Facial Nerve
Eric E. Kraus
Craig H. Smith
EMBRYOLOGY
The facial nerve is formed from elements of the second (hyoid) branchial arch, which supplies its motor and sensory components. The migration of the abducens nucleus rostrally, coupled with the movement of the facial nucleus caudally and laterally, gives rise to the uniquely curved brainstem course of this nerve.1
Much of the complexity of the interconnections between cranial nerves V, VII, IX, and X is a result of the evagination of the second branchial arch during the sixth week of development, which causes it to overlap the lower arches. In addition, the embryonic mesodermal tissue of the second arch enters the skin of the face, splitting the elements of the first branchial arch; the underlying muscles of mastication become separated from the overlying cutaneous sensory distribution.2
ANATOMY
An understanding of the rudiments of facial nerve anatomy is necessary for accurate clinical correlation. This will be discussed in terms of the nerve’s supranuclear, nuclear, and infranuclear segments. The infranuclear segment will be further separated into the motor root and nervus intermedius of Wrisberg.
Supranuclear Segment
Facial movement is a complex operation that involves input from both pyramidal and extrapyramidal areas.3 The extrapyramidal circuits involve the premotor cortex, parietal cortex, temporal cortex, cingulate gyrus, hippocampus, amygdala, hypothalamus, basal ganglia, cerebellum, and midbrain tegmentum. These varied connections help explain the tight association of facial movement with emotions and the limbic circuit, as well as the apparent paradox seen in persons who have lost voluntary control of facial movement yet may laugh normally upon hearing a joke.
The cortical area that subserves volitional facial movement is located in the lower third of the precentral gyrus, with representation of the upper face situated rostral to the lower face. These descending motor fibers unite in the internal capsule, decussate in the pons, and terminate in the facial nucleus, which is located in the lateral tegmentum of the caudal pons.4 Both crossed and uncrossed fibers descend to the upper face, whereas only crossed fibers descend to the lower face (Fig. 1). Ascending sensory fibers traveling in the medial lemniscus synapse in the ventral posterior medial nucleus of the thalamus. Medial lemniscal fibers originate in the nucleus solitarius, the gustatory gray of the spinal tract of nerve V, and the main sensory nucleus of nerve V. Much of the primary sensory information is interpreted by the thalamus, while other information is relayed to the postcentral gyrus of the parietal cortex for more complex sensory interpretation. An extensive number of connections within the brainstem are also made, allowing for a richly diverse pattern of reflexes. Lastly, muscle spindle information probably reaches the cerebellum from the mesencephalic nucleus of nerve V in the caudal midbrain.
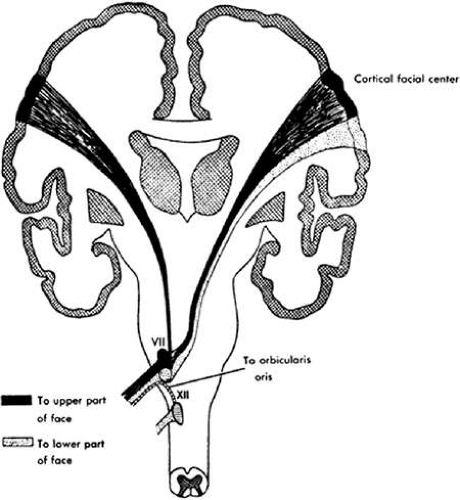 Fig. 1. Pathways for the supranuclear control of facial movement. The upper part of the face is supplied from both hemispheres. Also shown is postulated motor input to the ipsilateral orbicularis oris muscle from the hypoglossal nucleus, a possible explanation for the facial weakness seen in lesions of the lower brainstem. (From Haymaker W: Bing’s Local Diagnosis in Neurologic Diseases, 15th ed. St. Louis: CV Mosby, 1969:230, with permission.) |
Nuclear Segment
The facial motor nucleus extends approximately 3 to 4 mm in length; its caudal portion is an extension of the nucleus ambiguus, and its rostral portion reaches the abducens nucleus dorsomedially and the motor nucleus of nerve V laterally.5 In its rostral extent is found a separate, discrete bunch of large multipolar cells representing the accessory facial nucleus.6 Both nuclei control motor function. Running rostromedially and dorsally, these motor fibers sweep around the abducens nucleus to form the internal genu, which bulges into the fourth ventricle. On its course laterally to exit the brainstem, the nerve passes by the superior salivatory nucleus, where visceral motor fibers destined for the submandibular and sphenopalatine ganglia are picked up by the facial nerve.3,7
Sensory information is transported to the brainstem via small, medium, and large fibers. Each specializes in a different sensory modality, and each synapses on different sensory nuclei in the brainstem or cervical cord. The terminology of the brainstem can be confusing because many of the tracts and nuclei serve many different cranial nerves (see next paragraph). Yet, these structures are often named after the cranial nerve with the largest input (i.e., descending tract of nerve V).
The descending tract of nerve V and associated gray receive small fiber somatic pain and temperature input from cranial nerves V, VII, IX, and X. The solitary tract and nucleus receives small fiber visceral information from the nasal mucosa and anterior two thirds of the tongue, as well as information from nerves IX and X. The main sensory nucleus of nerve V receives medium fiber somatic input for light touch and vibration from both nerves V and VII. Large fiber muscle spindle information is much less clearly defined, but many believe that the mesencephalic nucleus of nerve V receives this input.3,8
Infranuclear Segment: Motor Root
Within the cerebellopontine angle, the somatic motor component of the facial nerve (motor root) is closely approximated to the nervus intermedius and the auditory nerve. Enclosed in a leptomeningeal sheath that contains an extension of the subarachnoid space, the three nerves enter the internal auditory meatus, traveling laterally.9 At the point of entry, the nervus intermedius is between nerve VIII and the motor root. The motor root and nervus intermedius enter the facial canal (aqueduct of Fallopius) within the substance of the temporal bone and then widen to form the geniculate ganglion. It is in the geniculate ganglion where the first parts of the nervus intermedius (see next section) diverge, while other parts continue with the motor nerve (Fig. 2).
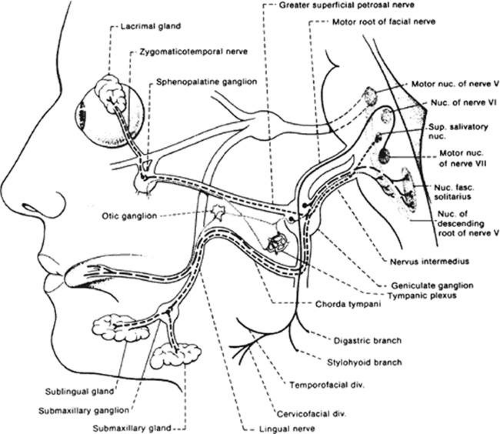 Fig. 2. Course of the facial nerve. Dashed lines represent the autonomic afferent and efferent fibers; the solid lines represent motor input. (From DeJong RN: The Neurologic Exam, 4th ed. Hagerstown: Harper & Row, 1979:181, with permission.) |
The motor nerve then turns posteriorly at a sharp angle, forming the external genu. After the genu, the nerve enters the tympanic (horizontal) portion of the facial canal. This is located below and medial to the horizontal semicircular canal and above the pyramidal eminence that houses the stapedius muscle. The proximal part of this segment is housed behind a fragile, easily fractured tympanic wall; this is a common site of facial nerve damage in traumatic head injuries. Not infrequently, the nerve prolapses into the oval window niche, partly or completely concealing the footplate of the stapes. This anomaly is of clinical importance when the stapes is removed or manipulated during ear surgery.10
At the posterior aspect of the middle ear, the nerve curves downward, at which point a branch innervates the stapedius muscle. This minute muscle acts to dampen wide acoustic input surges from the delicate bony transmission system. The downward course takes it into the anterior wall of the mastoid process of the temporal bone. It is within this segment that the chorda tympani arises and marks the final separation of fibers that form the nervus intermedius. The chorda tympani transmit afferent taste sensation and efferent parasympathetic fibers to the submandibular ganglion (also known as the submaxillary ganglion; see Fig. 2).
The motor nerve continues in the temporal bone until it exits at the base through the stylomastoid foramen. Three branches immediately diverge to innervate the posterior auricular, posterior belly of the digastric, and stylohyoid muscles. It is also in this location that connections are made with nerves IX and X, the auriculotemporal branch of nerve V, and the cervical plexus.
Running anteriorly approximately 2 cm from the stylomastoid foramen the nerve divides into upper and lower divisions, which traverse the superficial portion of the parotid gland (Fig. 3). Pathology of the parotid may impair facial nerve function. Emerging from the parotid gland, the nerve passes over the fascial plane of the masseter muscle, with variable communications between upper and lower divisions. This rich anastomotic network becomes clinically important in cases of aberrant regeneration and in the surgical treatment of synkinetic movements. Eventually the nerve divides further into its five major branches: temporal, zygomatic, buccal, mandibular, and cervical. The distal ends of these branches anastomose with those of the trigeminal nerve; the clinical significance of these communications is open to speculation.11
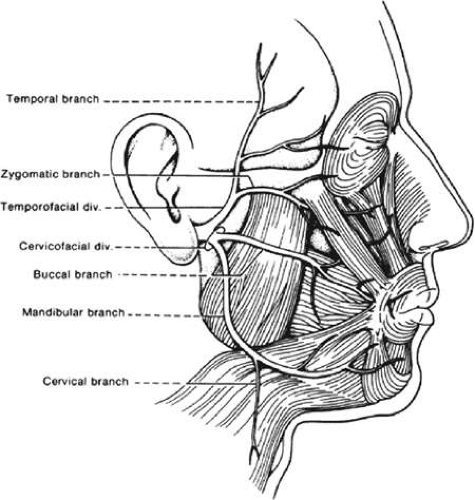 Fig. 3. The distal branches of the facial nerve (motor). (From DeJong RN: The Neurologic Exam, 4th ed. Hagerstown: Harper & Row, 1979:179, with permission.) |
All of the muscles of facial expression are supplied by the facial nerve, with the exception of the levator palpebrae superioris, which is supplied by the oculomotor nerve.
Infranuclear Segment (Nervus Intermedius)
The nervus intermedius of Wrisberg is made up of all the components of the facial nerve except the somatic motor component, as discussed above (Fig. 2). Broadly categorized, information is transmitted for visceral motor function and for visceral and somatic sensation.
The superior salivatory nucleus is the origin of the visceral motor preganglionic parasympathetic nerve destined for both the submandibular and sublingual glands via postganglionic fibers from the submandibular ganglion. These fibers run in the nervus intermedius through the geniculate ganglion, where they follow the somatic motor nerve through the facial canal. Along its downward course within the temporal bone, the preganglionic fibers separate to run with the chorda tympani. The course of the chorda tympani is complicated, running upward and anteriorly over the incus, under the malleus, across the tympanic cavity, and through the petrotympanic fissure to join with the lingual nerve. Finally these parasympathetic fibers reach their destination in the submandibular ganglion.
The lacrimal nucleus, often considered part of the superior salivatory nucleus, is the origin of the visceral motor preganglionic parasympathetic nerve destined for the lacrimal gland via postganglionic fibers from the sphenopalatine ganglion.9 These fibers run in the nervus intermedius, traverse the geniculate ganglion, and form the greater superficial petrosal nerve. On its course, the greater superficial petrosal nerve joins the deep petrosal nerve carrying sympathetic information from the carotid plexus to form the vidian nerve, which ends in the sphenopalatine ganglion. Postganglionic fibers travel with the zygomaticotemporal branch of cranial nerve V to the lacrimal gland.
Visceral sensory fibers may take two routes on their way back to synapse in the nucleus of solitarius. Regardless of the route, their unipolar cell bodies lie in the geniculate ganglion. Taste from the anterior two thirds of the tongue runs with the lingual nerve, chorda tympani, through the facial canal to the geniculate ganglion, and via the nervus intermedius to the brainstem. Sensation from the palate, nose, and pharynx runs with the maxillary nerve to the sphenopalatine ganglion, vidian nerve, greater superficial petrosal nerve to the geniculate ganglion, and via the nervus intermedius to the brainstem.
Somatic sensory fibers from parts of the tympanic membrane, external auditory canal, and periauricular area have their cell bodies in the geniculate ganglion; via the nervus intermedius, they synapse in the nucleus of the descending tract of nerve V and the main sensory nucleus of nerve V.
Microscopic Anatomy
In the segment between the geniculate ganglion and the branch to the stapedius muscle, the facial nerve consists of a single bundle bound by a dense, thick perineural sheath. For the remainder of its course, it lies within a loose rubric of connective tissue.12 It is speculated that this tightly bound portion of the nerve is the pathophysiologic determinant of the degree of facial paresis when there is inflammation of the facial nerve, such as in the mononeuritis of Bell palsy. Any swelling of the nerve fascicles is contained by the perineurium, not by the bony walls surrounding it.10 Therefore, attempts at facial nerve decompression will be best accomplished in this region.
Vascular Supply
The vascular supply of the facial nerve is complex and more fully described elsewhere.12 The posterior vertebrobasilar circulation supplies the proximal and middle portions of the nerve via the anterior inferior cerebellar artery and the internal auditory artery, respectively. Further supply of the middle portion of the nerve comes from the petrosal artery via the middle meningeal artery off the external carotid. Distal segments receive blood from the stylomastoid artery, which is also off the external carotid. The considerable overlap of the arterial supply, especially in the middle portions through the facial canal, make it unlikely that occlusion of any single artery will compromise facial nerve function.12
CLINICAL EVALUATION OF FACIAL NERVE FUNCTION
Motor Function
The majority of facial nerve functions can be readily assessed by observation:
View the patient at rest, during emotionally derived movements, and during volitional facial movements:
With the patient at rest, note the symmetry of the face. Paralysis is associated with drooping of the angle of the mouth and lower lid (Fig. 4). This sagging becomes more apparent as the paresis persists. Mild infranuclear-type weakness may be characterized solely as an asymmetry of blink, an observation that is easily missed if the patient’s face is not examined during the initial history taking.
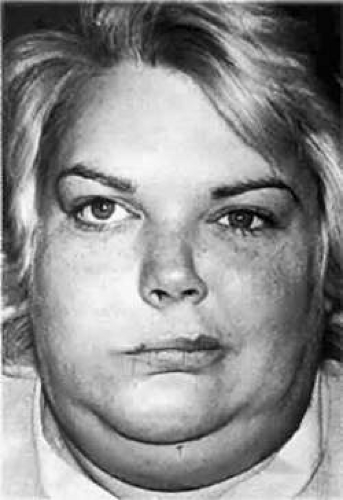
Fig. 4. A 29-year-old woman with a right Bell palsy. Note the right lower lid droop and the leftward displacement of the facial musculature (due to unopposed innervational tone on the left).
The dissociation of emotional and voluntary movements is characteristic of supranuclear lesions; the apparent diplegia of the parkinsonian facies will disappear with volitional movement, and the lower facial weakness caused by a stroke disappears with involuntary smile.3,13
In infranuclear lesions, the patient may complain of hyperacusis from weakness of the stapedius muscle.
Inspect forced closure of the eyes:
Infranuclear lesions usually result in some difficulty in lid closure; in the extreme, there is lack of orbicularis oculi function (lagophthalmos) and upward-rolling eyes (Bell phenomenon; see below), with failure of the covering lid to hide the movements.
Look for involuntary facial movements during volitional movements and with the patient at rest:
The most common involuntary movements during volitional activity are the synkinesias seen following Bell palsy (see “Disorders of Overactivity”).
Unilateral involuntary movements that occur at complete facial rest represent facial myokymia, hemifacial spasm, or seizure, each of which have characteristic features (see “Disorders of Overactivity”).
Sensory Function
Although it is a function of overlapping sensory fibers from the trigeminal, glossopharyngeal, vagus, and greater auricular nerves, abnormal sensation along the posterior aspect of the external auditory canal and tympanic membrane may be an early indication of facial nerve dysfunction.15
Taste is most reliably tested by electrogustometry, which compares the amounts of electrical current applied to the anterolateral aspect of the tongue necessary to produce taste perception. When associated with infranuclear weakness, an increase in the electrical threshold necessary to evoke the perception indicates that the facial nerve lesion is proximal to the origin of the chorda tympani.16 The simple application of salt or sugar to the anterior aspect of the tongue, although unreliable, may give useful information regarding the nerve’s integrity.17
Autonomic Function
Salivary and lacrimal function can be quantified and evaluated through comparison to normal controls as well as to the contralateral side. Examples of tests of these autonomic functions are the salivary flow test and Schirmer’s test of lacrimal function, respectively. This type of testing may be helpful in the prognosis of facial palsy in select patients, thereby helping to direct more extreme measures of therapy.18 In general, however, these tests are difficult to quantitate and impractical for use in general practice.
FACIAL NERVE DISORDERS
Although the facial nerve carries both afferent and efferent information, it is usually the dysfunctional motor component that is brought to the attention of the ophthalmologist. Clinically, dysfunction of the facial nerve can be due to disorders of underactivity or overactivity; these can be further localized anatomically to the supranuclear, nuclear, or infranuclear segments. There are many electrodiagnostic methods capable of evaluating facial nerve disorders, and these are reviewed in detail elsewhere.16
Disorders of Underactivity
Supranuclear Lesions
Motor function of the upper face derives from both hemispheres. As a result, unilateral hemispheric lesions spare the forehead and orbicularis musculature in most cases. However, up to 25% of patients with unilateral disease have objective weakness of the forehead or eye closure.14 This is usually mild, but occasionally can be quite profound. Rarely, infranuclear lesions have been described that spare the forehead, but the accompanying lateralized neurological findings involving the ipsilateral body usually suggest an obvious supranuclear disturbance.10 In addition to the physical examination, computerized tomographic (CT) and magnetic resonance imaging (MRI) scans allow prompt identification of these lesions.
Motor strip or corticobulbar tract lesions are characterized by paresis of volitional movement, with preservation of facial tone and involuntary expressions. These involuntary functions are subserved by extrapyramidal input that originates in the basal ganglia and traverses extrapyramidal pathways to the facial nucleus. When these fibers are damaged in disease states involving the basal ganglia or brainstem (e.g., Parkinson disease), volitional facial movements usually remain normal, whereas little facial tone or emotional expression is displayed.3,13
The list of possible causes of supranuclear facial paresis is large. The major categories of causes are vascular, infectious, demyelinating, and mass lesions.
Nuclear Lesions (Including Those of the Intrapontine Fascicle)
The facial nucleus lies in close proximity to the abducens nucleus and the para-abducens (paramedian) reticular formation. Consequently, patients with nuclear lesions often present with abnormalities of these contiguous structures. However, dissociation between the facial nerve modalities of somatic motor, visceral motor, and sensation can be seen at the level of the pons.
Foville Syndrome
Patients with Foville syndrome display peripheral facial weakness, ipsilateral conjugate horizontal gaze paresis, and contralateral hemiparesis. Lesions associated with these clinical features extend from the facial nucleus to the abducens nucleus and paramedian pontine reticular formation dorsomedially, and into the corticospinal tracts ventrally.19 The paramedian reticular formation can be thought of as the conjugate gaze center of the brainstem, which is why the gaze paresis is conjugate rather than just an ipsilateral abducens palsy.
Millard-Gubler Syndrome
In Millard-Gubler syndrome there is a combination of contralateral hemiparesis, abducens palsy and variable facial nerve palsy.19 Lesions associated with these clinical features lie more ventrally in the brainstem than those of Foville syndrome, and they cause an infranuclear abducens palsy rather than a nuclear disruption. Ipsilateral conjugate gaze paresis, as seen in Foville syndrome, is absent.
Although Foville syndrome and Millard-Gubler syndrome are of historical interest, they represent only signatures of brainstem involvement in which there are varying degrees of nuclear and corticospinal tract dysfunction. Clinically, if a patient has both peripheral facial weakness and eye findings, the presence of a central lesion should be considered and signs of contralateral hemiparesis should be inspected. Stroke, demyelinating disease, and infiltrating tumor are the most common causes; sudden onset suggests the former and either a subacute progression or relapsing-remitting occurrence for the latter two.
Möbius Syndrome
Harlan, writing in 1881, described the first patient with this condition. In 1892, Möbius collated a number of cases, bringing greater recognition to the syndrome that now bears his name. Peripheral facial weakness and abduction deficits are central features of this syndrome, and in the majority of cases these findings are bilateral. A host of associated features have been described, including other cranial nerve palsies, ptosis, musculoskeletal abnormalities, cardiac anomalies, craniofacial defects, and mental retardation.20 Nuclear agenesis of nerves VI and VII is considered the classic syndrome, but investigators have found cases in which the abnormality was nuclear, neuropathic, or myopathic.21,22 Furthermore, the etiologies postulated to date include congenital hypoplasias, vasculopathies, genetics, infections, neuronal degeneration, and muscular dystrophy.23,24,25,26 Imaging studies in nuclear cases, when positive, have shown brainstem atrophy and caudal pontine calcifications. At necropsy, the calcifications in one patient correlated with necrotic areas.27
Surgical treatment of the facial diplegia associated with this syndrome has been occasionally successful; this involves the use of muscle transplants that are innervated by transposition of either cranial nerves V or XII.28
Complications of AIDS
Supranuclear, nuclear, and infranuclear lesions of the facial nerve can also be found in AIDS patients. The meningeal space is a common site of infranuclear involvement with the infectious processes seen in this illness. Depending on the clinical location of disease, CT/MRI, cerebrospinal fluid analysis, and serologic tests are very important ways of differentiating possible causes. Consideration should be given to the presence of toxoplasmosis, lymphoma (intraparenchymal and meningeal), neurosyphilis, tuberculosis, fungus (especially Cryptococcus), and viruses (HIV, cytomegalovirus, and progressive multifocal leukoencephalopathy).
A study by Keane29 found that 50 of 2,030 (2.5%) AIDS patients admitted to the hospital had neuro-ophthalmologic pathology; of these 50 patients, 7 had a peripheral-type facial paresis, all due to lesions of the pontine tegmentum.
Infranuclear Lesions
When facial weakness is progressive and of peripheral nature, lesions along the course of the facial nerve must be considered. By testing the various facial nerve functions, these lesions can be clinically localized, and specific neuroradiological techniques can be used to define further the extent of involvement and suggest a cause. Facial weakness is bilateral in approximately 1% of cases.30
Cerebellopontine Angle Lesions
As noted above, cranial nerves VII and VIII are enclosed in a common sheath as they leave the brainstem in the cerebellopontine angle on their way to the internal auditory canal. Thus, a combination of progressive facial weakness, tinnitus, hearing loss, dizziness, and periorbital dysesthesias (trigeminal nerve involvement) should alert the clinician to a potential mass lesion in this area. Careful evaluation of facial function may also uncover dysfunction of modalities carried by the nervus intermedius.
Tumors of the cerebellopontine angle are generally of a benign histological character. The most common tumors are acoustic neuroma, meningioma, and epidermal cyst. Extra-axial in location, these tumors grow slowly, which is why disequilibrium, rather than true vertigo, is most often reported. The advent of MRI has made evaluation of the cerebellopontine angle simple. Initial workup may also include an audiogram and brainstem auditory evoked potentials.31
Bell Palsy (Idiopathic Facial Palsy)
Since Sir Charles Bell’s classic descriptions of peripheral facial weakness, a voluminous body of literature has developed on the possible etiologies and treatment modalities of the idiopathic variety of facial weakness.17,32,33,34,35,36
Clinical Features. Bell palsy, by far the most common type of facial palsy, is a disease that typically affects adults at any age. Men and women are equally affected. It is characterized by an acute unilateral infranuclear facial nerve paresis (Fig. 4). The maximal weakness is usually reached within 2 to 3 weeks, with a majority of patients maximally affected by 2 to 5 days. In 50% of patients there will be a complaint of retromastoid pain preceding, or concurrent with, the onset of paresis.35 Many patients complain of either increased or decreased lacrimation; a smaller group of patients report having a subjective feeling of numbness, despite intact sensory testing. A subjective sensation of increased lacrimation is not from increased production,37 as demonstrated by normal Schirmer test results, but rather a laxity of the lower lid prevents normal flow of tears toward the lacrimal duct, with the tears more able to spill over. A subjective feeling of diminished taste or perverted taste (parageusia) on the involved side is reported by 30% of patients.
It is not uncommon to find other cranial nerve signs, such as altered facial sensation, corneal hypoesthesia, or tongue deviation, in a case that is otherwise typical of Bell palsy. Broadly defined, this might not cause alarm if one considers Bell palsy to be a viral disease, and thus capable of causing a mononeuritis multiplex.37 If, however, one uses a more narrow definition, patients with more than just facial nerve involvement probably should be diagnosed as having idiopathic cranial polyneuritis.38
Bell phenomenon, a normal upward deviation of the eye with attempted lid closure, is easily seen when the orbicularis oculi muscles are paralyzed, thereby preventing the normal covering over of this phenomenon.
The cause of Bell palsy is felt most often to be reactivation of herpes simplex virus type 1. Murakami, et. al. found HSV-1 DNA in facial nerve endoneurial fluid of 11/14 patients with Bell palsy using the polymerase chain reaction (PCR), but not in 9 patients with Ramsay-Hunt syndrome or 12 controls.39 It is seen more commonly among diabetics, hypertensives, and pregnant women. Few early pathologic examinations have been done, for obvious reasons. Liston40 examined the facial nerve 1 week after onset and found demyelination, axonal changes, and inflammatory cells consistent with a viral cause. Other investigators have not found a cellular infiltrate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


