Eyelid Anatomy
Malena M. Amato
Blythe Monheit
John W. Shore
Knowledge of the relationship between structure and function in the human eyelid is essential to understand its anatomic complexity (Fig. 1). The primary function of the eyelid is to protect the eye and to preserve vision. Glands within the eyelids produce the complex tear film that provides nutrition, lubrication, and protection for the ocular surface.1 The eyelids also contribute to the lacrimal pump and their blinking action helps eliminate tears from the lacrimal lake. The eyelids play an essential role in protecting the ocular surface by means of eye protective mechanisms. These are normal physiologic responses that maintain the precorneal tear film and ensure ocular surface defense. Important eye protective mechanisms provided by the eyelids that act to protect the ocular surface from drying and exposure include tear production, eyelid closure, blink frequency and adequacy, and stabilization of the precorneal tear film by reduction of evaporative tear loss.
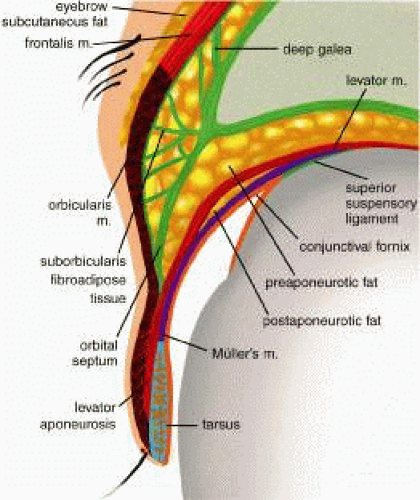 Fig. 1. Cross section of the upper eyelid. |
The eyelids are divided into anterior and posterior layers, termed lamellae (Fig. 2). The anterior lamella includes skin and orbicularis oculi muscle. A thin, multilayered septum separates the anterior preseptal tissues from the postseptal orbital structures. The posterior lamella includes the tarsus and its attachments and the conjunctiva. The upper and lower eyelid retractor muscles have attachments onto the tarsus. Knowledge of the concept of an anterior and posterior lamella is essential to understanding eyelid reconstruction, because creation of both elements is required.
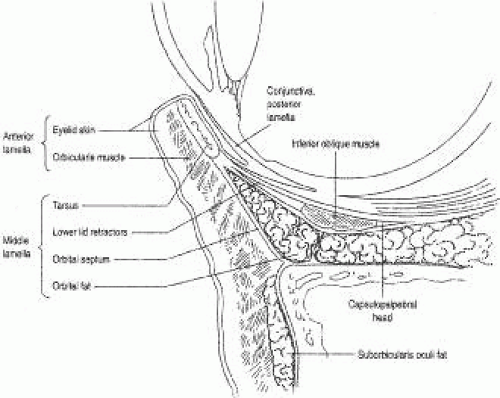 Fig. 2. Lower eyelid anatomy. (From American Academy of Ophthalmology. Orbit, Eyelids and Lacrimal System; Basic and Clinical Science Course, Section 7. San Francisco: American Academy of Ophthalmology, 2000-2001.) |
This chapter briefly reviews embryology, growth, and development of the eyelids to provide a better understanding of eyelid anatomy. The anatomy and function of the layers of the eyelid are discussed including skin and eyelid margin, orbicularis muscle, septum, orbital fat, retractor muscles, tarsus, and conjunctiva. Other important components of the adnexal structures will also be discussed; the surrounding lacrimal drainage system; and the vascular, lymphatic, and nervous supply to the orbit and eyelids.
EMBRYOLOGY
The eyelids are derived from an “inductive interaction” between mesodermal and ectodermal tissues. Development of the five brachial or pharyngeal arches occurs in the first few weeks of gestation. At about 5 weeks, a sheet of immature mesoderm originates from the first brachial arch, called the mandibular arch. Mesenchymal proliferation occurs cephalad to the first brachial arch to form the facial processes: the frontonasal, medial nasal, lateral nasal, and mandibular2 (Fig. 3). The upper eyelids are formed from the frontonasal process, which is an extension of orbital or paraxial mesoderm.3 At about 6 weeks of gestation, mesoderm from the dorsal portion of the first brachial arch forms the maxillary process. The mesoderm of the maxillary process lies in apposition to the paraxial mesoderm of the eye and nasal process and extends superiorly to form the lower eyelid. The appearance of the eyelid fold marks the beginning of eyelid development during the sixth or seventh week of gestation. Incomplete eyelid fold development is thought to be the cause for a number of congenital eyelid anomalies, including ablepharon, cryptophthalmos, and microblepharon.4
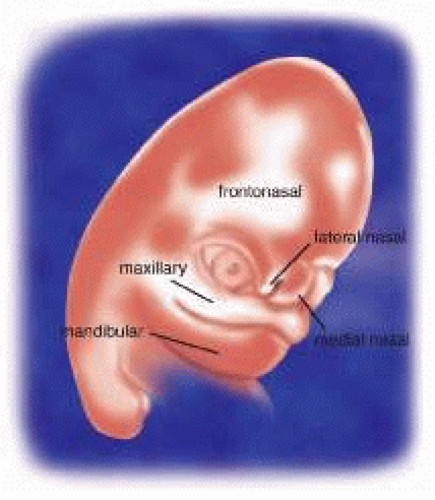 Fig. 3. The facial processes. |
The embryonic eyelids undergo a process of fusion, development, and dysjunction, or separation, during development (Fig. 4). Fusion of the eyelids occurs at about the eighth gestational week and is complete at about 10 weeks. During eyelid fusion, differentiation of the eyelid structures occurs. The cilia and meibomian and sweat glands are derived from an inward migration of ectodermal cells. Simultaneous condensation of mesenchymal tissue surrounds the meibomian glands to form the tarsus.5 Failure of fusion of the eyelids results in colobomas of the eyelid margin. At 10 weeks, the levator palpebrae superioris (LPS) begins to develop and separates from the superior rectus muscle by the fourth month. Poor development of these retractor muscles in the upper eyelid is thought to be the cause of congenital ptosis. Dysjunction, or separation, of the eyelids does not occur until the end of the fifth month and is discussed in more detail later.
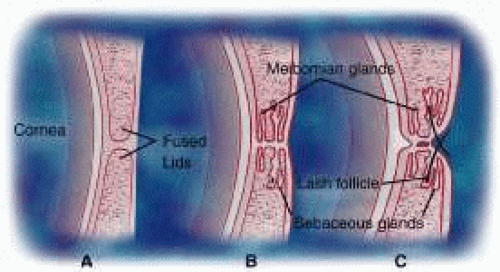 Fig. 4. Eyelid development. A. Eyelid fusion—8 to 10 weeks gestation. B. Development of eyelid margin structures—3 to 4 months gestation. C. Eyelid dysjunction—5 to 6 months gestation. |
The nasolacrimal duct derives from ectodermal tissue in the nasolacrimal groove between the lateral nasal and maxillary processes.6 This tissue is known as the nasolacrimal ectodermal cord. Mesenchymal tissues from the maxillary process cover the ectodermal tissue medially, before it canalizes. The central cells of the cord degenerate until there is a superior membrane composed of canalicular and conjunctival epithelium, as well as an inferior membrane of nasolacrimal and nasal epithelium. These superior and inferior ends are usually patent at the time of birth. The lacrimal gland arises from an outpouching of the conjunctiva as a modified salivary gland.
Mesodermal tissue from the second brachial arch spreads to cover the entire head and neck by way of myoblast induction. This superficial embryonic muscle plane becomes the superficial skeletal muscle of the eyelids. The orbicularis oculi, corrugator supercilii, and procerus muscles arise from the infraorbital lamina, immediately below the orbital rim, whereas the frontalis muscle develops from the temporal lamina. Aponeurotic fibers of the galea envelop the developing frontalis muscle and split into deep and superficial layers. The thinner superficial galea continues as the anterior muscle sheath of the frontalis and orbicularis, whereas the deep galea encompasses the sub-brow fat and continues into the eyelid as the posterior orbicularis fascia.7
Eyelid dysjunction occurs at approximately 21 to 26 weeks of gestation and results from keratinization of the eyelid margins, contraction of the inferior eyelid retractors, and secretion of sebum by the meibomian glands.8 Although separation of the eyelids is usually complete by the sixth month of gestation, it may persist until shortly before birth. Failure of eyelid separation may result in conditions such as ankyloblepharon, blepharophimosis, epicanthus, and euryblepharon. Nests of melanocytes presenting on the eyelid margins at the time of separation may form kissing nevi that can be seen after birth.
EYELID ANATOMY
THE SKIN
The eyelid skin is composed of a thin dermis and contains little subcutaneous fat.9 It is very elastic and is one of the thinnest of the body. It is loosely adherent to the underlying orbicularis oculi muscle. The skin of the upper eyelid is thinner than that of the lower eyelids. In later years, the skin becomes redundant. The excess skin provides an excellent source for skin grafting for eyelid reconstruction. There is a marked transition from the thin eyelid skin to the thicker skin of the eyebrow and cheek. The redundancy and elasticity of the eyelid skin and other eyelid structures allows for primary closure of fairly large defects (up to 30% of the eyelid in older adult patients). Upper eyelid skin laxity increases with age. This is called dermatochalasis. Dermatochalasis may progress and cause hooding, which results in mechanical ptosis that constricts the superior visual fields, or cause a mechanical upper eyelid entropion. Prominence of the lower eyelids may result from prolapse of the orbital fat, malar bags, or hypertrophic or overriding orbicularis oculi muscle. Excising excessive amounts of skin from either the upper or lower eyelids can create lagophthalmos or frank ectropion.
Transverse eyelid creases are present in both upper and lower eyelids, measuring 8 to 10 mm above the upper eyelid margin and 4 to 5 mm below the lower eyelid margin.3 The upper eyelid crease, more specifically called the superior palpebral crease, represents the cutaneous insertion of fibers of the levator aponeurosis into the preseptal orbicularis oculi, which is usually the site of the eyelid fold. The upper eyelid fold refers to the roll of skin overlying the eyelid crease. Absence of an eyelid crease implies lack of LPS function, such as seen in congenital blepharoptosis. Dehiscence of the levator aponeurosis from its insertion on the tarsus, as seen in involutional ptosis, may also result in an elevated eyelid crease. Insertions of the levator aponeurosis into the preseptal orbicularis oculi and dermis are either weak or absent in the Asian eyelid. The anatomy of the Asian eyelids is discussed later in the chapter. The region between the upper eyelid crease and the superior orbital margin is referred to as the superior orbital sulcus. Loss of orbital volume following enucleation or atrophy of orbital fat as seen with aging may result in a concavity of the superior sulcus skin and muscle.
The lower eyelid has three creases (Fig. 5). The inferior palpebral crease is a true crease marking the inferior edge of the tarsus and the insertions of the lower eyelid retractor muscles. The other two creases are less well defined and are the nasojugal crease inferomedially and the malar crease inferior to the lateral canthus, which marks the junction of the orbicularis muscle and the malar fat pad. These topographic landmarks demarcate the inferior border of the lower eyelid.
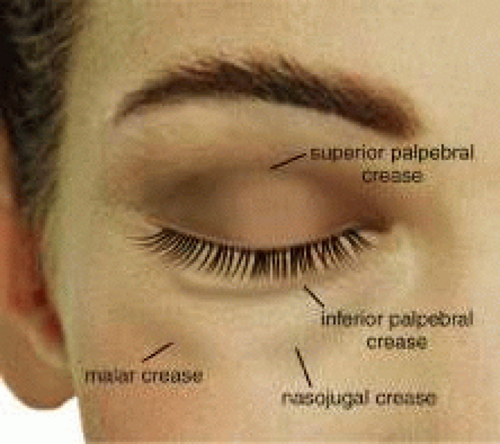 Fig. 5. Surface topography. |
EYELID MARGIN
The upper and lower eyelid margins are composed of several identifiable structures (Fig. 6). The lash line is the most anterior line found along the eyelid margin, which is the site of origin of the cilia. Approximately 100 to 150 cilia are found in the upper eyelid, and approximately 50 to 75 cilia are in the lower eyelid. The eyelashes arise from hair follicles on the anterior surface of the tarsus and project outward, anterior to the eyelid margin. Both meibomian glands and eyelashes differentiate during the second month of gestation from a common pilosebaceous unit. Congenital distichiasis can result from poor differentiation, because an extra row of lashes arises from the meibomian orifices. A lash follicle may also develop from a meibomian gland following trauma in certain disease states, or with chronic irritation, leading to acquired distichiasis.10 Each hair follicle contains approximately two sebaceous glands called glands of Zeis. Sweat glands, or glands of Moll, also lie near the cilia and empty into the adjacent follicles. Glands of Moll and Zeis secrete lipid that contributes to the superficial layer of the tear film and slows evaporation.9 Posterior to the lash line and anterior to the tarsus on the eyelid margin is the gray line. The gray line is also referred to as the muscle of Riolan and represents the pretarsal orbicularis muscle on the eyelid margin.11 An incision posterior to the gray line along the eyelid margin demarcates the anterior lamella from the posterior lamella of the eyelid. The meibomian glands and tarsus comprise the layer of the eyelid margin located immediately posterior to the gray line and is part of the posterior lamella. The meibomian glands are arranged vertically within the tarsus with their orifices at the marginal surface. A mucocutaneous junction is located posterior to the meibomian gland orifices on the eyelid margin. The lacrimal puncta are also visible on all four eyelids near the medial canthal angle. The puncta represent the opening from the eyelid margin into the ampulla and canaliculi, which is the beginning of the lacrimal drainage apparatus. The lacrimal drainage system is described later in the chapter.
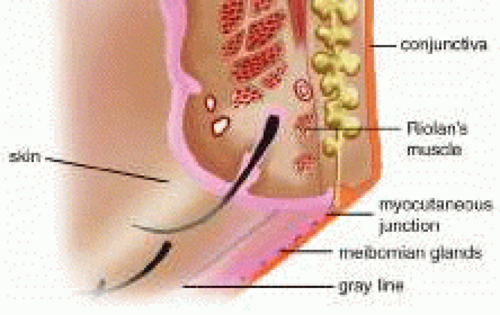 Fig. 6. Eyelid margin. |
THE ORBICULARIS OCULI MUSCLE
The orbicularis oculi muscle is a thin sheet of concentrically arranged muscle fibers covering the eyelids and periorbital region. It is the main protractor of the eyelids and its primary function is narrowing of the palpebral fissures and closure of the eyelids. It also plays a role in the lacrimal pump system. The orbicularis oculi muscle is innervated by the facial nerve, and although it is a skeletal muscle, it is under voluntary, as well as reflex, control.12 The orbicularis oculi muscle is classically divided into three anatomic parts13 (Fig. 7). The pretarsal orbicularis overlies the tarsus, the preseptal orbicularis overlies the orbital septum, and the orbital portion lies beneath the skin that surrounds the remaining orbital aperture (Fig. 8). The pretarsal and the preseptal orbicularis together are referred to as the palpebral orbicularis. Voluntary squeezing of the orbital orbicularis closes the palpebral fissure and protects the globe and orbit from injury. Involuntary movements, such as blinking and the functioning of the lacrimal pump, result mainly from contraction of the palpebral portion of the orbicularis oculi muscle.10
 Fig. 7. Orbicularis oculi muscle, cadaver dissection. A. Orbital portion. B. Preseptal portion. C. Pretarsal portion. |
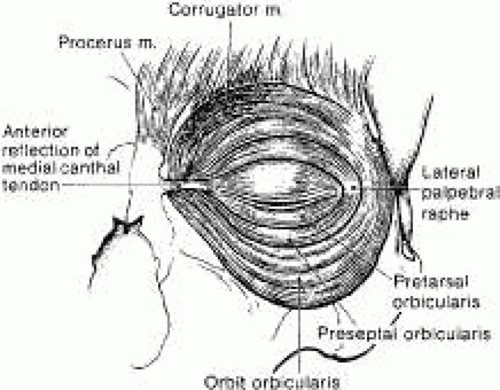 Fig. 8. Protractor muscles of eyelid closure with the skin layer removed. |
The orbital portion of the orbicularis oculi muscle is the outermost and the largest segment. It is responsible for forcible eyelid closure (squeezing) and voluntary eyelid closure (winking). The orbital portion of the orbicularis muscle originates from the periosteum of the frontal and maxillary bones at the insertion of the medial canthal tendon (MCT). It is a continuous muscle that encircles the orbit before reinserting at the medial canthus inferiorly where it is attached to the periosteum of the posterior lacrimal crest, the lacrimal fascia, and the MCT.12 Superiorly, the orbital portion extends to the eyebrow and interdigitates with the frontalis and the corrugator superioris muscles. Medially, attachments extend from the supraorbital notch to the side of the nasal bone. Inferiorly, the orbital portion arises from the anterior limb of the MCT and the surrounding periosteum and extends to the infraorbital foramen where it continues along the infraorbital margin. Laterally, the orbital orbicularis portion courses over the zygoma and cheek and over the temporal fascia.
The preseptal portion of the orbicularis oculi muscle overlies the orbital septum and functions in voluntary eyelid closure (winking) and involuntary eyelid closure (blinking). The action of the superior preseptal orbicularis muscle can also force the eyelid margin below the level of its canthal attachments as seen in looking down.14 The preseptal portion has a superficial origin from the anterior limb of the MCT and a deep origin, called the Jones muscle, which arises from the posterior lacrimal crest and the fascia surrounding the lacrimal crest.8 The orbital segment interdigitates with the preseptal orbicularis muscle and courses laterally across the upper and lower eyelids. The two segments fuse to form the lateral horizontal raphe, which overlies the lateral canthal tendon (LCT) and the lateral orbital rim.
The pretarsal portion of the orbicularis muscle is primarily responsible for horizontal movement of the eyelid, which is important in the function of the lacrimal pump. It also assists in eyelid closure mainly during involuntary blinking. The lower one third of the pretarsal muscle in the upper eyelid is adherent to the underlying tarsus, whereas the upper two thirds of the muscle is adherent to the superficial insertion of levator aponeurosis at the superior tarsal border.14 There are two medial insertions of the pretarsal portion of the orbicularis muscle. The superficial head condenses to form the anterior limb of the MCT and inserts into the anterior lacrimal crest. The deep head, called the tensor tarsi muscle of Horner, shares the same site of origin as the preseptal muscle. It inserts on fascia covering the lacrimal sac fossa and on the periosteum of the posterior lacrimal crest. Here, it is identified as the posterior limb of the MCT15 (Fig. 9). Contraction of the Horner’s muscle draws the eyelids (especially the lower) medially and posteriorly. The resulting lateral pull on the lacrimal diaphragm creates a negative pressure in the lacrimal sac and draws the tears from the canaliculi into the sac. The deep and superficial heads of the pretarsal orbicularis oculi muscle encircle both lacrimal canaliculi and along with the Jones muscle facilitate tear drainage. Contraction shortens the ampullae of the canaliculi system and facilitates the movement of tears into the sac. The lacrimal drainage system is described in further detail later in the chapter. Laterally, the upper and lower pretarsal muscles fuse to form the LCT and insert 3 to 4 mm deep to the lateral palpebral raphe onto the lateral orbital tubercle. The deep medial and lateral attachments of the pretarsal orbicularis oculi muscle are important in maintaining eyelid to globe apposition.
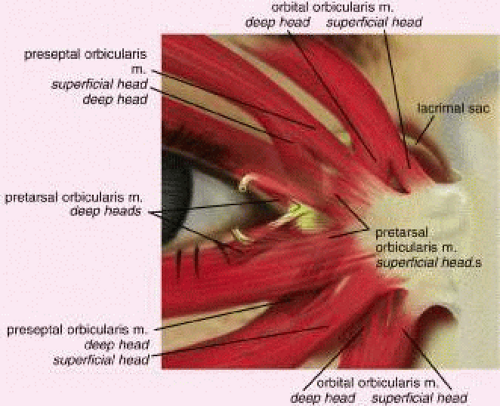 Fig. 9. Medial attachments of the orbicularis oculi muscle. |
ORBITAL SEPTUM
The orbital septum is a thin, fibrous, multilayered sheath that arises from the anterior periorbita (periosteal lining of the orbit) at the arcus marginalis (Fig. 10). The orbital septum separates the eyelids from the orbit and serves as an important anatomic barrier to infection, hemorrhage, and edema. Inflammatory or infectious processes anterior to the septum are considered preseptal, whereas similar findings posterior to the orbital septum are considered orbital. In older individuals, the septum can become tenuous. Orbital or preaponeurotic fat is an important anatomic landmark and herniation of orbital fat through the septum from trauma or surgery indicates a disruption of the orbital septum.
 Fig. 10. The multilayered orbital septum; the skin and orbicularis muscle are retracted. |
From the arcus marginalis, the septum spans the anterior orbit in a plane deep to the orbicularis oculi muscle and ultimately fuses with the eyelid retractors or tarsus (Fig. 11). In the upper eyelid, the orbital septum adjoins the posterior epimysium of the orbicularis before it fuses with the levator aponeurosis approximately 2 to 3 mm above the superior tarsal border and about 10 mm above the lash line.16 In the lower eyelid, the septum arises from the inferior orbital rim as a condensation of the periorbita and periosteum. It continues anteriorly until it joins with the lower eyelid retractors as a single unit at a point 4 to 5 mm below the inferior tarsus or it inserts on the lower border of the tarsus. The septum travels medially with the pretarsal orbicularis muscle and attaches to the posterior lacrimal crest with a few fibers extending to the anterior lacrimal crest. Laterally, the septum attaches to the deep insertion of the pretarsal segment of the orbicularis muscle and inserts onto the lateral orbital tubercle.17
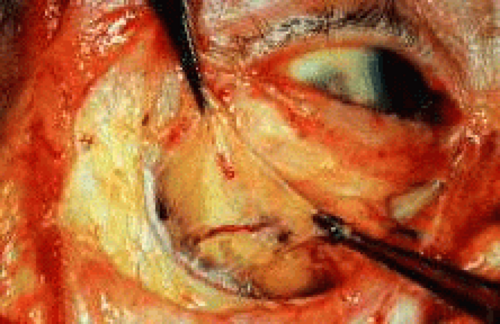 Fig. 11. The orbital septum. (From Zide BM, Jelkes GW. Surgical Anatomy of the Orbit. New York: Raven Press, 1985.) |
In the Asian eyelids, the eyelid creases vary in position in relation to the eyelid margin and may be lower than the occidental eyelid, or they may be absent altogether. In the upper eyelid, the orbital septum may fuse with the aponeurosis as is inserts into the tarsus. This insertion can occur as high as the superior border of the tarsus or as low as the lash line accounting for the lower or absent upper eyelid crease.3 There are also differences in the Asian lower eyelids. Epiblepharon is a common finding in the Asian lower eyelid and is seen as an additional fold of skin running horizontally below the lower eyelid margin. It is often associated with a loss of the eyelid crease or with a crease that rests very close to the eyelid margin of the lower eyelid. The absence of an eyelid crease may be due to lack of deep anchoring of the superficial skin to the preseptal portion of the orbicularis oculi muscle.18 An overriding orbicularis muscle is also associated with epiblepharon. The weight of the skin fold and the orbicularis muscle may rotate the lower eyelid margin inward, creating an entropion.
FAT
Fat within the orbit and eyelids serves as a protective cushion for the globe and facilitates movement of the globe. There are three general locations of fat that are described: eyelid, sub-brow, and orbital. In the upper eyelid, there are two fat pads, medial and central (preaponeurotic) (Fig. 12). The central preaponeurotic fat is divided by the trochlea of the superior oblique tendon and fascial strands of the medial retinaculum. These divisions are arbitrary and the fascial planes can be variable, because eyelid fat is interconnected and contiguous with deeper orbital fat. The preaponeurotic fat pad is an important surgical landmark, because it lies just posterior to the orbital septum and anterior to the levator aponeurosis (Fig. 13). The central preaponeurotic fat pad tends to be yellow as compared with the whiter more fibrous medial fat pad. The medial fat pad is derived from orbital fat deep to the levator muscle. It is more vascular because of the location of the palpebral arterial arcade that serpiginously courses through the medial fat pad.19,20 The lacrimal gland occupies the temporal space lateral to the central preaponeurotic fat pad. The lacrimal gland is a firm, pink, vascular, lobulated structure that produces the aqueous component of the precorneal tear film. (The anatomy and function of the lacrimal gland is described later in the chapter.) Care must be taken to avoid excision of the lacrimal gland while liposculpturing during blepharoplasty. Fine connective tissue septa extend anteriorly from the capsule of preaponeurotic fat to the orbital septum and posteriorly to the levator aponeurosis.17 The postaponeurotic or pretarsal space, located between the levator aponeurosis anteriorly and the tarsus posteriorly, may contain a small amount of peripheral orbital fat. The fibrous septa compartmentalizing superficial and deep orbital fat and extensions of the fascial sheaths of the orbital muscles and eyelid structures are of great importance to the movement of the upper eyelid.
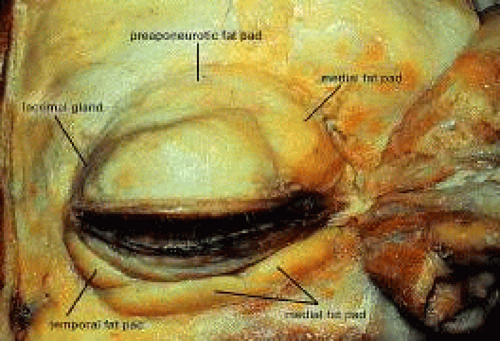 Fig. 12. Eyelid fat pads in a cadaver dissection. |
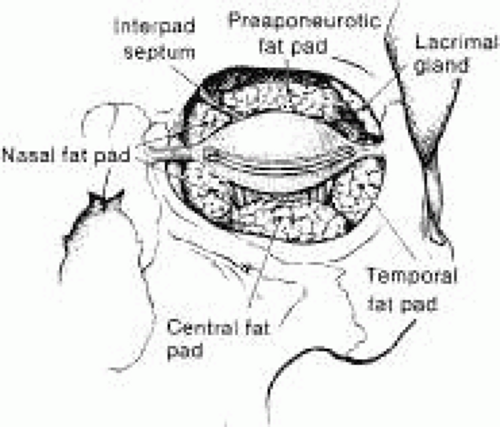 Fig. 13. Frontal view of the eyelids and orbit showing the fat pad distribution; the skin and protractor muscles have been removed. |
Sub-brow fat can form a redundant upper eyelid skin fold and undergoes gravitational descent during aging (Fig. 14). In females, the eyebrow is generally arched and above the level of the supraorbital rim. The male eyebrow is flatter and at the level of the supraorbital rim. The eyebrow fat pad is more prominent in the male, producing a fuller appearance in the lateral brow area. The position of the eyebrow can affect the height and excursion of the upper eyelid and must be considered in a patient being evaluated for blepharoptosis or for blepharoplasty. The retro-orbicularis oculus fat (ROOF) is defined as the layer of fibrofatty tissue deep to the orbicularis oculus muscle, superficial to the orbital septum and orbital rim, and extending medially from the superior orbital nerve and laterally over the lateral upper orbit.21 Resection of the ROOF in conjunction with aesthetic blepharoplasty can soften and flatten heaviness and bulkiness in the lateral upper orbital and brow region. A direct or indirect browplasty or browpexy may be an alternative treatment for patients with brow ptosis.22 One must discern patients with eyebrow ptosis from those with eyelid ptosis caused by levator muscle or Muller’s muscle dysfunction.
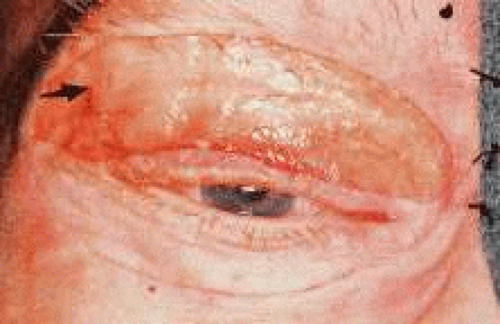 Fig. 14. Sub-brow fat. (From Zide BM, Jelkes GW. Surgical Anatomy of the Orbit. New York: Raven Press, 1985.) |
Some surgeons consider the lower eyelid to have three fat pads.9,23 A medial fat pad is subdivided by the origin of the inferior oblique muscle. Temporally, a small fat pad lies inferior to the lateral canthus and is separated from the main fat pad by a fibrous extension of connective tissue from the orbital septum and periorbita that joins with the capsulopalpebral fascia (CPF) and Lockwood’s ligament.24 Because the eyelid fat pads are in direct communication with the deep extraconal fat of the orbit, caution must be exercised when handling orbital fat in the anterior orbit. Traction on the fat pad may injure deep orbital vessels causing orbital hemorrhage and permanent loss of vision.19,25
The midfacial fat compartments include the suborbicularis oculi fat (SOOF) and malar fat pads. These fat compartments are bound to the orbicularis muscle by the superficial muscular aponeurotic system (SMAS) of the cheek. The SOOF is composed of the deep subcutaneous fat and connective tissue, which is located beneath the orbicularis muscle in the lower eyelid and extends into the midface. In the aging lower eyelid, eyelid tone decreases with associated skin and muscle laxity. Horizontal laxity of the lower eyelid increases, and pseudoherniation of orbital fat may result in contour irregularities. The SOOF can become apparent with the gravitational descent seen in the midface with aging and contributes to the aesthetic deformity of the lower lids. Malar bags may also develop from descent of the malar fat pad. A SOOF lift is a technique used for midfacial rejuvenation that includes subperiosteal dissection of the SMAS to elevate the SOOF and redraping the orbicularis muscle to reposition the midface.26 Recent emphasis has been placed on a SOOF lift for midfacial rejuvenation surgery in conjunction with a lower eyelid blepharoplasty and lateral canthoplasty.27 The SOOF lift has also been used for functional repair of lower eyelid deformities seen in patients with significant involutional or cicatricial ectropion.
Asian eyelids characteristically have a fuller appearance than the eyelids of Caucasian individuals. Upper eyelid fullness in the Asian person is typically caused by extension of preaponeurotic fat and brow fat into the upper eyelid. A recent study by Carter and colleagues28 used high-resolution magnetic resonance images to compare Asian and Caucasian lower eyelids. The study revealed two major differences in the lower eyelid anatomy: (1) there is more anterior projection of orbital fat with respect to the orbital rim in the Asian eyelid as compared with whites and (2) there is a more superior projection of orbital fat that extends to the inferior border of the tarsus with poorly defined eyelid creases in Asians.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


