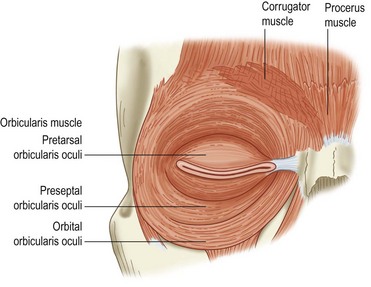
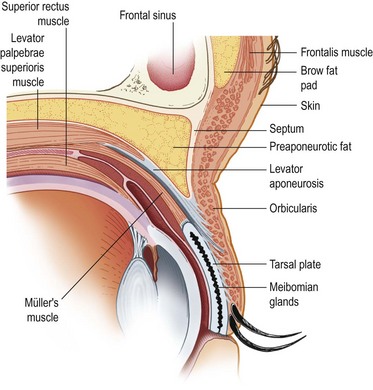
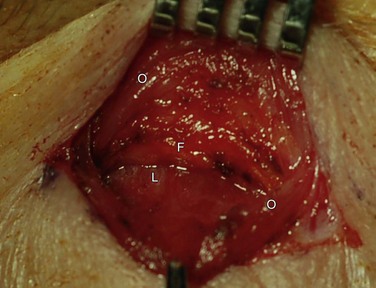
2 The eyelids comprise of an upper and lower eyelid, joined at the medial and lateral canthi. The average aperture of the eyelids measures about 30 mm in horizontal width, and approximately 10 mm in vertical height. The highest peak on the upper eyelid lies slightly nasal, and the lowest contour of the lower eyelid rests slightly lateral. The upper eyelid generally covers 1–3 mm of the upper cornea, and the lower eyelid typically rests at, or near the lower limbus. The upper eyelid crease falls 6–10 mm from the eyelid lash line. The brow is positioned anterior to the superior orbital rim.1–4 The main protractor of the eyelid, which serves to close the eye, is the orbicularis oculi. It is innervated by the facial nerve, and divided into the pretarsal, preseptal, and orbital portions (Fig. 2.1). The pretarsal and preseptal portions are used in spontaneous blink, and the orbital portion is needed for forced eyelid closure. Facial nerve palsy can lead to lagophthalmos and incomplete blink. Whitnall’s ligament or superior traverse ligament is a condensation of elastic fibers of the anterior sheath of the levator muscle. It is located between the transition of the levator aponeurosis and muscle. It provides the suspension support for the upper eyelid and superior orbital tissues. It is thought to transfer the vector of force of the levator muscle from anterior–posterior to superior–inferior. It is analogous to Lockwood’s ligament in the lower eyelid. Medially it attaches near the trochlea and superior oblique tendon, and laterally, it runs through the lacrimal gland, and attaches to the inside of the lateral orbital wall, approximately 10 mm above the lateral tubercle.1–4 The levator aponeurosis divides into an anterior and posterior portion just above the superior tarsal border. The anterior portion inserts into the pretarsal orbicularis. The most superior portion of these attachments forms the eyelid crease with contraction of the levator complex (Fig. 2.2). The posterior portion inserts onto the anterior surface of the tarsus. The aponeurosis appears as a thick whitish band between Whitnall’s ligament and the tarsal plate (Fig. 2.3).
Eyelid Anatomy and Function
Overview of External Anatomy
Eyelid Muscles: Protractors
Eyelid Muscles: Retractors
Upper Lid Retractor: Levator
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Eyelid Anatomy and Function