 Eyelid Sweat Gland Tumors
Eyelid Sweat Gland TumorsEyelid Syringoma
General Considerations
Simple cysts of eccrine or apocrine sweat glands are called eccrine hidrocystoma or apocrine hidrocystoma, respectively (see Chapter 11). Herein, we discuss solid tumors derived from sweat gland epithelium, beginning with syringoma.
Clinical Features
Syringoma can be solitary or multiple. The multiple variant is more common and is often bilateral, symmetric, and most pronounced on the lower eyelid. They are often subtle and hardly noticed by the patient. Multiple syringomas each range from 1 to 3 mm in size and have a yellow-brown color (3,7). Multiple syringomas are usually not associated with other conditions. However, some reports indicate that it is more common in patients with Down’s syndrome (4,11,12), Marfan’s syndrome, and Ehlers-Danlos syndrome (7,12).
Differential Diagnosis
Differential diagnosis includes most of the eyelid lesions discussed in this atlas. Solitary lesions can simulate basal cell carcinoma, sebaceous adenoma, and sebaceous carcinoma. The multiple variety can simulate trichoepithelioma, milium, sarcoidosis, and other conditions (2).
Pathology
Based on histochemical and electron microscopic findings, syringoma represents an adenoma of eccrine ducts (1,3,5). It is composed of cords and nests of solid cells with ducts located within a dense fibrous tissue stroma. The ducts are lined by a double layer of compressed epithelial cells that sometimes assume a comma-shaped or “tadpole” appearance, a feature considered characteristic of this condition (3,7). Numerous cystic dilations of the ducts can result in keratin cysts that can suggest the diagnosis of milium, trichoepithelioma, or squamous cell carcinoma. The keratin cysts can rupture and incite a granulomatous inflammatory reaction (3). Concerning pathogenesis, human papillomavirus types have been detected in solitary eyelid syringoma, suggesting a viral etiology (13).
Management
Management is usually observation. Cosmetics can improve appearance. A larger solitary lesion may require surgical excision to rule out malignancy. Other methods of management include electrodessication and curettage, dermabrasion, and carbon dioxide laser resurfacing (14,15,16,17,18,19). Some authors have advocated combination of carbon dioxide laser and trichloroacetic acid (16). Although solitary syringoma is cytologically benign, it can recur after incomplete excision and exhibit aggressive behavior.
Selected References
1. Hashimoto K, Gross BF, Lever WF. Syringoma. J Invest Dermatol 1966: 46:150-166.
2. Griffith DG, Salasche SJ, Clemons DE. Sweat gland tumors. In: Griffith DG, Salasche SJ, Clemons DE, eds. Cutaneous Abnormalities of the Eyelid and Face. New York: McGraw-Hill; 1987:232.
3. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996: 2296-2300.
4. Kilmer SL. Adnexal tumors. In: Mannis MJ, Masai MS, Huntley AC, eds. Eye and Skin Disease. Philadelphia: Lippincott-Raven; 1996:361-362.
5. Elder D, Elenitsas R, Ragsdale BD. Tumors of the epidermal appendages. In: Elder D, Elenitsas R, Jaworsky C, et al., eds. Lever’s Histopathology of the Skin. Philadelphia: Lippincott-Raven; 1997:778-779.
6. Patrizi A, Neri I, Marzaduri S, et al. Syringoma: a review of twenty-nine cases. Acta Dermatol Venereol 1998;78:460-462.
7. Rodgers IR, Jakobiec FA, Hidayat AA. Eyelid tumors of apocrine, eccrine, and pilar origins. In: Albert DM, Jakobiec FA. Principles and Practice of Ophthalmology. 2nd ed. Philadelphia: WB Saunders; 2000:3414-3415.
8. Older JJ. Eyelid Tumors. Clinical Diagnosis and Surgical Treatment. 2nd ed. New York: Raven Press; 2003:50.
9. Ozdal PC, Callejo SA, Codere F, et al. Benign ocular adnexal tumours of apocrine, eccrine or hair follicle origin. Can J Ophthalmol 2003;38: 357-363.
10. Ostler HB, Maibach HI, Hoke AW, et al. Epidermal skin tumors. In: Ostler HB, Maibach HI, Hoke AW, et al., eds. Diseases of the Skin and the Eye. Philadelphia: Lippincott Williams & Wilkins; 2004:185.
11. Schepis C, Siragusa M, et al. Palpebral syringomas and Down’s syndrome. Dermatology 1994;189:248-250.
12. Urban CD, Cannon JR, Cole RD. Eruptive syringomas in Down’s syndrome. Arch Dermatol 1981;117:374.
13. Assadoullina A, Bialasiewicz AA, de Villiers EM, et al. Detection of HPV-20, HPV-23, and HPV-DL332 in a solitary eyelid syringoma. Am J Ophthalmol 2000;129:99-101.
14. Apfelberg DB, Maser MR, Lash H, et al. Superpulse CO2 laser treatment of facial syringomata. Lasers Surg Med 1987;7:533-537.
15. Wang JI, Roenigk HH Jr. Treatment of multiple facial syringomas with the carbon dioxide (CO2) laser. Dermatol Surg 1999;25:136-139.
16. Kang WH, Kim NS, Kim YB, et al. A new treatment for syringoma. Combination of carbon dioxide laser and trichloroacetic acid. Dermatol Surg 1998;24:1370-1374.
17. Maloney ME. An easy method for removal of syringoma. J Dermatol Surg Oncol 1982;8:973-975.
18. Stevenson TR, Swanson NA. Syringoma: removal by electrodessication and curettage. Ann Plast Surg 1985;15:151-154.
19. Karam P, Benedetto AV. Syringomas: new approach to an old technique. Int J Dermatol 1996;35:219-220.
Eyelid Syringoma
Syringoma can be multiple or solitary. Although syringoma is almost always benign, low-grade malignant behavior can rarely occur.
 Figure 4.1. Subtle, bilateral syringoma involving the lower eyelids in a 70-year-old woman. |
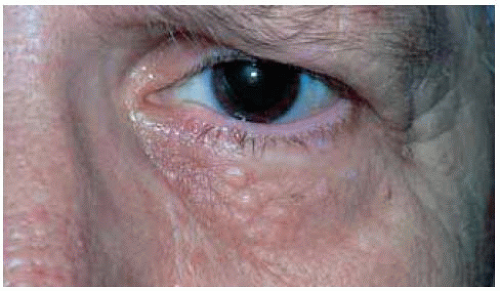 Figure 4.2. Closer view of left eye of patient seen in Figure 4.1, showing elevated tan-colored lesions, similar in color to the adjacent normal skin. |
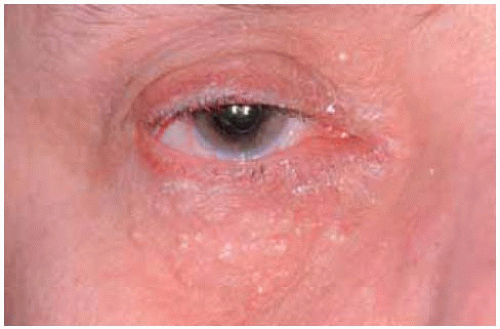 Figure 4.3. Multiple, subtle syringomas on lower eyelid and cheek of a 50-year-old woman. |
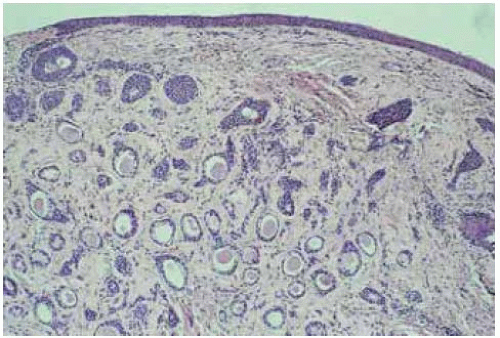 Figure 4.4. Photomicrograph of syringoma showing ducts and tubules of epithelial cells in dense fibrous stroma. (Hematoxylin-eosin 50.) |
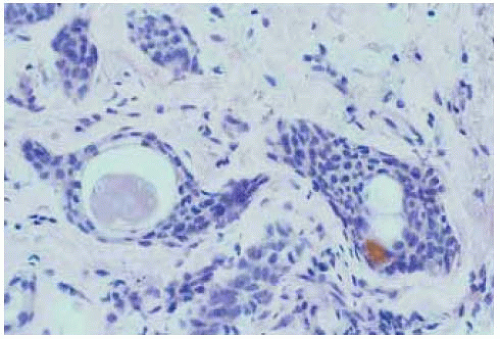 Figure 4.5. Photom icrograph of syringom a showing arrangement of ducts and tubules of epithelial cells, with lightly eosinophilic material in lumen. (Hematoxylin-eosin 200.) |
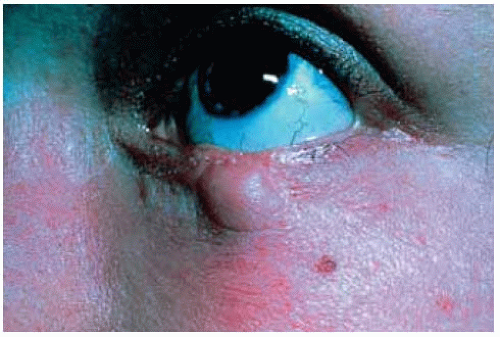 Figure 4.6. Recurrent solitary, larger syringoma of lower eyelid of a 20-year-old woman. Although the original tumor was diagnosed as a benign syringom a, the recurrence showed local invasion, suggesting a low-grade malignancy. (Courtesy of Gordon Klintworth, MD.) |
Eyelid Eccrine Acrospiroma
General Considerations
Eccrine acrospiroma (also called clear cell hydradenoma, eccrine hydradenoma, and porosyringoma) is a tumor that arises from duct and secretory coil of the eccrine sweat gland (1,2,3,4,5,6,7,8,9,10,11,12,13). It is usually solitary and can occur in all parts of the body, with the face and ears being affected in about 10% of cases (1). It can be nodular, solid, or cystic. Although the majority are benign, a malignant variant has been observed (1). The terminology regarding this lesion has been the source of some confusion, but “eccrine acrospiroma” seems to be preferred.
Clinical Features
Eccrine acrospiroma of the eyelid can assume any of a variety of clinical patterns. It is generally a rather rapidly growing solid or cystic lesion that may attain a size of 5 to 30 mm. A smaller lesion may be similar in color to the normal adjacent skin or it may appear as a fleshy subcutaneous mass. A larger eccrine acrospiroma often has blue, crusty appearance and may sometimes become ulcerated. Pain on pressure can be elicited in about 20% of cases (7). The tumor can occasionally show aggressive growth and invade the conjunctiva and orbit (9,11).
Pathology
Histopathologically, eccrine acrospiroma has characteristic features. It is a well-circumscribed lesion deep to the epidermis composed of lobules of epithelial cells that demonstrate a biphasic pattern. One pattern is composed of foci of round to ovoid cells with clear cytoplasm that contain glycogen. The other is composed of closely compact spindle-shaped cells with eosinophilic cytoplasm (1,2,8). In some areas, tumor cells merge with the overlying acanthotic epithelium (8). Enzyme histochemical and electron microscopic studies have established its eccrine gland origin (1,8). Eyelid eccrine acrospiroma has been shown to exhibit oncocytic, apocrine, and sebaceous differentiation, attesting the pluripotentiality of adnexal glandular epithelia (13). Eccrine poroma, a similar tumor that arises from sweat duct epithelium, has been reported on the eyelid (10).
Management
Management is complete surgical excision. The diagnosis is not usually suspected clinically and is made on histopathologic evaluation. The prognosis is excellent.
Selected References
1. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2301-2302.
2. Rodgers IR, Jakobiec FA, Hidayat AA. Eyelid tumors of apocrine, eccrine, and pilar origins. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. Philadelphia: WB Saunders; 1994:1781-1782.
3. Boniuk M, Halpert B. Clear cell hidradenoma of myoepithelioma of the eyelid. Arch Ophthalmol 1964;72:59-63.
4. Ferry AP, Haddad HM. Eccrine acrospiroma (porosyringoma) of the eyelid. Arch Ophthalmol 1970;83:591-593.
5. Grossniklaus HE, Knight SH. Eccrine acrospiroma (clear cell hidradenoma) of the eyelid. Immunohistochemical and ultrastructural features. Ophthalmology 1991;98:347.
6. Johnson BL Jr, Helwig EB. Eccrine acrospiroma. A clinicopathologic study. Cancer 1969;23:641-657.
7. Ostler HB, Maibach HI, Hoke AW, et al. Diseases of the Skin and the Eye. Philadelphia: Lippincott Williams & Wilkins; 2004:184.
8. Elder D, Elenitsas R, Ragsdale BD. Tumors of the epidermal appendages. In: Elder D, Elenitsas R, Jaworsky C, et al., eds. Lever’s Histopathology of the Skin. Philadelphia: Lippincott-Raven; 1997:786-789.
9. Older JJ. Eyelid Tumors. Clinical Diagnosis and Surgical Treatment. 2nd ed. New York: Raven Press; 2003:50.
10. Vu PP, Whitehead KJ, Sullivan TJ. Eccrine poroma of the eyelid. Clin Exp Ophthalmol 2001;29:253-255.
11. Jagannath C, Sandhya CS, Venugopalachari K. Eccrine acrospiroma of eye lid—a case report. Indian J Ophthalmol 1990;38:182.
12. Haneveld GT, Hamburg A. Sweat gland tumour of the eyelid with conjunctival involvement. Ophthalmologica 1979;179:73-76.
13. Buchi ER, Peng Y, Eng AM, et al. Eccrine acrospiroma of the eyelid with oncocytic, apocrine and sebaceous differentiation. Further evidence for pluripotentiality of the adnexal epithelia. Eur J Ophthalmol 1991;1: 187-193.
Eccrine Acrospiroma
Unlike a simple eccrine hidrocystoma, eccrine acrospiroma is a solid tumor clinically, although it can sometimes have a cystic component. It can assume a variety of clinical configurations.
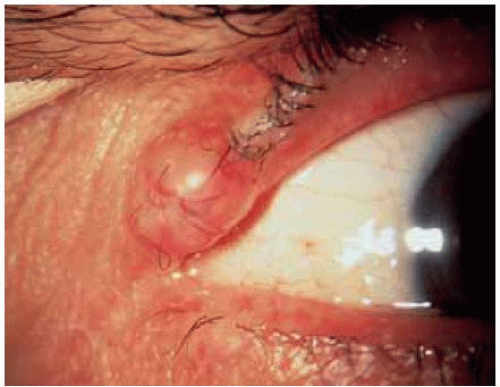 Figure 4.7. Eccrine acrospiroma of upper eyelid of a 75-year-old man. The mass appears as a slightly fleshy nodule deep to the epidermis. |
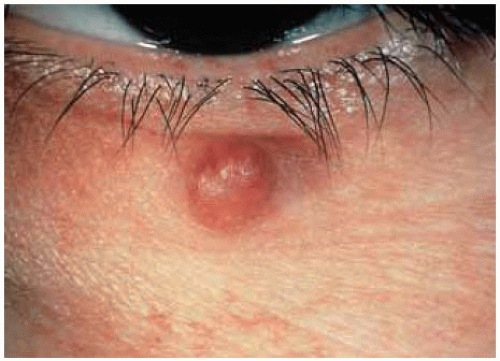 Figure 4.8. Eccrine acrospiroma in lower eyelid. (Courtesy of Ramon Font, MD.) |
 Figure 4.9. Larger, blue-colored eccrine acrospiroma near medial canthus in an elderly person. The lesion had a large cystic component. The smaller solid lesion above is possibly a nevus or papilloma. (Courtesy of Armed Forces Institute of Pathology, Washington, DC). |
 Figure 4.10. Pedunculated eccrine acrospiroma below lower eyelid of a 19-year-old girl. The lesion had been slowly enlarging for 1 year. (Courtesy of Steven Searl, MD.) |
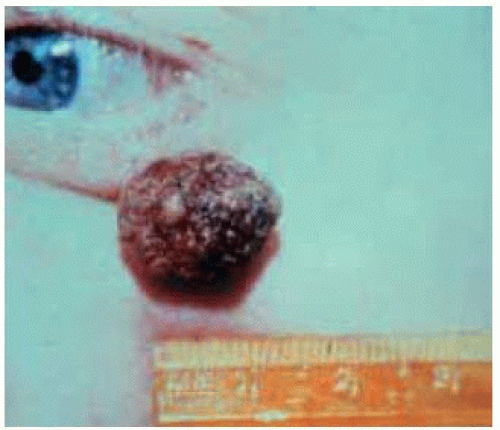 Figure 4.11. Rapidly growing eccrine acrospiroma beneath the lower eyelid of a 46-year-old man. The lesion had grown rapidly over the prior 2 months. (Courtesy of Hans Grossniklaus, MD.) |
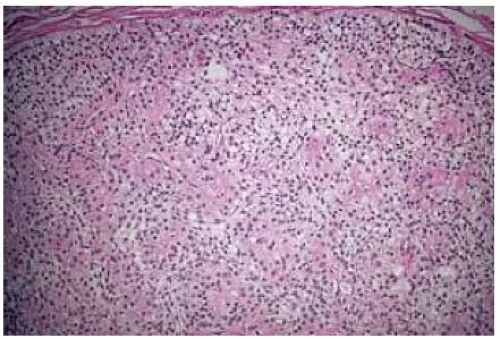 Figure 4.12. Histopathology of eccrine acrospiroma showing biphasic pattern of epithelial cells. Note the interm ixing of spindle cells with eosinophilic cytoplasm and more rounded cells with clear cytoplasm. (Hematoxylin-eosin 75.) |
Eyelid Syringocystadenoma Papillif
General Considerations
Syringocystadenoma papilliferum is an uncommon benign tumor that arises from apocrine glands (1,2,3,4,5,6,7,8,9). It occurs most often on the scalp and temple and only occasionally on the eyelid, where it presumably arises from the apocrine glands of Moll. In one series, it accounted for 2% of ocular adnexal tumors of apocrine, eccrine, or hair follicle origin (9). In about 75% of cases, it arises during puberty within a nevus sebaceous of Jadassohn; thus, it may be a component of the organoid nevus syndrome (10). When it is confined to the eyelid, it is often a solitary lesion that appears in middle age and is not usually associated with nevus sebaceous of Jadassohn (3). It is believed by some authors that syringocystadenoma papilliferum can evolve into basal cell carcinoma and that it may represent a transition phase between nevus sebaceous of Jadassohn and basal cell carcinoma (8).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


