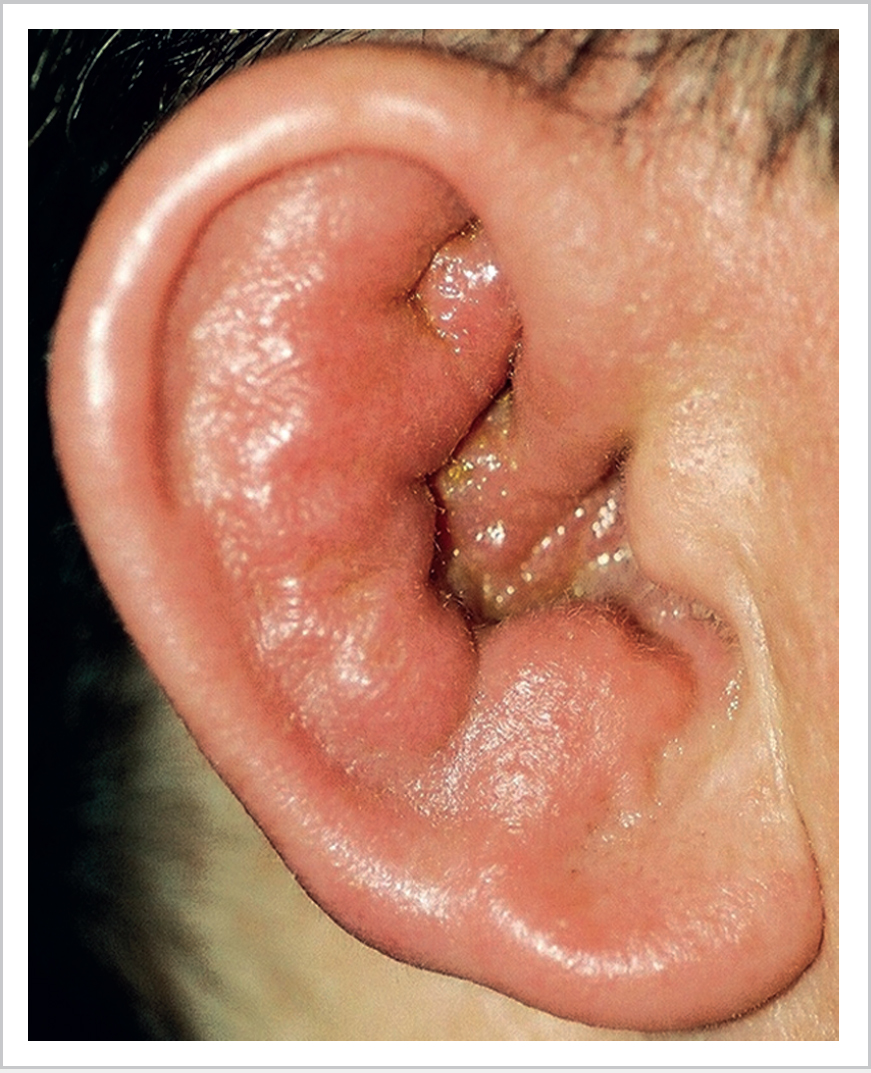
3 External Ear Disease • Cellulitis of auricle: regional neck nodes may be inflamed; usually gram +ve cocci (not Pseudomonas) • Allergic dermatitis: no history of trauma, peau d’orange/shiny appearances may occur; c/o itching; sensitization may occur with repeated exposure • Auricular erysipelas: superficial cellulitis caused by group A Streptococcus; often preceded by trauma; may lead to systemic toxicity, contagious • Infectious (peri)chondritis (Fig. 3.1): Pseudomonas, Staphylococcus aureus, and Streptococcus; aggressive Rx required; clinically sparing of lobule • Relapsing polychondritis: recurring inflammation of cartilage throughout body (e.g., nose, larynx); autoimmune response to type II collagen; 85 to 90% of these patients get auricular cartilage involvement; recurrent episodes may cause “cauliflower” ear; systemic corticosteroids for acute episodes • Eczema, psoriasis • Furuncle: small abscess in a hair follicle; if ready to rupture, gently open with tip of sterile needle • Acute otitis externa: • Malignant (necrotizing) otitis externa: • Chronic otitis externa: chronic itching with skin often shiny, scaling and devoid of wax; cultures can be non-specific or misleading; treat secondary infection and use topical steroids • Post-inflammatory stenosis of EAM (external auditory meatus) subepithelial fibrosis with progressive narrowing of EAM; early management includes local steroids; once scar is mature, consider tissue excision and split-thickness grafting but risk of recurrence • Myringitis bullosa hemorrhagica: • Granular myringitis: Chondrodermatitis nodularis chronica helicis (Winkler nodule) • Benign, usually on rim of helix/antihelix • Red, raised, and tender nodule with central depression/crater • Tenderness affects sleeping position • Full-thickness excision; topical steroids may help while waiting for surgery • Gouty tophi: yellow/pink nodules on helix; control of gout required • Keratoacanthoma: benign tumour of hair follicles most common anterior to tragus; rapidly growing and painless—biopsy to distinguish from neoplastic lesions • Hypertrophic scars remain confined to site of injury • Keloid scars invade adjacent normal tissue, commonly lobule from earrings; topical injection of steroids (± excision) • Risk factors: • Basal cell carcinoma: • Squamous cell carcinoma (SCC): • Produced from ceruminous glands in outer 1/3 of ear canal • Usually natural clearance aided by epithelial migration
3.1 Inflammatory Disorders of the Auricle
3.2 Inflammatory Disorders of the External Auditory Meatus
 Pseudomonas infection most common; also S. aureus, Candida, Aspergillus
Pseudomonas infection most common; also S. aureus, Candida, Aspergillus
 Risk factors: prolonged water exposure, repeated trauma (e.g., cotton buds), eczema/psoriasis, middle ear discharge
Risk factors: prolonged water exposure, repeated trauma (e.g., cotton buds), eczema/psoriasis, middle ear discharge
 Painful (especially on tragal movement): narcotic painkillers may be required
Painful (especially on tragal movement): narcotic painkillers may be required
 Rx: aural toilet, Pope wick and antibiotic/steroid drops, water exclusion
Rx: aural toilet, Pope wick and antibiotic/steroid drops, water exclusion
 May spread to cause facial cellulitis, requiring systemic antibiotics
May spread to cause facial cellulitis, requiring systemic antibiotics
 Otomycosis: fungal infection often follows prolonged treatment with topical antibiotics
Otomycosis: fungal infection often follows prolonged treatment with topical antibiotics
 Otitis externa becoming an invasive infection, leading to osteomyelitis (tympanic plate to skull base)
Otitis externa becoming an invasive infection, leading to osteomyelitis (tympanic plate to skull base)
 Pseudomonas aeruginosa usual infecting organism
Pseudomonas aeruginosa usual infecting organism
 Diabetic patients and immunocompromised most affected, often elderly
Diabetic patients and immunocompromised most affected, often elderly
 Unresolving infection with deep otalgia and granulations noted at cartilage/bone junction of external ear canal—here the clefts of Santorini provide the pathway for the spread of infection
Unresolving infection with deep otalgia and granulations noted at cartilage/bone junction of external ear canal—here the clefts of Santorini provide the pathway for the spread of infection
 Cranial nerve (CN) palsies (7–12) and death (intracranial infection) can occur in severe cases
Cranial nerve (CN) palsies (7–12) and death (intracranial infection) can occur in severe cases
 Rx: rigorous diabetic control, long-term intravenous (IV) antibiotic, topical ciprofloxacin drops; possible role for hyperbaric oxygen
Rx: rigorous diabetic control, long-term intravenous (IV) antibiotic, topical ciprofloxacin drops; possible role for hyperbaric oxygen
3.3 Inflammatory Disorders of the Tympanic Membrane
 Painful infection of tympanic membrane (TM), uncertain causative organism
Painful infection of tympanic membrane (TM), uncertain causative organism
 Mostly in autumn, benign and self-limiting
Mostly in autumn, benign and self-limiting
 Blisters of varying size on TM/EAM—filled with serous/hemorrhagic fluid
Blisters of varying size on TM/EAM—filled with serous/hemorrhagic fluid
 Analgesia (± antibiotic/steroid drops)
Analgesia (± antibiotic/steroid drops)
 Separate or confluent granulations on surface of TM
Separate or confluent granulations on surface of TM
 Topical drops and superficial curettage
Topical drops and superficial curettage
 Some progress to inflammatory obliteration of deep EAM
Some progress to inflammatory obliteration of deep EAM
3.4 Non-inflammatory Lesions of the External Ear
3.4.1 Other Pinna Lesions
3.4.2 Carcinoma of the Auricle
 Older men, light-haired, fair-skinned individuals
Older men, light-haired, fair-skinned individuals
 End stage of actinic-induced epidermal dysplasia
End stage of actinic-induced epidermal dysplasia
 Gradual pushing deep invasive margin
Gradual pushing deep invasive margin
 Local excision
Local excision
 Aetiology sun exposure, arsenic, radiation, previous scarring
Aetiology sun exposure, arsenic, radiation, previous scarring
 Usually progress from solar keratosis through dysplasia and carcinoma in situ
Usually progress from solar keratosis through dysplasia and carcinoma in situ
 Protuberant areas like helix most affected
Protuberant areas like helix most affected
 Local excision with flaps for early lesions, ± radiotherapy
Local excision with flaps for early lesions, ± radiotherapy
3.4.3 Wax
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


