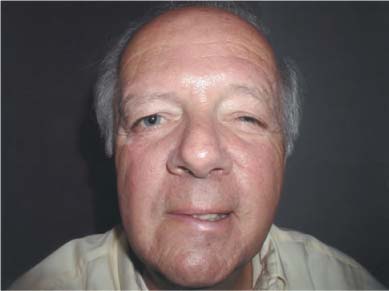
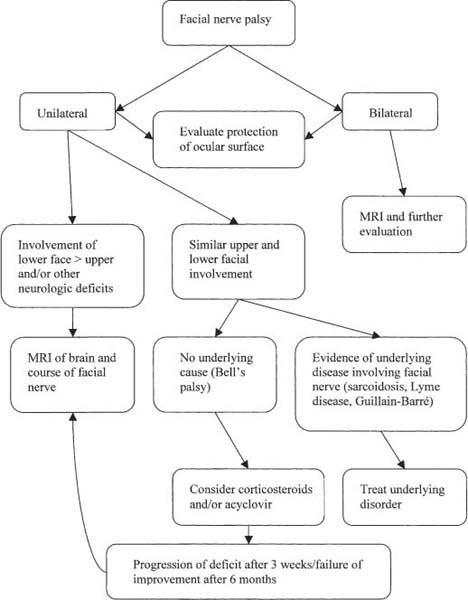
Chapter 42 Involvement of the facial nerve is common in neuroophthalmic disorders, and may result from focal involvement of the peripheral portion of the seventh cranial nerve (CNVII) or represent a manifestation of central nervous system disease. Assessment of patients with facial nerve dysfunction should focus on involvement of other contiguous cranial nerves, and ocular examination should be performed to detect coexistent pathology of the anterior segment. Because facial nerve paralysis may be a manifestation of central nervous system disease, even patients with presumed isolated facial nerve involvement should be evaluated within 24 hours after the onset of symptoms. Although trauma, infection, and inflammation of CNVII may occur, by far the most common cause of peripheral facial nerve paresis is idiopathic or Bell’s palsy. The incidence of Bell’s palsy appears to increase with age and has been reported to be between 15 to 40 cases per 100,000. A viral prodrome is reported by many patients with Bell’s palsy, followed by an acute, unilateral facial nerve palsy. Facial droop may be accompanied by tearing, ocular surface irritation due to exposure, and mild facial pain. Occasionally there is hyperacusis, if the nerve to the stapedius muscle is affected, or impairment of taste of the anterior two thirds of the tongue, if there is involvement of the chorda tympani. Lesions of the facial nerve usually result in motor dysfunction only. Peripheral facial nerve palsy results in paresis of the musculature of the upper and lower face, impairing both voluntary and involuntary facial motor activity (Fig. 42–1). There may be flattening of the ipsilateral nasolabial fold, drooping of the inferior eyelid with widening of the palpebral fissure, loss of the efferent portion of the corneal blink reflex, and impairment of eyelid closure. There may be evidence of corneal exposure and keratitis due to impaired lid closure. Congenital bilateral facial nerve paralysis is characteristic of the Mobius syndrome, in which there is abnormal development of the facial nerve and nucleus. Associations include abduction deficits and abnormal development of the musculature of the chest wall. Patients with the Mobius syndrome are occasionally mistakenly thought to be depressed or have other psychiatric illnesses because of the facial diplegia and resulting lack of facial expression. Patients with the Marcus Gunn jaw-winking phenomenon often present with blepharoptosis (ptosis), which resolves or causes eyelid retraction with opening of the mandible (Fig. 42–2). Miswiring of the eyelid protractors is believed to result in synkinesis with the lateral pterygoid muscles such that when the patient opens the mouth, aberrant fibers from the fifth nerve fire and elevate the upper eyelid. There may be other associated ocular motility deficits. Facial palsy in young patients is most commonly traumatic and is more commonly associated with an underlying cause than that seen in adults. Because facial nerve involvement in young patients is often associated with other developmental defects, extensive surgical intervention with facial reanimation may be required. FIGURE 42–1 Bell’s palsy showing impairment of eyelid closure on the right due to weakness of the orbicularis oculi and weakness of the muscles of the lower face on the right side. Bell’s palsy may progress within the first 2 weeks, but is generally maximal at the onset of symptoms, and progression of the deficit after 3 weeks should suggest another cause of CNVII palsy. The presence of other cranial neuropathies, particularly adjacent nerves such as trigeminal and abducens, should prompt neuroimaging of the brainstem and skull base (Fig. 42–3). In addition, the assessment of patients with facial nerve palsy should focus on underlying systemic disorders during the neuroophthalmic history. Assessment of the function of the musculature of the upper face may help differentiate a central from a peripheral lesion, with sparing of upper face involvement suggesting central involvement and prompting neuroimaging, best accomplished with magnetic resonance imaging (MRI). Bilateral facial nerve palsy portends a more ominous prognosis and should prompt further investigation, including neuroimaging. In a series of 43 patients with bilateral facial palsy described by Keane,1 nine patients had tumors and five patients had an infectious cause. Fifty percent of these patients had a benign, self-limited cause of facial paralysis. Recurrent facial palsy may occur in 10% of patients with Bell’s palsy. Recurrent facial nerve palsy in association with facial swelling is characteristic of the Melkersson-Rosenthal syndrome. There may be associated swelling of the mucosal surfaces and furrowing of the tongue. An association with angioneurotic edema has been suggested and some patients respond to treatment with clofazamine. FIGURE 42–2 A: Patient with Marcus Gunn jaw-winking phenomenon showing slight blepharoptosis on the right and B: eyelid retraction with opening of the mandible (left). FIGURE 42–3 The evaluation of a patient with facial nerve paralysis. Patients with premotor cortical dysfunction, most commonly from cerebrovascular disease, may have unilateral or bilateral impairment of voluntary eyelid closure, while involuntary eyelid closure is generally maintained. Because of the dual innervation to the muscles of the upper face and forehead, impairment of the muscles of the lower face that is out of proportion to that of the upper face suggests facial nerve dysfunction of a supranuclear etiology. In addition to producing other cortical neurologic signs, supranuclear lesions resulting in facial palsy preserve taste to the anterior two thirds of the tongue and lacrimation, and do not cause hyperacusis. Disorders of the basal ganglia, such as Parkinson’s disease (“masked facies”) are characterized by decreased facial motor activity with retention of volitional movement. Similar findings are seen in association with impairment of vertical gaze in patients with progressive supranuclear palsy. Brainstem lesions resulting in complete facial nerve paralysis, most commonly from stroke and demyelination, are usually associated with other neurologic findings, including sixth nerve paresis, horizontal gaze paresis, ataxia, hemiparesis, and vestibuloauditory dysfunction. The Millard-Gubler syndrome, consisting of facial palsy, contralateral hemiparesis, and ipsilateral abduction deficit, is a characteristic brainstem syndrome. Facial nerve paresis may rarely be the first finding in patients with cerebellopontine angle (CPA) tumors, most commonly from an acoustic neuroma. Tumors of the CPA may also involve the ipsilateral fifth, sixth, and eighth nerve in addition to CNVII. Involvement of CNVII may represent the manifestation of a systemic disorder. Viral infection with herpes simplex and varicella zoster (Ramsay Hunt syndrome) have been well described. Lyme disease, syphilis, human immunodeficiency virus infection, tuberculosis, and sarcoidosis have been reported to cause facial nerve paresis with other signs of neurologic dysfunction or in isolation. Facial nerve paresis may also occur as part of a “mononeuritis multiplex” from diabetes mellitus or vasculitis. Involvement of the facial nerve in the ascending weakness of Guillain-Barré syndrome (GBS) and as a feature of multiple sclerosis have been described. Decreased tone of the orbicularis oculi is seen in myasthenia gravis and various myopathies (see Chapter 34) and may masquerade as facial nerve paresis.
FACIAL NERVE DISORDERS
FACIAL NERVE PARALYSIS
URGENCY OF EVALUATION
DIAGNOSIS
Demographics
Symptoms
Signs
Red Flags
 Congenital facial nerve dysfunction and facial palsy in the young
Congenital facial nerve dysfunction and facial palsy in the young
 Progression of the facial palsy
Progression of the facial palsy
 The presence of other neurologic deficits
The presence of other neurologic deficits
 Sparing of the upper face
Sparing of the upper face
 Bilateral facial nerve palsy
Bilateral facial nerve palsy
 Recurrent facial palsy
Recurrent facial palsy

Differential Diagnosis
Facial paralysis secondary to cerebral disease
Facial paralysis secondary to basal ganglia disease
Facial paralysis secondary to brainstem disease
Facial palsy due to a systemic disorder
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


