Fig. 8.1
Drawings and photos of the excimer laser trabeculostomy procedure. The laser fiber is introduced into the anterior chamber through a clear cornea incision (a) and advanced across the anterior chamber (b) to the trabecular meshwork of the opposite quadrant (c). When the fiber tip is in contact with or slightly compresasing the trabecular meshwork laser pulses are initiated (d). Tissue fluorescence produced by each UV laser pulse can be visualized gonioscopicly (e). A series of laser channels of approx. 0.2mm diameter each enabels flow from the anterior chamber to Schlemm’s canal (f). a, c-d, and f: Peschke GmbH, Waldshut-Tiengen, Germany; b and e: U. Giers

Fig. 8.2
Gonioscope view/IOP high = SC not visible (U. Giers)
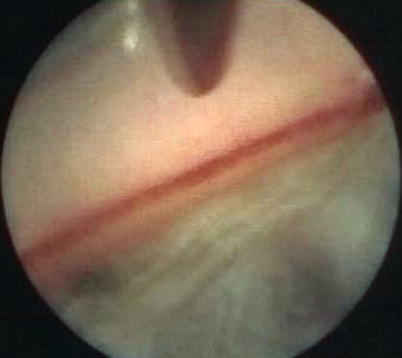
Fig. 8.3
Endoscopic view/IOP low = SC visible, blood filled (U. Giers)
By means of the essentially non-thermal photoablation using the specified laser parameters, ELT evaporates human tissue, denaturing the organic structures without producing undesirable marginal necrosis [24]. ELT excises the TM, the juxtacanalicular TM, and the inner wall of SC without damaging the outer wall of SC or the collector channels [25]. No filtering fistula or bleb is created [21, 26, 27].
Technical Aspects of Performing an ELT Procedure
The current ELT procedure is performed with an AIDA XeCl laser (TUI-Laser AG, Germering, Germany) in the following manner:
1.
The laser is automated to internally calibrate and control the output fluence in accordance with the manufacturer’s specifications. Unlike solid-state lasers, this XeCl gas laser requires a short “warm up” time during which the output energy is stabilized before use.
2.
The sterile, non-reusable fiber-optic delivery system is coupled to the laser. The output beam is then adjusted at the fiber tip to ensure suprathreshold fluence for tissue ablation at the fiber tip. The console includes a power meter to enable this calibration which is performed prior to each procedure, similar to the tuning of a phaco handpiece before use.
3.
Topical, peribulbar, or retrobulbar local anesthesia is administered. In ELT alone, topical pilocarpine 2 % is used preoperatively to constrict the pupil. In phakic patients this may also assist in protecting the lens. Alternatively, intracameral Miochol (acetylcholine 10 mg/ml) may be used.
4.
A 1 mm paracentesis is created in the superotemporal perilimbal cornea 2 o’clock for left eyes and 10 o’clock for right eyes, or in combined cataract and ELT procedures, the previously created phaco-tunnel may be used in a similar fashion (Fig. 8.4).
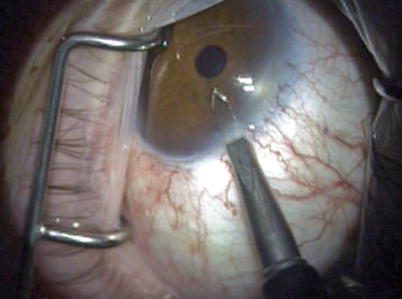
Fig. 8.4
Paracentesis in the superotemporal perilimbal cornea (U. Giers)
5.
A viscoelastic agent (Healon) fills the anterior chamber through the paracentesis. Depending on the surgeons’ preference, the IOP may be unchanged or increased by this injection, enabling or precluding visualization of SC by blood reflux (Fig. 8.5).
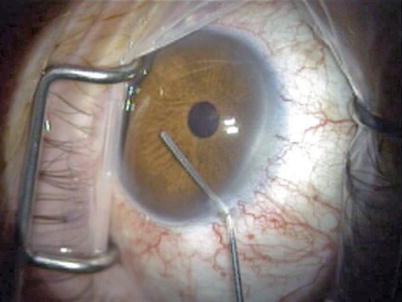
Fig. 8.5
Viscoelastic agent is introduced (U. Giers)
6.
The laser probe is inserted into the anterior chamber through the paracentesis (Fig. 8.6) and is advanced to the opposite chamber angle via gonioscopic (using the surgeon’s preferred goniolens) or endoscopic visualization (Fig. 8.7). The ELT fiber may be attached coaxial with an endoscope, or a second paracentesis endoscopic view may be utilized.
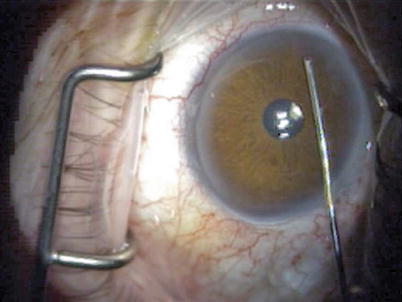
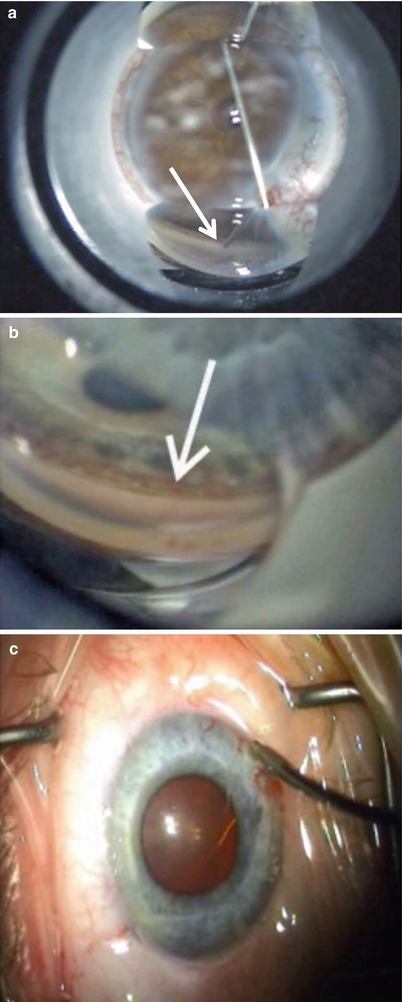
Fig. 8.6
Laser probe is inserted through the paracentesis to cross the anterior chamber (U. Giers)
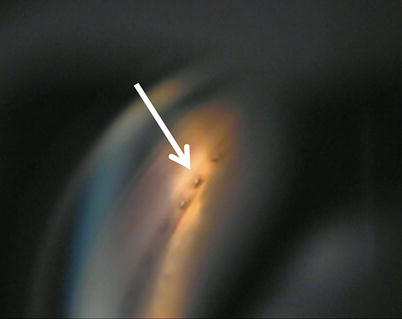
Fig. 8.7
(a) Gonioscopic view of ELT probe in contact with TM (white arrow). (b) Blood in Schlemm’s canal (arrow) verifies appropriate targeting and depth, gonioscopic view (c) Induced blood reflux verifies success and enables documentation of number of successful channels into Schlemm’s canal (U. Giers)
7.
The fiber tip is centered on the pigmented TM and advanced to be in contact with the TM. SC is targeted whenever visible, or surgeons are advised to alternate placement of the fiber to anterior, mid, and posterior TM regions to assure some of the channels will, in fact, enter into SC. The number of pulses which controls the penetration depth is fixed, similar to the penetration depth control in LASIK. Perforation of the inner wall of SC into SC depends, therefore, on its distance from the fiber tip which can be variable depending on the angle of placement and the amount of pressure on the fiber. The calculation of this distance was determined in numerous preclinical experiments [28, 29]. Thus, the most common protocol consists of ten probe placement sites on TM, a percentage of which is likely to enter SC.
8.
The laser is activated, delivering laser pulses at 20 Hz per treatment site. Each pulse converts the tissue at the fiber tip into gas. This gas may be seen exiting around the fiber tip during each ablation (Fig. 8.8).
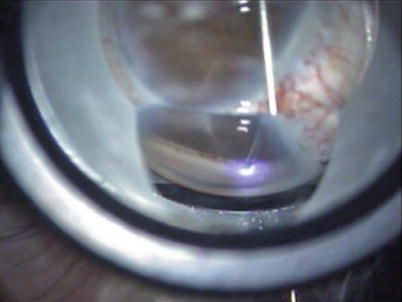
Fig. 8.8
In this series of chanels created tissue fluorescence is visible during a UV laser pulses creating the next channel. (U. Giers)
9.
As the channel is created, pulse by pulse, an opening is created from the anterior chamber into SC through photoablation of the TM, the juxtacanalicular TM and the inner wall of SC. As soon as the outflow obstruction at the fiber tip is removed as SC is entered, the pathway for the gas, previously retrograde around the fiber, becomes anterograde, entering SC. In theory, this product-of-ablation gas is then assumed to dilate SC, pushing the outer wall away and concurrently dilating the adjacent surrounding collector channels. This concept of the product-of-ablation gas dilation of SC and collector channels is termed “pneumatic canaloplasty.” Once adequate imaging devices are developed to visualize this process in real time, this theory can be validated.
10.
The probe tip is then repositioned such that additional channels are created.
11.
The probe is removed from the anterior chamber.
12.
The viscoelastic agent is exchanged for BSS with irrigation/aspiration, coaxial or bimanual (Fig. 8.9).
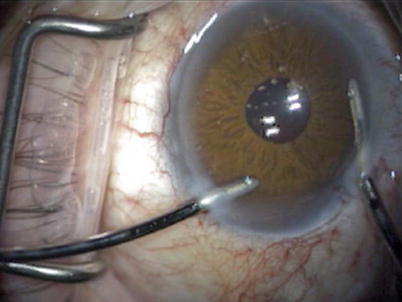
Fig. 8.9
Viscoelastic is exchanged for BSS (U. Giers)
13.
The anterior chamber can be monitored for the number of and location of patent trabeculostomy sites by blood reflux from SC during a period of iatrogenic temporary hypotony during the viscoelastic agent/fluid exchange.
Postoperative topical ophthalmic medication regimens are individualized by surgeon, most include:
1.
A combination of steroid and antibiotic eye drops or ointment is administered immediately at the end of the procedure.
2.
The operated eye is shielded or patched, and the patient is released once stable, similar to after phacoemulsification.
3.
The operated eye is usually treated with a topical fixed combination of steroid (dexamethasone 0.1 %) and antibiotic eye drops qid for 1 week and then tapered over 3 weeks.
4.
In the rare case of an anterior chamber inflammatory reaction, mydriatic eye drops may be added and the topical steroid can be intensified by surgeon’s preference.
Most surgeons discontinue all antiglaucoma medications after the procedure. However, preoperative antiglaucoma medication may be continued and later reduced dependent on the postoperative IOP. When medications are reduced, IOP should be monitored carefully on a regular basis.
After ELT
Ideally, the patients are monitored postoperatively with gonioscopy in addition to IOP and the findings documented as to the number of sites noted patent. In the cases that have been followed in this manner, channels are documented to remain patent years after the ELT procedure, and in some of these patients, goniolens “pumping” can induce blood to appear at the channels, further confirming the patency of these channels into SC (Figs. 8.10 and 8.11).