 Eyelid Histiocytic, Myxoi and Fibrous Lesions
Eyelid Histiocytic, Myxoi and Fibrous LesionsEyelid Xanthelasma and Xanthoma
General Considerations
Xanthelasma is an extremely common, benign subcutaneous eyelid lesion that has characteristic clinical and histopathologic features (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26). When it is larger and nodular, assuming tumorous proportions, it is called a xanthoma. Xanthelasma tends to be bilateral and more common in the elderly. It occurs in 1% to 3% of individuals and is slightly more common in women (4). Although some patients with xanthelasma are normolipemic, about 50% of them have essential hyperlipidemia (usually type II) or secondary hyperlipidemia owing to conditions like diabetes mellitus or biliary cirrhosis (1,2,3,4,5,6).
Tuberous xanthoma appears as solitary or multiple, placoid or papular lesions that have a predilection for buttocks, elbows, knees, and fingers. It is more likely to be associated with hyperlipidemia types II and III (1). It may be a result from hyperlipemic genetic defects in lipid metabolism, and is most often transmitted as an autosomal-dominant trait. It consists of one or more elevated nodules that are usually located in the extremities, but can be found on the eyelids (7,8,9,10,11). One case of multiple bilateral eyelid tumors was initially believed to represent fibrous histiocytomas (1), but later the diagnosis was changed to tuberous xanthomas (2). (See Figure 10.10.)
Multiple eruptive xanthomas can sometimes occur in patients who experience a rapid rise in serum triglyceride levels (5). In some cases, these lesions can become very large and aggressive despite being benign, and even invade through the orbital septum into the orbital fat. Interestingly, these large xanthomatous lesions have been known to extensively involve all four eyelids in patients with normal serum lipid levels (8,9,10,11).
Affected patients are believed to be at higher risk of death from cardiovascular disease (4). Xanthelasma is also seen with greater frequency in patients with the Erdheim-Chester disease, an idiopathic condition characterized by lipid deposition in bones, heart, retroperitoneum, and orbit (12,13,14).
Clinical Features
Clinically, xanthelasma appears as one or more, flat or minimally elevated, yellow, placoid lesions that affect the loose skin of the eyelids, more commonly on the medial aspect of the eyelids. It generally occurs in middle-aged or older adults and is more common in women. It is often bilateral and symmetrical, and can sometimes slowly enlarge and coalesce to form large, raised, plaquelike, or nodular lesions. When a xanthelasma becomes elevated and nodular, it is more properly called a tuberous xanthoma (7,8,9,10,11).
Pathology
Microscopically, xanthelasma and xanthoma are forms of lipoma that consist of an infiltration of the superficial reticular dermis by foamy histiocytes. The cells tend to be more concentrated around blood vessels (1,2,3,4,5). Touton giant cells are occasionally present. There is generally an absence of fibrosis.
Management
There are several approaches to management of xanthelasma and xanthoma, depending on the clinical circumstances (15,16,17,18,19,20,21,22,23,24,25,26). Management should include evaluation of the affected patient for various hyperlipidemias and Erdheim-Chester disease. The eyelid lesions can generally be observed. Surgical excision should be considered for larger or cosmetically unacceptable lesions. The wound can be closed with sutures or allowed to heal by secondary intention (16). An intriguing technique has been reported in which the xanthelasma is raised with a skin flap and resected from the back side of the skin and then the skin flap without the tumor is sutured into its original position (19). Others have modified that technique to treat the xanthelasma on the back side of the flap with erbium yttrium aluminum garnet (YAG) laser and then suturing the flap into position (25). Topical application of 35% trichloroacetic acid can also be effective (5). Others have advocated topical 100% bichloracetic acid (18). Very good results have also been obtained by using a carbon dioxide laser to vaporize the lesions (15,21). More recently, the erbium YAG laser has also been reported to be effective (23). The treatment options have recently been reviewed in detail (24). In addition, affected patients should be treated medically for elevated serum lipids. Sometimes such medical treatment alone brings about resolution of xanthelasma (26). The larger, tuberous xanthomas generally require surgical excision.
Selected References
1. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2334-2337.
2. Netland PA, Font RL, Jakobiec FA. Orbital histiocytic disorders. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. Philadelphia: WB Saunders; 1994:2094-2095.
3. Ostler HB, Maibach HI, Hoke AW, et al. In: Diseases of the Skin and the Eye. Philadelphia: Lippincott Williams & Wilkins; 2004:154-155.
4. Habif TP. Cutaneous manifestations of internal disease. In: Clinical Dermatology. 2nd ed. St. Louis: CV Mosby; 1990:648-650.
5. Tucker SM. Xanthomas. In: Mannis MJ, Masai MS, Huntley AC, eds. Eye and Skin Disease. Philadelphia: Lippincott-Raven; 1996:99-103.
6. Pinto X, Ribera M, Fiol C. Dyslipoproteinemia in patients with xanthelasma. Arch Dermatol 1989;125:1281-1282.
7. Shukla Y, Ratnawat PS. Tuberous xanthoma of upper eyelid (a case report). Indian J Ophthalmol 1982;30:3.
8. Rose EH, Vistnes LM. Unilateral invasive xanthelasma palpebrarum. Ophthal Plast Reconstr Surg 1987;3:91-94.
9. Tosti A, Varotti C, Tosti G, et al. Bilateral extensive xanthelasma palpebrarum. Cutis 1988;41:113-114.
10. Depot MJ, Jakobiec FA, Dodick JM, et al. Bilateral and extensive xanthelasma palpebrarum in a young man. Ophthalmology 1984;91:522-527.
11. Ohta M, Suzuki Y, Sawada M. Bilateral tumor-like invasive xanthelasma palpebrarum in the superior palpebra. Ophthal Plast Reconstr Surg 1996;12:196-198.
12. Alper MG, Zimmerman LE, LaPiana FG. Orbital manifestations of Erdheim-Chester disease. Trans Am Ophthalmol Soc 1983;81:64-85.
13. Shields JA, Karcioglu Z, Shields CL, et al. Orbital and eyelid involvement with Erdheim-Chester disease. Arch Ophthalmol 1991;109:850-854.
14. Opie KM, Kaye J, Vinciullo C. Erdheim-Chester disease. Australas J Dermatol 2003;44:194-198.
15. Ullmann Y, Har-Shai Y, Peled IJ. The use of CO2 laser for the treatment of xanthelasma palpebrarum. Ann Plast Surg 1993;31:504-507.
16. Eedy DJ. Treatment of xanthelasma by excision with secondary intention healing. Clin Exp Dermatol 1996;21:273-275.
17. Sampath R, Parmar D, Cree IA, et al. Histology of xanthelasma lesion treated by argon laser photocoagulation. Eye 1998;12:479-480.
18. Haygood LJ, Bennett JD, Brodell RT. Treatment of xanthelasma palpebrarum with bichloracetic acid. Dermatol Surg 1998;24:1027-1031.
19. Doi H, Ogawa Y. A new operative method for treatment of xanthelasma or xanthoma palpebrarum: microsurgical inverted peeling. Plast Reconstr Surg 1998 ;102:1171-1174.
20. Cartwright MJ. Xanthelasma procedures. Plast Reconstr Surg 1999; 104:878.
21. Raulin C, Schoenermark MP, Werner S, et al. Xanthelasma palpebrarum: treatment with the ultrapulsed CO2 laser. Lasers Surg Med 1999;24:122-127.
22. Hawk JL. Cryotherapy may be effective for eyelid xanthelasma. Clin Exp Dermatol 2000;25:351.
23. Borelli C, Kaudewitz P. Xanthelasma palpebrarum: treatment with the erbium:YAG laser. Lasers Surg Med 2001;29:260-264.
24. Rohrich RJ, Janis JE, Pownell PH. Xanthelasma palpebrarum: a review and current management principles. Plast Reconstr Surg 2002;110:1310-1314.
25. Levy JL, Trelles MA. New operative technique for treatment of xanthelasma palpebrarum: laser-inverted resurfacing: preliminary report. Ann Plast Surg 2003;50:339-343.
26. Shields CL, Mashayekhi A, Racciato P, et al. Disappearance of eyelid xanthelasma following oral simvastatin (ZocorTM). Br J Ophthalmol 2005; 89:639.
Eyelid Xanthelasma
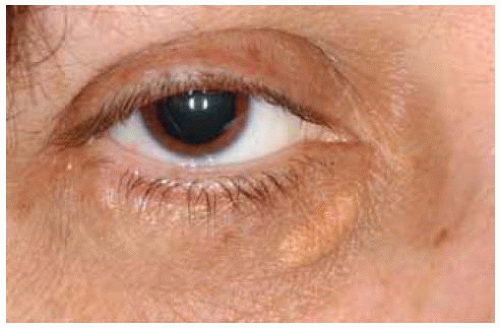 Figure 10.1. Typical xanthelasm a appearing as a yellow, slightly elevated placoid lesion in the medial aspect of lower eyelid. |
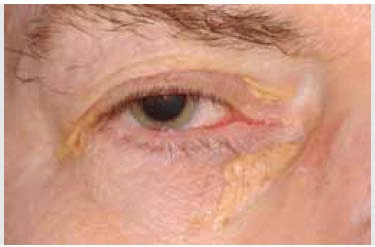
 Figure 10.2. Xanthelasmas of upper and lower eyelids at lateral and medial canthus in an elderly man. |
 Figure 10.3. Xanthelasm a in medial aspect of left upper eyelid in a middle-aged woman. |
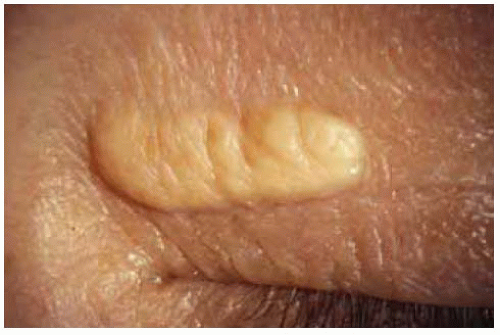 Figure 10.4. Close up view of lesion shown in Figure 10.3, showing yellow color and preservation of skin creases. |
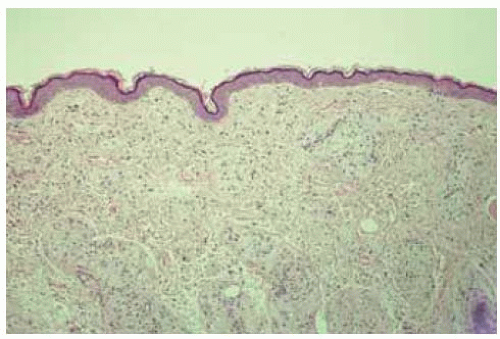 Figure 10.5. Low-magnification photom icrograph showing epiderm is and appearance of lipid containing cells in dermis. (Hematoxylin-eosin 10.) |
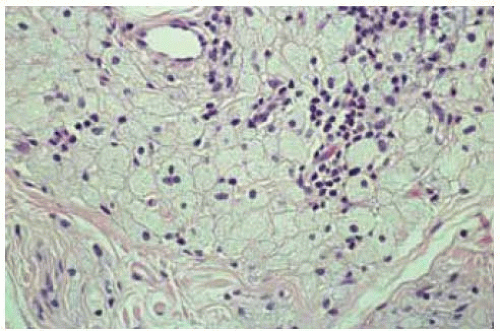 Figure 10.6. Photomicrograph showing compact round cells containing lipid. There is a mild infiltration of chronic inflammatory cells. (Hematoxylin-eosin 50.) |
Eyelid Xanthelasma and Xanthoma: Association With Systemic Conditions
1. Shields CL, Mashayekhi A, Racciato P, et al. Disappearance of eyelid xanthelasma following oral simvastatin (Zocor TM ).Br J Ophthalmol 2005;89:639.
2. Shields JA, Karcioglu Z, Shields CL, et al. Orbital and eyelid involvement with Erdheim-Chester disease. Arch Ophthalmol 1991;109:850-854.
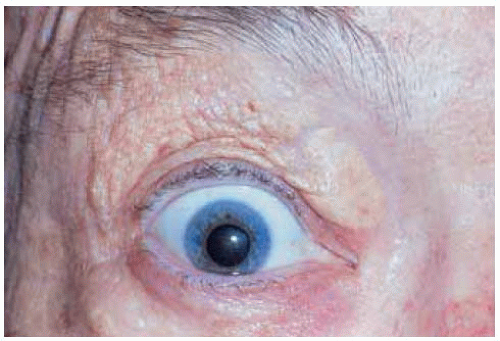 Figure 10.7. Xanthelasma in a patient with Erdheim-Chester disease. This patient also had massive bilateral orbital involvement. |
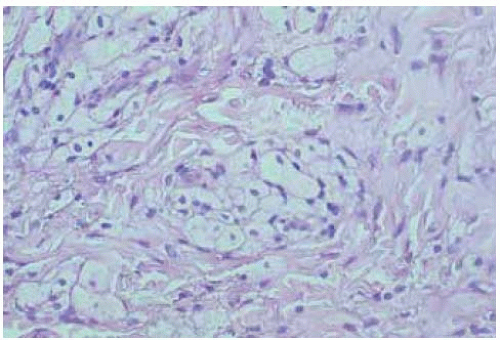 Figure 10.8. Histopathology of lesion shown in Figure 10.7 showing large, round lipid containing cells in the derm is. The xanthom a cells seem to be most concentrated around blood vessels. (Hem atoxylin-eosin 150.) |
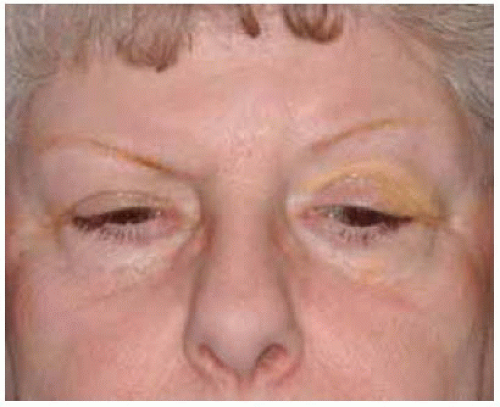 Figure 10.9. Xanthelasma of upper and lower eyelids on left side of 62-year-old woman. She had bronchial asthma and an underlying orbital mass that proved on biopsy to be compatible with Erdheim-Chester disease. |
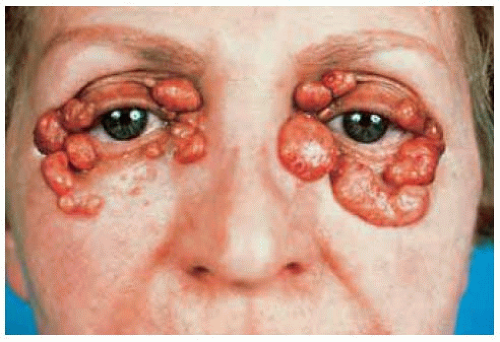 Figure 10.10. Tuberous xanthoma involving all four eyelids. Histopathologically, there was some disagreement, with some pathologists believing that the lesions could represent fibrous histiocytomas. (Courtesy of Mark Tso, MD.) |
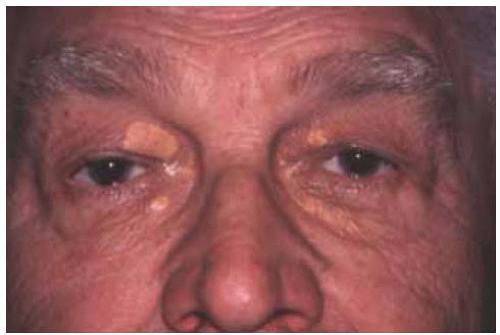 Figure 10.11. Bilateral xanthelasm a associated with hyperlipidemia. Patient started taking simvastatin for hyperlipidemia. |
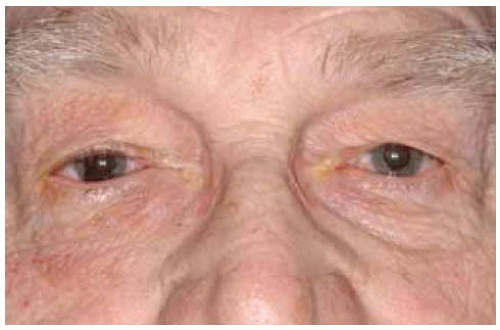 Figure 10.12. Same patient 10 years later, showing disappearance of the xanthelasma after long-term use of simvastatin. |
Eyelid Xanthogranuloma
General Considerations
Juvenile xanthogranuloma (JXG) is an idiopathic granulomatous inflammation that usually affects the skin of infants, but can occur in ocular tissues of adults as well as children (1,2,3,4,5,6,7,8,9,10,11,12,13,14). Hence, the word “juvenile” may not be always accurate. We use “juvenile xanthogranuloma” here because of its widespread usage, but we briefly mention adult xanthogranuloma as well. In a series of 53 cases of ocular JXG, the eyelid was involved in 13 (25%; 1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


