Step
Duration
Activity allowed
1
Day 0–20
Activities of daily living
2
Day 21–30
Aerobic activity
3
Day 31–40
Noncontact, sport-specific drills
4
Day 41–on
Full-contact practice and game play may be considereda
Nasal Bone Fractures
Anatomically, the nose is a structure with two nasal passages separated by a midline septum comprised primarily of cartilage. The lower two-thirds of the nose is soft tissue, and the upper third is supported by the nasal bones, which articulate in the midline. Superiorly, these bones are attached to the frontal bone of the face, and laterally, they are attached to the maxilla [17]. Children’s noses are structurally different than adults’ noses, with the former being comprised predominantly of compliant cartilage; consequently, in young children, nasal fractures are uncommon [17]. As the bony anatomy of the adolescent nose more closely resembles that of the adult, the incidence of nasal bone fractures rises.
The history is typically straightforward, with an obvious mechanism such as a ball or blow from another athlete striking the nose either directly or tangentially. As discussed elsewhere, one must always begin an examination with a primary survey emphasizing the ABCs of trauma, ensuring there is an adequate airway, and controlling the possible bleeding. On inspection, there is usually an obvious deformity and, often, associated epistaxis. Palpation of the nose and maxillofacial structures is done to assess crepitus or deformity of the nasal bone. Uncommon findings include evidence of cerebrospinal fluid (CSF) leakage and potential signs and symptoms of concomitant injury, such as diplopia (seen with orbital fractures), mental status changes (seen with intracranial pathology), or malocclusion (seen with other maxillofacial injuries) [18]. If the presence of CSF is suspected, the confirmatory laboratory analysis is the beta-2 transferrin test [19].
Crucial to the examination of a nasal fracture is an internal assessment of the nasal septum to rule out a septal hematoma , a condition which should not be missed. On direct visualization, such hematomas appear as bulging, bluish masses in the nasal septum [11]. Following nasal trauma, with or without a bony fracture, children are especially susceptible to septal hematoma and its complications [6]. The flexible nasal cartilage of youth athletes can buckle under deforming forces, producing a separation between the perichondrium and the cartilage, and a hematoma can form in this potential space [6]. Separated from its overlying nutrition, the septal cartilage can necrose and perforate; eventually, a patient may develop the dreaded complication of a saddle nose deformity [17]. If a septal hematoma is identified, it should be aspirated or incised immediately using local anesthesia [20].
There is a limited role for imaging in such injuries. Despite a lack of sensitivity and specificity of plain films for this condition, X-rays are frequently obtained and rarely alter management (Fig. 13.1). Computerized tomography (CT) scans have much greater sensitivity and specificity, but are not justified in isolated nasal fractures given the associated cost and radiation exposure; CT scans do, however, play a role in the patient who has sustained extensive maxillofacial trauma (Fig. 13.2) [6].

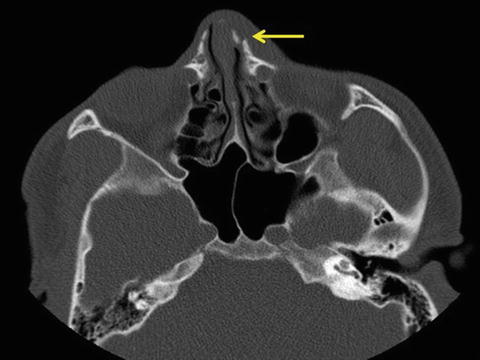
Fig. 13.1
Plain film of nasal fracture in a 16-year-old boy who was punched
Fig. 13.2
CT scan of nasal fracture in a 13-year-old boy injured while playing basketball
Treatment of nasal bone fractures begins with controlling bleeding (see section on epistaxis), treating associated soft tissue injuries, and achieving adequate analgesia. Non-displaced nasal fractures may require no further treatment, whereas significantly displaced fractures typically will undergo closed or open reduction with the goals being realignment of the cartilaginous and bony structures to decrease discomfort and maximize airway patency [20]. In pediatric patients specifically, fractures should be reduced within 3–5 days, as later reduction may be more challenging [17]. Closed reductions are occasionally performed by primary care clinicians as well as specialists; the details of the procedure are beyond the scope of this book [18]. When aesthetic concerns are paramount, either (1) an open reduction or (2) a closed reduction followed by expected rhinoplasty should be chosen [17].
Prompt attention is needed for nasal bone fractures, but with adequate treatment and protection, such injuries do not always require immediate or extended removal from sports. Table 13.2 describes return-to-play conditions for the youth athlete pre- or post-definitive management [11].
Table 13.2
Return-to-play criteria for adolescent athletes with a nasal fracture
1 | Fracture should be closed (no associated laceration) |
2 | Adequate hemostasis has been achieved and a septal hematoma has been ruled out |
3 | The athlete and his/her parents understand the risk for worsening injury and adequate assent/consent have been obtained |
4 | The athlete wants to return to play |
5 | Adequate analgesia has been achieved |
6 | There exist no visual concerns: visual acuity is baseline; visual fields are full; there is no diplopia |
7 | Protective headgear/face mask is recommended |
Mandible Fractures
The mandible has six defined anatomic regions including the symphysis or parasymphyseal region, body, ramus, angle, the coronoid process, and the condyles. Mandible fractures are categorized based on which of these regions are affected. More than 50 % of patients with trauma to the mandible will have fractures in more than one area [21]. Fractures of the condyle are more common in children less than 10 years old, whereas fractures of the symphysis, body, and ramus increase in frequency with age [22].
The history usually involves a forced occlusion : a fall with the chin striking a surface or a blow, from an object or another player, from the lateral or frontolateral direction. After assessing and addressing the ABCs of trauma, physical examination should begin with inspection of the soft tissues. The clinician should note the presence of edema, ecchymosis, hematoma, and lacerations (especially at the chin) and should inspect the oral cavity for the presence of dental injuries/avulsion of the teeth, ecchymosis of the floor of the mouth, lacerations of the mucosa, and integrity of the gingiva. This should be followed by palpation of the entire mandible, intraorally and extraorally, and the temporomandibular joints (TMJ) while the patient opens and closes the mouth to assess the condyles . The examiner should also evaluate occlusion as well as voluntary mandibular mobility, noting deviations on mouth opening and pain and/or difficulty with opening. Sensation should be tested as patients may have numbness of the lip, teeth, and chin (associated with injury to the inferior alveolar nerve) or of the anterior tongue, lip, and cheek mucosa (associated with injury to the lingual or long buccal nerves) [23]. Patients may also present with drooling. Malocclusion may not be obvious on exam; thus, asking a patient about subjective perception of malocclusion may be useful [24]. Patients may be unable to bite down and hold a tongue depressor between their teeth if there is malocclusion [24, 25]. It must be remembered that a force great enough to fracture the mandible is capable of causing injury to other organ systems, and so a thorough secondary examination of the face and body should be done [26].
Diagnosis can be made with plain film radiographs and CTs. Radiographs have been advocated as the study of choice in isolated mandible fractures [23]. Panoramic radiographs are desirable because they provide an excellent image of the entire mandible; however, they are not always available in emergency departments. Panoramic radiographs also require the patient to sit upright in a steady position. If a patient is unable to sit for this study or if it is unavailable, alternate views can be utilized. These include the Towne’s (anterior/posterior projection to look at the condyles) posteroanterior, bilateral oblique, lateral, and submentovertex views [23]. CT with axial and coronal cuts allows for accurate visualization of the injury (Fig. 13.3), and three-dimensional (3D) reconstruction can be valuable for preoperative assessment and surgical planning [8]. CT should be done for patients with significant trauma and suspicion of fractures of other facial bones.
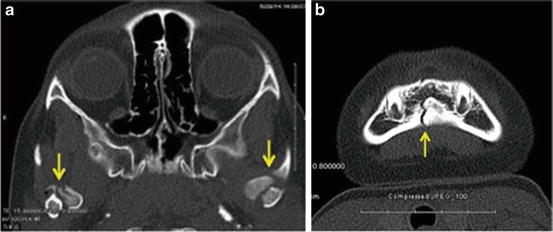
Fig. 13.3
6-year-old female who fell off a bicycle and struck her chin on the ground. (a) CT scan showing bilateral mandible condylar fractures. (b) CT scan showing an additional parasymphyseal fracture
The management of mandible fractures will differ based on multiple variables. These include fracture location, complexity (e.g., displacement, comminution, number of sites), the presence of malocclusion, and the patient’s age and stage of skeletal and dental development [27]. The primary goal of treatment is reestablishment of occlusion. Children with primary or mixed dentition are often treated more conservatively as surgical repair can damage tooth buds and result in maldevelopment of permanent teeth [28]. In adolescent patients, the treatment objective is to establish the best alignment of bony fragments with the least invasive technique [21]. Mandible fractures may be treated with closed reduction and maxillomandibular fixation, which is when the upper and lower jaws are temporarily connected by wires, elastic bands, or metal splints. Fractures with greater degrees of displacement may require surgical correction with open reduction and internal fixation (ORIF) [21]. Adolescents have a greater potential for regeneration and remodeling compared to adults, and so fixation duration may be shorter [26]. Antibiotics that cover oral flora are recommended for open fractures, such as those with intraoral lacerations, disruption of gingiva, or dislodgement of teeth [23].
Nutritional intake must be monitored and optimized during healing as oral intake may be anatomically compromised and poor nutritional status could hinder the healing process [26]. Frequent post operative follow-up is recommended to detect and treat complications such as infection, malocclusion, malunion, or nonunion. Patients must also be monitored for long-term complications such as damage to permanent teeth, growth disturbance, mandibular hypoplasia, neurosensory changes, TMJ dysfunction, and ankylosis in condylar fractures (the inability to open the jaw more than 5 mm) [21, 26, 27]. Return-to-play guidelines in this chapter’s Overview section may be followed.
Orbital Fractures
The orbit is the bony cavity that holds the eyeball and its associated tissues and appendages. Orbital fractures occur with direct blunt trauma to the globe and orbital rim. Fractures of the orbit may involve the bony structures making up the rim or the orbital walls. Orbital fractures may occur as isolated injuries, though they are often associated with more complex fractures including those involving the anterior cranial vault, naso-orbitoethmoid, or zygomatic complex and Le Fort injuries [9, 29]. The orbital rim is composed of three bony regions: frontal, zygomatic, and nasoethmoidal maxillary. The walls that make up the orbital cavity are the superior (or roof), inferior (or floor), medial, and lateral. The orbital floor is the most frequently fractured (Fig. 13.4) [30, 31] followed by the medial wall [9]. Orbital roof fractures occur in younger children who lack frontal sinus pneumatization and have larger craniofacial ratios; these fractures have a higher likelihood of associated neurocranial injuries [29, 32]. Pressure to the orbital rim may fracture just the orbital walls, which is called a “blowout fracture .” Blowout fractures can result in entrapment of one or more soft tissue structures, which limits vertical motility and causes diplopia and enophthalmos (posterior displacement of the globe resulting in a sunken appearance). Blowout fractures with minimal displacement of the bone fragment are more common in the pediatric population [30] and are termed “trapdoor fractures.” These occur when a circular segment of the orbital wall may fracture and become displaced but remain attached on one side. Entrapment of orbital contents can occur in these injuries.

Fig. 13.4
CT scan of an orbital floor fracture in a 16-year-old male struck by a baseball
The typical history includes an object, such as a baseball or elbow , striking the periorbital region. Physical examination should begin with inspection noting ecchymosis, edema, and globe position and then follow with palpation of the periorbital rim. A detailed sensory exam including visual acuity testing should be performed and patients should be asked if they have double vision. Signs and symptoms of orbital fractures can be quite varied, and there can be a range of patient presentations, from asymptomatic with minimal bruising and swelling to diplopia, enophthalmos, hypoglobus (downward globe displacement), and hypoesthesia along the maxillary nerve (numbness of the cheek, upper lip, and upper gingiva) [33]. With 14–40 % of patients reportedly suffering from intraocular complications, patients with orbital fractures must receive a complete ophthalmic evaluation to rule out concurrent ocular injury [31, 34, 35] (see chapter on “Eye Injuries”). The “white-eyed blowout” fracture is a pattern seen in pediatric patients. It was first described in 1998 as an orbital floor fracture that has minimal soft tissue signs of trauma (edema, ecchymosis), lacks enophthalmos, and has minimal evidence of floor disruption on imaging exams, but results in marked motility restrictions in vertical gaze suggesting entrapment of the inferior rectus muscle [36]. Nausea and vomiting have been described as another sign of inferior rectus entrapment with some patients exhibiting the oculocardiac reflex (triad of nausea/vomiting, bradycardia, and syncope) [30, 37]. This injury should be considered in children and adolescents with vertical diplopia, gaze restriction, and nausea/vomiting in the setting of periorbital trauma.
CT with thin-cut high-resolution coronal, axial, and sagittal views of the orbits with 3D reconstructions is the most efficacious imaging modality [29]. Plain radiographs are not recommended as they result in a high number of false negatives and nondiagnostic results [33]. MRI is inferior to CT in the evaluation of these injuries, as MRI provides poor visualization of bone. MRI may be useful if a vascular injury is being considered [38].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


