would not be expected with a rapid insult to the facial nerve, such as seen in Bell’s palsy.
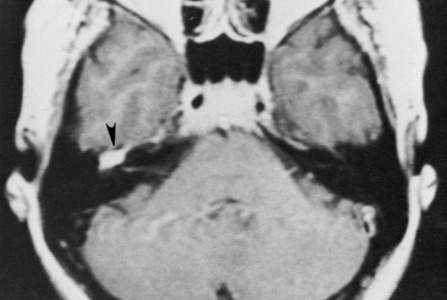
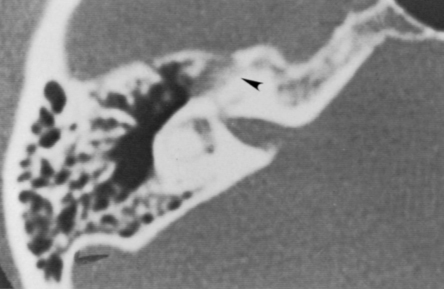
High-resolution magnetic resonance imaging (MRI) with gadolinium may be sufficient to detect most facial nerve tumors (Fig. 30-1). Imaging of a facial nerve neuroma generally reveals a mass lesion and enlargement of the fallopian canal. Small facial hemangiomas at the geniculate ganglion may require high-resolution computed tomography (CT) (Fig. 30-2). These tumors exhibit characteristic bony changes, termed honeycomb bone.28 The medial extent of tumors arising at the geniculate ganglion can be assessed best with gadolinium-enhanced MRI.29 This medial extension has important ramifications regarding selection of surgical approach.
PATIENT SELECTION
The timing of surgery is perhaps the most difficult aspect of planning. Many patients with facial nerve tumors have normal or nearly normal facial function. The best anticipated facial function after a facial nerve graft is a House-Brackmann grade III to IV.16 Waiting too long to remove the tumor can adversely affect the ultimate facial nerve results, however. Patients with a long-standing facial nerve paralysis have worse results after facial nerve grafting than patients who have grafting when they have normal facial function.9,13 Extraneural tumors, such as facial nerve hemangiomas, can be removed with preservation of facial nerve continuity; early surgery in such cases may offer the best hope for excellent facial nerve function. Labyrinthine fistula can develop from bony erosion by the tumor and can lead to deafness and dizziness if the tumor is neglected too long.13,30
For an older patient in poor health who has a small tumor and good facial function, observation may be the best strategy. Younger patients with good facial function may also be followed, but they must be aware of the possible risk to the ultimate facial nerve outcome and to their hearing if surgery is delayed.12 In some cases, we follow patients until they show greater than 50% denervation by electroneuronography. When they reach this degree of denervation, we are concerned that facial nerve grafting after further loss of neural “firepower” would ultimately result in poor facial function.
Another option is planned surgical decompression to reduce pressure on nerve fascicles.31 This is an option for selected patients with small tumors for whom a facial palsy is an unacceptable outcome because it can give them several more years of normal facial function.32 When the tumor becomes neurosurgically significant, it is then resected. Decompression can be accomplished through the middle fossa or translabyrinthine approach, depending on the segments of the facial nerve that are involved.
Facial nerve neuromas in the IAC may be recognized during surgery for what was presumed to be an acoustic tumor.33 Tumor in the labyrinthine fallopian canal and the course of the facial nerve over the posterior aspect of an “acoustic tumor” are clues to the existence of a facial nerve neuroma. Preoperatively, we counsel patients with acoustic tumors about this unlikely possibility. When a facial neuroma is diagnosed intraoperatively, the options are to resect the tumor and place a nerve graft, and decompress the tumor. In some cases, the diagnosis of a facial nerve tumor is not made before the continuity of the facial nerve has been lost.
Radiation Therapy and Radiosurgery
Stereotactic radiotherapy and radiosurgery has been performed on several facial neuromas.34 Reports are anecdotal, and the outcome of this therapy for facial nerve tumors is completely unknown. Because this technique is investigational, treatment of facial tumors with radiosurgery should be performed only as part of an institutional review board–approved protocol. A case of malignant transformation after radiosurgery has been reported.35 This patient had partial excision of a facial nerve neuroma with postoperative radiation. Ten years later, the patient developed the cancer and had a poor outcome.
Patient Counseling
To describe a “good” result after facial nerve grafting, I tell my patients that they will look normal at rest and have active voluntary movement, but it will not be entirely symmetric motion. This asymmetry will be to the extent that family members will notice a difference, but a stranger on the street would not likely turn and stare (Fig. 30-3).
FIGURE 30-3 Patient postoperatively exhibiting House-Brackmann facial function grade IV 1 year after facial nerve graft.
Patients with a preoperative facial nerve palsy are told to expect worse postoperative facial function after nerve grafting. The longer the duration or the greater the severity of the preoperative palsy, the worse the ultimate result. The other potential risks and complications of surgery are also discussed according to the surgical approach needed. For middle fossa and translabyrinthine cases, the risks are similar to risks for patients with acoustic tumors treated through these approaches (see Chapters 48 and 49).
SURGICAL TECHNIQUES
Preoperative preparation, patient positioning, and instrumentation are as described in Chapter 1. For patients needing a facial nerve graft, the upper neck is also prepared for harvesting of the greater auricular nerve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


