A perilymph fistula (PLF) is defined as an abnormal connection between the perilymphatic fluid spaces of the inner ear and the air spaces of the middle ear. As a result of the abnormal connection, perilymph fluid may leak and/or ambient pressure changes may be transmitted between the two spaces. Most PLFs occur at or near the oval and/or round windows. Physiologic alterations associated with PLFs result in significant morbidity and disability and profound lifestyle changes. In some cases, PLFs may also result in serious or life-threatening complications, including hearing loss, loss of vestibular function, and meningitis, respectively. The controversy regarding PLF diagnosis arises in part from the adherence to the belief that PLFs are a diagnosis of exclusion. PLFs have been confirmed histopathologically in blinded prospective studies, establishing the pathologic “gold standard” for PLF diagnosis.1, 2 Unfortunately, this standard for pathologic diagnosis cannot be used in the clinical setting for obvious reasons. However, chronic or persistent combinations of dysequilibrium, headache, adult-onset motion sickness (motion-related nausea and vomiting), and neurocognitive disruption, particularly when exacerbated by exertion or physical activity, are classic symptoms of a PLF in one or both ears, until proved otherwise. Contrary to popular belief, only about one-half of traumatic PLF patients have an objective hearing loss. Hearing loss is usually a complication of PLF, not a primary result of otic capsule compromise. Background PLFs were first recognized as a result of pathologic causes, such as tumors or virulent middle ear or mastoid infections. PLFs were later documented as a complication of otic capsule erosion by cholesteatomas, usually at the lateral extent of the horizontal canal.3, 4 Traumatic PLFs have been recognized clinically for more than 100 years.5 PLFs were later identified in military personnel exposed to sudden decompression or blasts and in scuba divers, who presented with sudden hearing loss from round window rupture.6–14 Barotrauma is a well-documented cause of PLFs.13, 15–17 Conditions associated with sudden or dramatic changes in ambient air pressure can rupture the oval or round window via extreme implosive forces.18–20 Certain types of acoustic trauma may also cause PLFs. We have confirmed reports of PLFs in patients exposed to explosions or to sudden or catastrophically loud sound.21 With the advent of stapedectomy, PLFs were implicated as a complication of stapes surgical procedures,22–24 particularly if Gelfoam was used as the graft or if polyethylene tubing was used as a prosthesis.25, 26 In 1971, Goodhill27 advanced the theory of implosive and explosive mechanisms for traumatic PLFs. According to Goodhill, an explosive PLF occurs when a sudden increase in the cerebrospinal fluid (CSF) pressure that ruptures the oval or round window due to increased intracranial pressure is transmitted to the perilymphatic fluid space. An implosive event occurs when sufficient external (ambient) pressures were applied to the tympanic membrane or entered the middle ear through the eustachian tube, driving the stapes into the inner ear and causing rupture of the oval or round window, or both. G.A. Fee, an astute Canadian otolaryngologist,28 was among the first to identify trauma as a cause of PLFs5, 29–35 in patients suspected of having Meniere’s disease. The most likely mechanism of PLFs after blunt body or head trauma is a transient dramatic increase in intracranial pressure, as proposed by Goodhill’s explosive theory.27 The head trauma need not be severe. Whiplash injury has been linked to PLFs.36 Goodhill’s explanations probably account for PLFs occurring in association with whiplash trauma to the neck, and without direct head blow.36 A more recent example of implosive PLF formation is airbag deployment trauma. According to Ferber-Viart et al.,37 airbags may reach peak volume in 50 ms after impact, inflating at a speed of 156 mph, and with an opening force equivalent to a shotgun blast. Traumatic injury to head, neck, upper body, and face in association with airbag deployment has been well documented.38–40 These reports suggest that PLFs from airbag injury are likely to increase. The patient with spontaneous or idiopathic PLF exhibits signs, symptoms, and findings fully consistent with PLFs but that lack correlation to a specific cause.41–45 In reality, spontaneous PLFs probably do not exist per se but are more likely a reflection of the inability to correctly identify a causative event. Anatomic variants have been associated with PLFs,46, 47 including patent fissula ante fenestrae,1, 2, 48, 49 large patent cochlear aqueducts,50, 51 the Mondini deformity,52, 53 and oval window microfissures.2, 54, 55 In some cases, anatomic variants may show familial tendency.56 Congenital PLFs have been described by many clinicians;47, 56–59 in some cases, congenital PLFs appear to have anatomic and/or familial links. Within the modern otologic community, great diversity exists with regard to the identification and management of PLFs. A detailed review is beyond the scope of this chapter. The following discussion summarizes our methods and approaches in dealing with some of the purported controversies associated with the care of the PLF patient. Discussion CLASSIFICATION OF PLFs A myriad of different etiologies for PLFs have been described in the literature. To simplify this discussion, we suggest a global classification of PLF etiology: (1) pathologic (e.g., cholesteatoma, infection/erosion, tumors); (2) traumatic (e.g., acoustic, blast or barotrauma, surgical complication); and (3) spontaneous (idiopathic) (Table 55-1). We have encountered a wide array of interesting causes of PLFs, including PLFs that resulted from prolonged vomiting after exposure to toxic fumes, PLFs in a young weightlifter, PLFs developing during labor and delivery, and PLFs that occurred after a frozen 24-lb turkey fell from a freezer on a patient’s head. In our experience, trauma to the head and neck is by far the most common cause of PLFs. However, our experience is heavily weighted toward trauma patients. There are two level I regional trauma centers in our metropolitan area, one of which is located within our hospital system.
| Pathologic Congenital Cholesteatomas Neoplasms (particularly tumors of the mastoid or skull base) Middle ear infections Mastoid infections Stapedectomy and stapedotomy |
| Traumatic Implosive Barotrauma SCUBA diving Rapid descent in aircraft Acoustic trauma (e.g., exposure to loud noise or explosions) Explosive Explosive Head and neck trauma (including whiplash) Airbag trauma Conditions associated with sudden or sustained increases in intracranial or intrathoracic pressure (e.g., heavy lifting, protracted or violent vomiting, childbirth, obstructive sleep apnea) |
| Spontaneous or unknown causes Anatomic variants? (e.g., persistent aqueduct patentency or congenital defects?) |
CLINICAL PRESENTATION
Our experience confirms the observation by Healy et al.60, 61 that dysequilibrium is the most common presenting symptom of PLF62 (Fig. 55–1). The typical PLF patient has disabling difficulty with gait and imbalance; the patient “cruises,” touching or holding onto walls or furniture, subconsciously attempting to increase proprioceptive input. The PLF patient is constantly spatially disoriented and often is visually dependent. In addition to constant or persistent balance difficulties, physical exertion, especially lifting or straining, will exacerbate or initiate symptoms.
Low-pressure headache, similar or identical to the headache associated with a persistent CSF leak after a spinal tap, is also a primary complaint in patients with active PLFs.62 The typical PLF headache is unilateral and almost always present on the side of the active PLF. In the case of bilateral PLFs, the pain is often worse on the most active side. The PLF headache is severe, sometimes throbbing, and often accompanied by hypersensitivity to light and sound. Headaches persist as long as PLFs are active; when the PLFs are closed surgically or with bed rest, the headaches resolve immediately, similar to the resolution of symptoms after successful blood patching of postspinal tap CSF leaks. Because headache is not a standard part of most otologic questionnaires and interview forms, and many PLF patients have significant short-term memory impairment and are poor or incomplete historians, this important symptom may be missed if not specifically sought.
Adult-onset motion sickness, or exacerbation of previously existing motion sickness, occurs in virtually 100% of PLF patients. Successful closure of PLFs resulted in either immediate improvement in, or cessation of, motion sickness symptoms in 100% of adult PLF patients (n = 31).63 The combined problems associated with motion sickness and with exertional exacerbation of symptoms are extremely disabling to PLF patients, often resulting in loss of mobility, loss of employment, inability to complete normal activities of daily living (ADLs), and even self-imposed reclusive behavior. Often there is comorbid (secondary) psychopathology, including anxiety, depression, and panic-type behavior, especially in undiagnosed patients. These symptoms, and the patient’s attempts to control or avoid them, often lead to misdiagnosis as primary mental or neurologic disorders.
Neurocognitive dysfunction is a well-documented and frequent complaint in patients with PLFs64, 65 (also K.R. Erickson, personal communication, 1989). It is commonly manifested by short-term memory impairment, multitasking problems, difficulties sorting and/or prioritizing tasks and information, and sometimes vague dyslexic disturbances with reading, writing, or difficulty tracking written words. A few patients also have speech difficulties, or dysphasic-mimicking problems with word recall. Cognitive dysfunction increases the patient’s sense of frustration and greatly complicates problems with ADL, schooling, and employment.
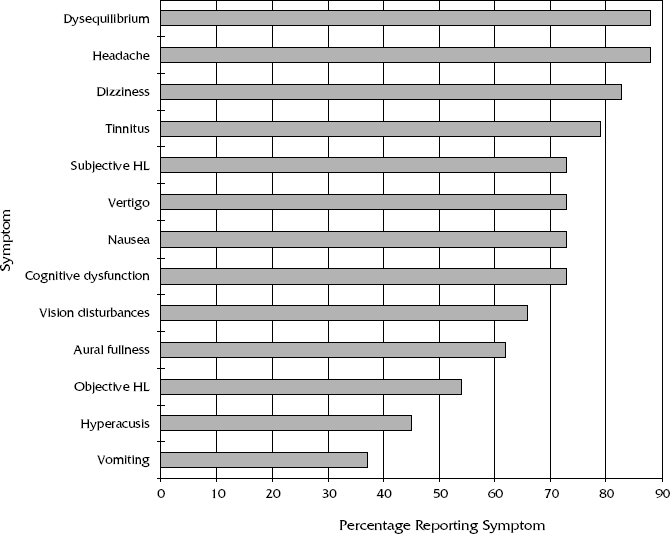
Figure 55-1 Presenting symptoms of perilymphatic fistula.
Hearing loss is not present in all patients with a PLF.66 In our practice, objective hearing loss occurs in about 55% of patients with post-traumatic PLF62 and in about 25% of all patients with PLFs. However, a much higher percentage of PLF patients will complain of subjective hearing loss/fluctuation, or of other auditory symptoms, including tinnitus, aural fullness/pressure, hyperacusis, and aural discomfort. It is obvious that subjective hearing loss and other auditory dysfunction is more common than our ability to document the PLF patient’s consistent complaint of compromised auditory function.67, 68 Objective hearing loss is therefore not an absolute criterion for PLF diagnosis, as is widely believed.
Acute-onset hearing loss in a PLF patient requires emergent care. If the hearing loss does not rapidly improve with restricted physical activity, surgical exploration for identification and PLF closure should be offered the patient.
DIAGNOSIS
The diagnosis of PLF can be established only at tympanotomy. Although imperfect, the clinical gold standard for PLF diagnosis remains visual inspection for perilymph leakage into the middle ear at tympanotomy. Unfortunately, this method is subjective, and two competent surgeons inspecting the same visual field may come to two different conclusions regarding the absence or presence of a perilymph leak. This is especially true if one of the surgeons is viewing the field from a monocular side arm or with any other monocular instrument such as an endoscope.
Even if a clinical fistula test69 – 72 is positive, the results are not diagnostic of PLF because any anatomic or pathologic condition permitting transfer of middle inner ear or intracranial pressure changes to stimulate vestibular receptors will result in a positive fistula test based on external canal pressure changes as the stimulus. Examples include otic capsule softening from lues, Paget’s disease, or labyrinthine fibrosis.73 Conversely, a negative PLF test does not rule out a PLF because external auditory canal pressures may not be transmitted to the inner ear receptors (e.g., with ossicular discontinuities). It is also possible that persons with a loss or absence of vestibular hair cell function in the affected ear will yield negative responses (objective and subjective) to conventional fistula tests. Reduced ability of the vestibular hair cells to respond to stimulation must be considered (established) when interpreting negative fistula test results. Although the only generally accepted way that a PLF can be confirmed is identification of perilymphatic leakage at tympanotomy, failure to observe a PLF leak at tympanotomy does not rule out a PLF because otic capsule integrity can be compromised without perilymph fluid leak.
Standard tests of vestibular and auditory function are normal in patients with uncomplicated PLFs because PLFs do not directly cause loss of auditory and vestibular hair cell function. It is only when complications of persistent PLFs damage receptors that hearing loss and vestibular function deficits occur. Electronystagmography (ENG) may or may not show a positional nystagmus in PLF patients, and caloric and rotation (vestibulo-ocular reflex, or VOR) testing are normal in virtually all uncomplicated PLF patients. Computed dynamic posturography (CDP) often shows abnormal results on sensory organization testing (SOTs); these findings are neither specific for, nor diagnostic of, PLFs. However, the auditory and vestibular functional status of PLF patients should be established by objective tests as early as possible in order to establish a baseline and in order to plan treatment and rehabilitation based on quantitative data.
Hearing loss complicating PLFs does not present a specific pure-tone threshold pattern or configuration, but most are sensorineural in type. Some clinicians have used electrocochleography (ECoG) to assist in the diagnosis of PLFs;74, 75
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


