Chapter 53 Extended Middle Cranial Fossa Approach
Gaining access to the cerebellopontine angle (CPA) and prepontine cisterns has presented a formidable challenge. Approaches designed to expose infraclinoid basilar tip aneurysms, petroclival meningiomas, chondromas, chondrosarcomas, and chordomas involving the petrous apex and clivus must take into consideration the vital neighboring neurovascular structures.1,2 The risks encountered in the region of the prepontine cistern during the management of aneurysms of the posterior circulation were best described by Drake3 in 1961, when he said, “the upper clival region is to be considered no-man’s land.” Several conventional neurosurgical approaches to this region have been described, including the subtemporal and trans-sylvian and a combination half-and-half approach incorporating both techniques. Despite advances in microsurgical techniques and neuroanesthesia, the petrous bone has previously been an impediment to satisfactory exposure in this anatomically complex region. Modern skull base approaches, including the middle cranial fossa and the middle fossa transpetrous or extended middle fossa (EMF), have been instrumental in removing the petrous barrier, minimizing temporal lobe retraction, and improving the line of sight for the neurosurgeon.
The middle fossa approach was first described in the literature in 1904.4 The sentinel work of House in 19615 led to a revitalization and refinement of this approach to the internal auditory canal (IAC), CPA, and prepontine cisterns. By extending the traditional middle fossa dissection anteriorly to the clivus, the EMF approach provides complete exposure of the IAC and the prepontine cisterns and the mid to upper clivus.6–11 Posteriorly, the approach allows access to tumors approaching, but not entering the jugular foramen (Table 53-1).
TABLE 53-1 Indications for Extended Middle Fossa Approach
| Vestibular schwannoma (<2 cm) |
| Petroclival meningioma |
| Chondroma |
| Chondrosarcoma |
| Chondroblastoma |
| Chordoma |
| Trigeminal schwannoma |
| Infraclinoidal basilar tip aneurysms |
SURGICAL ANATOMY
The surgical anatomy of the temporal bone from the middle fossa approach is complex (Fig. 53-1).12 Landmarks are not as apparent as with other approaches through the temporal bone. Laboratory dissection is essential so that the surgeon may become familiar with the anatomy from above.
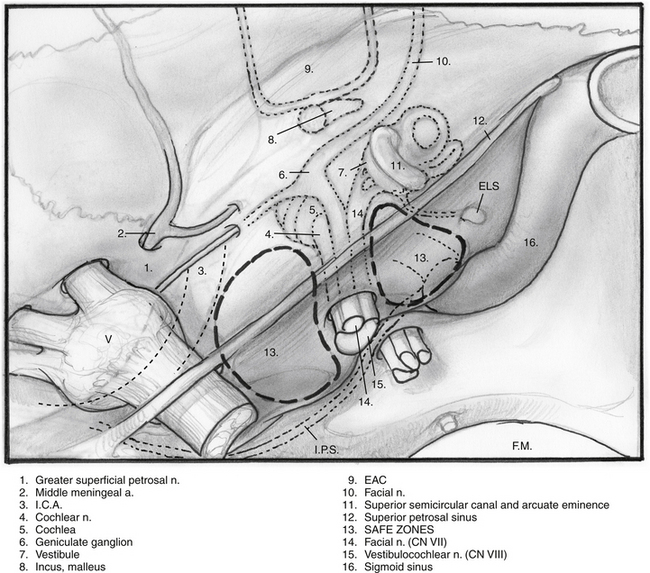
Anteriorly, the limit of the dissection is the middle meningeal artery, which is anterior and lateral to the greater superficial petrosal nerve. Excessive anterior retraction can lead to postoperative paresthesias in CN V3. The arcuate eminence roughly marks the position of the superior semicircular canal. The relationship between the arcuate eminence and the superior semicircular canal is inconstant.13 The superior semicircular canal tends to be perpendicular to the petrous ridge. Medially, the superior petrosal sinus runs along the petrous ridge.
SURGICAL TECHNIQUE
The patient is placed in the supine position with the head turned to the side opposite the lesion (Fig. 53-2). The surgeon is seated at the head of the table, and the anesthesiologist is seated at the foot. An incision is made in the preauricular area and extended superiorly in a gently curving fashion. Care must be taken near the anterior extension of the incision to avoid injury to the temporal branch of the facial nerve (see Fig. 53-2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


