Fig. 25.1
(a) Anterior segment OCT (AS-OCT) image of the angle in a patient in dark conditions. (b) Angle of the same patient with light shone onto the iris surface. (c) Angle of the same patient with light shone into the pupil. The angle can be seen to be closed with iridotrabecular contact in dark conditions, while this contact is relieved with light (Images courtesy of Ike K. Ahmed, MD)
Finally, as an adjunct to the clinical examination, diagnostic imaging modalities may be extremely useful in angle closure. Anterior segment optical coherence tomography (AS-OCT), Scheimpflug imaging, and ultrasound biomicroscopy (UBM) may all be useful adjunctive modalities in the accurate diagnosis of the underlying factors resulting in angle closure.
When thinking about the proper approach to an angle-closure patient and the most appropriate therapeutic intervention, it is useful to first consider the predominant mechanism of the angle closure. While not independent of each other and commonly angle closure can be multifactorial, the main mechanisms to be considered should be pupillary block, lenticular causes, plateau iris, and retrolenticular.
Treatment
Thought to be the most common form of angle closure, pupillary block refers to the phenomenon of aqueous humor build up in the posterior chamber space between the posterior iris and the anterior lens capsule. This may occur as a result of iris proximity to the anterior lens capsule or a forward position of the lens capsule resulting in apposition and trapping of aqueous humor in the posterior chamber. Without a conduit to allow for equalization of pressure between the posterior and anterior chamber, the mid-peripheral iris is pushed forward in a gradually increasing manner eventually causing iridotrabecular apposition in the “iris bombé” configuration. In order to alleviate the mechanism of pupillary block, relative or absolute, a pathway is required for fluid to exit the posterior chamber and enter into the anterior chamber, most commonly achieved via the creation of a peripheral iris opening to allow for equalization of fluid pressure, typically performed with a neodymium-doped yttrium aluminum garnet (Nd:YAG) laser. In cases where a peripheral iridotomy is not possible for reasons such as corneal edema and complete apposition of the peripheral iris to the cornea, pupillary block may also be relieved by using a needle to lift up the iris from the lens capsule, which can be performed at the slit lamp with the assistance of ophthalmic viscosurgical devices (OVD), providing a way for aqueous humor to exit the posterior chamber into the anterior chamber. Care must be taken not to injure the anterior lens capsule when performing this maneuver.
Although no conclusive clinical study has proven the benefit of laser iridotomy (LPI) for PACS, the relative ease and quickness of the procedure along with the relatively favorable safety profile of the minor procedure has given way to its more common and widespread use in attempts to prevent the more serious and grave consequences of AACG or PACG. Although LPI may be the first step in therapy, it is often insufficient in PAC or PACG to halt the disease process and does not address PAS or anatomical closure of the angle. It has been reported that nearly 1 out of 3 PAC eyes which received LPI continue to have significant ITC after treatment [36–38]. The term plateau iris configuration may be used to refer to eyes which appear to have a deep central anterior chamber with the peripheral iris continuing to appear in close apposition to the trabecular meshwork or have frank ITC. In cases of plateau iris configuration where IOP spikes occur following LPI, plateau iris syndrome may be diagnosed. Although the treatment of plateau iris is not the focus of this chapter and argon peripheral laser iridoplasty remains the standard treatment for plateau iris syndrome after LPI, surgical strategies to deal with plateau iris when combined with lensectomy will be discussed later on in this chapter.
Lenticular causes of angle closure can be a result of many different factors. Increase in lens thickness or lens vault, particularly in hyperopic eyes with smaller anterior segments, weakening of the zonular apparatus resulting in a forward position of the crystalline lens, and lens-induced pupillary block may all be implicated. It is well established that lensectomy widens the anterior chamber angle in ACG eyes as well as those with narrow, occludable angles [39–43]. Furthermore, in both prospective and retrospective studies comparing lens extraction with surgical iridectomy or trabeculectomy in acute and non-acute ACG, lensectomy patients were shown to have decreased postoperative medication requirements as well as a lower rate of complications [44–54].
In one study which randomized AACG patients to cataract surgery versus peripheral iridotomy alone, patients with an IOP >55 mmHg who underwent early lens extraction were found to be less likely to require IOP-lowering therapy [44]. In certain situations, lensectomy may be accompanied by other surgical procedures such as goniosynechialysis to release PAS, endocyclophotocoagulation, or filtration surgery. In one study randomizing 51 medically uncontrolled CACG eyes to cataract surgery alone versus combined phacotrabeculectomy, IOP was found to be lower in the combined surgery group as well as less postoperative dependence on topical medications, but the phacotrabeculectomy group had a significantly higher rate of complications, as well as progression of optic neuropathy [55]. In their study, 14.8 % of lensectomy-only eyes required subsequent filtration surgery.
The same group also performed the same randomized trial comparing phacoemulsification versus trabeculectomy head-to-head in 50 uncontrolled CACG eyes without cataractous lens opacities. No significant difference in IOP reduction between the two groups was found, but the trabeculectomy group required less postoperative medications. However, surgical complications were reported as 46 % in the trabeculectomy group as compared with only 4 % in the phacoemulsification-alone group (P = 0.001) and one third of the trabeculectomy eyes demonstrated cataract development during the 24-month follow-up [56]. Finally, in patients with medically controlled CACG who were randomized to lensectomy alone versus phacotrabeculectomy, there was no statistically significant difference between IOP at 12- and 24-month follow-up and no difference in disease progression rates, and while the phacotrabeculectomy group was on a mean of 0.8 medications less than the lensectomy-alone group, the phacotrabeculectomy group suffered significantly more postoperative complications [57]. When faced with deciding which procedure to most appropriately perform in a patient with ACG, one should consider whether lens extraction is likely to relieve the pre-trabecular meshwork obstruction, allowing for control of the IOP and opening of the angle, with or without medications, before deciding to pursue filtration or combined phacoemulsification and filtration surgery, which, as these studies have shown, result in more postoperative and potential long-term complications for the patient. In certain cases, lensectomy without filtration surgery may be combined with other non-bleb-forming procedures, to be discussed later, which have a more favorable risk profile.
The final consideration in the patient with angle closure is that of retrolenticular causes. This includes situations such as choroidal expansion, malignant glaucoma, ciliary effusions, or any other posterior-pushing mechanism. Although not classically considered in the category of primary angle closure and not within the scope of this chapter, a brief discussion on surgical considerations in malignant glaucoma will also be included in this chapter.
Surgical Technique and Considerations
Lensectomy in the angle-closure eye may present many unique challenges to the surgeon. The difficulties may range from poor visibility due to an edematous cornea, flat anterior chamber, abnormal iris behavior, intumescent lens, and loose or missing zonules to predisposition to malignant glaucoma both intraoperatively and postoperatively.
The surgical approach to the angle-closure patient begins preoperatively. It is ideal if any AACG attack is broken prior to surgical intervention and, as well, the eye as quiet as possible from inflammation with the use of topical steroids or nonsteroidal anti-inflammatory medications. Topical, with or without, the use of systemic medications to obtain as normal an IOP as possible prior to surgery is also advisable. Specular microscopy with a corneal endothelial cell count may be helpful in determining the state of cornea. AS-OCT may provide information as to the amount of anterior chamber space one will have to work with intraoperatively (Fig. 25.2) as well as potentially suggest diagnostic etiologies related to poor zonular support such as ACG due to spherophakia (Fig. 25.3). Finally, UBM imaging may provide a view to the ciliary processes, with anteriorly positioned ciliary processes seen commonly in plateau iris syndrome (Fig. 25.4).
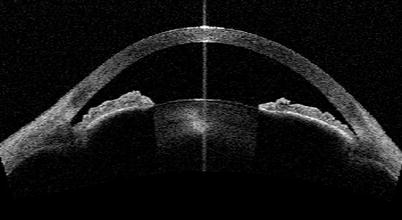
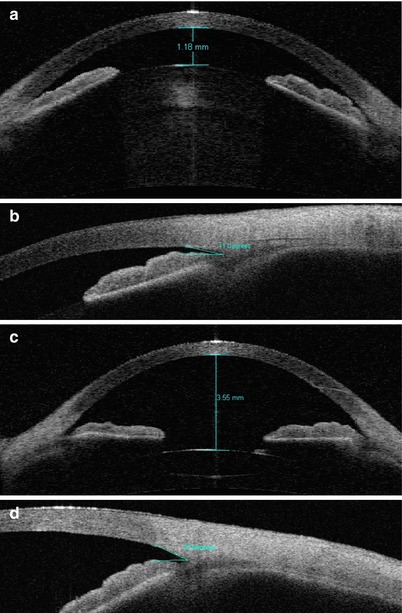
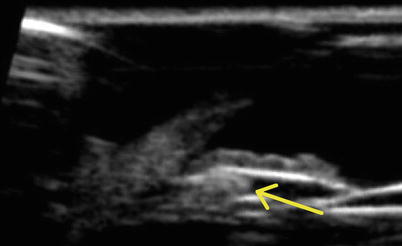
Fig. 25.2
AS-OCT image of a patient with high lens vault and also relative pupillary block seen with a convex iris contour
Fig. 25.3
(a) Spherophakia lens-induced angle closure with anterior chamber depth of 1.18 mm as measured on AS-OCT. (b) Angle view of the same patient. (c) Postoperative imaging of the same patient after lens extraction and goniosynechialysis showing anterior chamber depth of 3.55 mm. (d) Postoperative angle image of same patient (Images courtesy of Ike K. Ahmed, MD)
Fig. 25.4
Ultrasound biomicroscopy image of a plateau iris patient showing anteriorly positioned ciliary processes (arrow) propping up the peripheral iris causing a narrow angle
Intraoperatively, the first objective of surgery is to achieve an adequate view of the anterior segment to effectively and safely perform lens extraction. If the epithelium is edematous preventing an adequate view, topical glycerin may be used, or manual removal of the corneal epithelium is occasionally required. Once an adequate view has been achieved to proceed, the next objective is to protect the cornea, typically most effectively achieved by the use of a dispersive OVD injected into the anterior chamber via a paracentesis incision. Stabilization and deepening of the anterior chamber, often achieved with a cohesive OVD, should then be attained. In the occasional case, the anterior chamber cannot be deepened or formed with OVD, even with a high-viscosity agent such as Healon 5 (Abbott Medical Optics, Inc., Illinois, USA). In such cases, a pars plana tap to reduce posterior pressure can be an invaluable tool and technique in order to allow deepening of the anterior chamber for effective removal of the lens and as well providing a safe space for phacoemulsification and manipulations to occur away from the likely already-traumatized corneal endothelium [58].
The proper technique should involve a localized conjunctival peritomy and light cautery for hemostasis, followed by a careful measurement and marking with a caliper of 4 mm radially posterior to the limbus. A microvitreoretinal (MVR) blade is then used to enter the posterior segment with care taken to aim the blade posteriorly towards the optic nerve, to comfortably avoid the crystalline lens. Without the use of a separate infusion, the automated vitrectomy device is then placed into the posterior segment through the created incision, with care taken to point the guillotine and aspiration ostium posteriorly away from the lens. Vitrectomy with suction is then performed, and within a few seconds and with a very small volume of vitreous removed, sufficient decompression of the posterior segment will have occurred as to produce a dramatic and often surprising increase in the capacity to deepen the anterior chamber (Video 25.2).
Once the anterior chamber has been stabilized, the pupil may need to be addressed prior to lens extraction. Posterior synechiae from the iris to the lens capsule may need to be released, or pupil manipulation and expansion may be required. These maneuvers may be achieved using simple iris hook instruments such as the Kuglen or Lester hooks, pupil dilators such as the Beehler instrument, anterior segment microscissors to perform mini-sphincterotomies, or devices to maintain pupil dilation during surgery such as the Malyugin Ring or disposable iris retractors. Viscodilation with a viscoadaptive OVD is also often a useful adjunct in managing iris in these cases. In some cases, patients with atonic mid-dilated irides, or those with focal atrophy, may benefit from suture pupilloplasty to reduce photophobia and restore a more anatomically physiologic shape for both visual function and cosmesis. This is typically achieved using 10-0 polypropylene suture on a long curved needle to place either multiple interrupted sutures to close focal defects or occasionally a cerclage or partial cerclage suture to close circumferential or large clock-hour iris defects or areas of atonicity. Iris sutures may be tied using the McCannel [59], Siepser [60], any modification of the two, or intraocular microinstrument-mediated tying techniques (Videos 25.3 and 25.4).
In angle-closure eyes, creating a continuous curvilinear capsulorhexis (CCC) may be challenging, as these patients often have a lens or anterior capsule that is vaulted forward. As a result, an anterior CCC has the tendency to run out peripherally towards the lens equator. The use of high-viscosity OVD agents may be employed to flatten the anterior capsule, and as well, erring on the side of making the CCC slightly smaller may be useful strategies. If the lens cortex is hydrated, white, and intumescent, prior to commencing the CCC, a short hypodermic needle on a syringe half filled with balanced saline solution may be utilized to puncture the anterior capsule, immediately aspirating and decompressing the internal contents of the capsular bag to decrease the amount of forward pressure on the anterior capsule (Video 25.5). Should the CCC begin to stray peripherally during its creation, a tear-in technique is very useful to rescue the capsulorhexis (Video 25.6) [61]. If zonular issues are present in an angle-closure patient undergoing cataract extraction, a CCC is critical to permit the use of capsular tension devices. Without an intact CCC, capsular tension support devices are very challenging to use and may in fact be detrimental [62, 63].
Zonular weakness is frequently encountered in angle-closure eyes, from mild laxity allowing or causing the lens to vault forward into a configuration causing pupillary block or simply an overall forward position of the lens-iris apparatus with a crowded anterior segment. Occasionally the zonular laxity can present in the extreme and severe forms such as in microspherophakia as the cause of angle closure. While zonular weakness may occasionally be elucidated at the preoperative examination, this may be very subtle or difficult to observe in the angle-closure eye, especially after an AACG attack. Furthermore, patients with frank phacodonesis and lens movement typically will have enough space, even if only intermittent between saccades, between the iris and lens capsule to allow aqueous humor to pass from the posterior to the anterior chamber.
Intraoperatively, several signs may suggest moderate or severe zonulopathy: capsular wrinkling when attempting to puncture the anterior capsule, difficulty puncturing the anterior capsule, ovalization of the CCC, movement of the entire lens during creation of the CCC, or tilting or lens movement during phacoemulsification [64]. In angle-closure patients, capsular tension devices may serve to stabilize weak zonules or support an area of focalized weakened zonules, distribute forces along the capsular bag circumference evenly, expand the equator of the capsule, recenter a mildly subluxed capsular bag, and keep the capsular bag in an anatomically acceptable position. Although a small series, one study has shown with UBM postoperative imaging that implantation of a CTR placed the bag equator and CTR in an anatomically favorable position between the IOL haptics and the ciliary body without posterior iris touch [65]. Other studies have also suggested similar findings [66].
When confronted with weak zonules, the first decision to be made is whether a mere capsular tension ring will be sufficient to support the capsular bag. A CTR is suitable for use in cases where mild generalized zonular weakness or a localized focal zonulolysis area of less than four clock hours is suspected. As well, where no overt or gross lens subluxation is present, even in cases of suspected progressive zonulopathies, a CTR may be sufficient [67].
If the zonular weakness is in excess of these criteria, it is likely that more than a CTR alone will be required to stabilize the capsular bag. If more extensive support is required, one can select a Cionni-modified CTR (M-CTR) which consists of a CTR with one or two eyelets for suturing positioned 0.25 mm anterior to the equatorial ring or an Ahmed capsular tension segment (CTS). While the M-CTR encompasses the entire circumference, it is not injectable and must be manually inserted into the capsular bag.
This may be quite challenging especially in cases where the assistance of the device is required before the capsular bag contents are removed and may in fact damage zonules further. Also, it is ideal to position the eyelet for suturing into the area of greatest zonular weakness or absence, something which may require even further manual manipulation and rotation once the device is in the capsular bag. In these cases, an Ahmed CTS may be used, which is composed of a 120° arc length PMMA ring segment with a 5 mm radius of curvature. Like the M-CTR, it has an anterior positioned eyelet for suturing to the sclera. The CTS is more relatively easily maneuvered in the eye and into the capsular bag, without the need for rotational movements, which may further damage existing zonules. Further, because it is designed to slide into the capsular bag, it is more readily placed into the particular quadrant or zone where it is most needed and, with caution, can be used in cases of a discontinuous CCC or a posterior capsular tear.
The main body of the device is designed to sit in the capsular equator with the central eyelet remaining anterior to the anterior capsule. It can easily be placed prior to cataract extraction and may be supported intraoperatively with an inverted iris retractor through a paracentesis incision and sutured later on after the cataract has been removed. While the CTS provides focal support transversely to the scleral wall, it may be used in conjunction with a CTR to provide circumferential support and distribution of zonular tension. Finally, multiple CTS may be used if the zonular weakness or absence is profound. These may be sutured to the sclera through an ab externo technique using a 9-0 polypropylene suture or larger-caliber suture such as GORE-TEX expanded polytetrafluoroethylene (ePTFE) material (W.L. Gore & Associates, Inc., USA) for greater longevity and reduced suture breakage risk (Video 25.7) [67].
Once the decision has been made to employ the use of a CTR in surgery, the decision must be made whether to place it in the capsular bag prior to or after phacoemulsification. There are advantages and disadvantages to each approach. If there is suspicion of significant zonular weakness from either preoperative evaluation, intraoperative signs, or a concern for the capsular equator collapsing centrally, then consideration should be given to placing the CTR early on, prior to lens removal. The technique to achieve this involves careful and thorough viscodissection creating a plane between the capsular bag and the cortical material. A diligent viscodissection will prevent any cortical lens material entrapment by the CTR when placed prior to phacoemulsification. If moderate or severe zonular weakness is encountered, iris retractors may be used and placed gently on the CCC to stabilize the capsular bag while viscodissection and CTR injection is performed (Video 25.8). The CTR may be injected also after a CTS has been placed if this was required (Video 25.9).
After successful insertion of the CTR, hydrodissection and hydrodelineation may proceed as per the surgeon’s usual technique. The main advantage of early placement includes expansion of the capsular equator alleviating the concern of equatorial collapse and inadvertent bag injury during phacoemulsification. As well, the expanded capsular equator may serve in certain cases to barricade any vitreous that would otherwise be able to prolapse forward in an area of zonular dehiscence. In some cases, without early capsular tension device placement, phacoemulsification would be very challenging to achieve uneventfully in a very mobile lens and capsular bag complex.
While advantageous in early stabilization of the zonules, some disadvantages of early placement include the potential to injure or dehisce more zonules because of rotational forces transmitted to the zonular apparatus during CTR insertion. The potential for injury to the capsular bag itself during insertion, the potential entrapment of cortical material if viscodissection is not done properly making for challenging cortical removal, and the possibility of posterior dislocation of the CTR into the posterior segment should a posterior capsular tear occur during subsequent phacoemulsification. Finally, as the CTR expands the capsular equator and places tension on the posterior capsule, a taut capsule may be more easily torn or appear to move the posterior capsule into a more forward configuration during the latter stages of phacoemulsification and irrigation/aspiration.
Injection of a CTR late after the contents of the capsular bag have been removed can be advantageous in ease of insertion, but in cases where zonulopathy is moderate or severe, the capsular bag equator may collapse increasing the risk of inadvertent injury potentially eliminating the possibility that a CTR can even be considered.
It is worth noting that in angle-closure eyes, and eyes with suspected zonulopathy, direct chopping lens disassembly techniques such as phaco chop have some advantages over techniques such as divide and conquer. Phaco chop has been shown to dissipate significantly less phaco power and time into the eye [68, 69], being advantageous to the corneal endothelium [70] and other anterior segment structures such as the trabecular meshwork, which both may be already compromised in angle closure. Further, in the divide and conquer technique, a downward pressure is transmitted onto the zonular apparatus during sculpting maneuvers, which may further injure or break already-weakened zonules. Vector forces in phaco chop techniques, when performed properly, are transmitted endocapsularly with shearing or cracking of the lens material and minimal tension placed on zonules.
Once the crystalline lens material is removed and all required capsular tension devices have been placed properly, an intraocular lens (IOL) can be inserted, preferably into the capsular bag if sufficiently intact. Although different IOL models and designs may be used, it is the author’s experience that a soft foldable acrylic one-piece IOL unfolds slowly and gently in a manner which is gentle on the zonules and is the easiest to control in terms of endocapsular placement, rotation, and manipulations.
In the case of a non-intact posterior capsule, a three-piece IOL with thin polymethyl methacrylate, polypropylene, or polyimide haptics may be placed in the ciliary sulcus with posterior optic capture through an intact CCC for added stability. Although certainly possible to perform successfully, caution is advised when placing IOLs in the ciliary sulcus of eyes with crowded anterior segments. The bulky acrylic haptics such as those found on the one-piece acrylic IOL platforms should never be placed in the ciliary sulcus as they will chafe the posterior iris surface resulting in complications such as uveitis-glaucoma-hyphema syndrome. Finally, if capsular support is absent and not viable for IOL support, the iris claw IOL (Ophtec BV, Netherlands) may be used if the anterior chamber depth has been sufficiently improved after lens extraction and in the presence of a healthy corneal endothelium [71–73]. Should corneal or anterior chamber depth criteria not be met, a three-piece IOL may be fixated to the posterior chamber using the scleral-glued technique [74].
Combined Surgery
In certain clinical situations, the decision may be made to combine lens extraction with adjunctive glaucoma procedures including endocyclophotocoagulation (ECP) and goniosynechialysis (GSL), or even in cases with advanced disease where it is felt that lens extraction alone with adjunctive medications may not achieve the target IOP, filtration surgery including trabeculectomy, Ex-PRESS mini shunt, and long tube shunt implantation may be considered concurrently. Although filtration and tube shunt surgery are covered elsewhere in this book, a brief discussion of ECP and GSL will be included.
Although lens extraction may alone be completely therapeutic in angle closure due solely to lens vault, phacomorphic ACG, or lens-induced pupillary block, the angle may remain narrow after lens extraction alone, this being particularly so in cases of plateau iris [75]. In cases of angle closure undergoing cataract surgery where the primary cause is thought to be plateau iris configuration or where a mixed mechanism of lens-related causes and plateau iris is felt to be contributory, ECP may be considered as a way to widen the angle and increase the separation between the peripheral iris and the trabecular meshwork. While traditional ECP techniques have been reported as a treatment for refractory open-angle glaucoma, ECP may be a very effective tool in angle-closure glaucoma as well. In a technique that has been termed “endocycloplasty” [76], the diode laser beam and energy are directed and applied to the posterior aspect of the ciliary processes, pulling the entire ciliary process posteriorly away from the posterior iris surface. This allows the peripheral iris to fall back posteriorly away from the trabecular meshwork and angle.
This treatment is typically performed for 270° arc length via the same incision by which the phacoemulsification or lens extraction was performed. It is important to note that in this technique, the location of the laser application on the tail of the ciliary process is critical to its success. Treatment at the posterior tail of the process directs the entire ciliary process including the anterior head to shrink posteriorly.
The treatment should shrink and whiten the ciliary process, but care be taken to attempt to avoid “popping” as this may lead to increased postoperative inflammation and breakdown of the blood-aqueous barrier (Video 25.10). Although further study is required, the early results of this technique have appeared very promising in improving angle configuration (Figs. 25.5 and 25.6 – Visante post-ECPL, UBM post-ECPL).
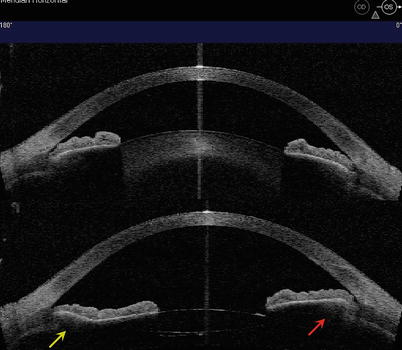

Fig. 25.5
Noncontact AS-OCT image of anterior chamber in an eye after lens extraction and endocycloplasty (ECPL). Because of the 270° treatment performed during surgery, the temporal angle (red arrow) remains narrow with the peripheral iris propped up by the anteriorly positioned ciliary processes, while the nasal angle (yellow arrow) is dramatically opened with the peripheral iris able to fall back from the angle and trabecular meshwork with the ciliary processes shrunken posteriorly from the treatment (Image courtesy of Ike K. Ahmed, MD)
Fig. 25.6
Ultrasound biomicroscopy of the same patient as seen in Fig. 25.5 showing again the temporal ciliary processes (red arrow) and the shrunken nasal ciliary processes (yellow arrow)
While lensectomy and even ECPL may deepen the anterior chamber, if peripheral anterior synechiae are present, more may need to be done for the control of IOP in synechial angle-closure patients. Goniosynechialysis has been reported to be effective and safe in the reduction of IOP [77] and even more so when combined with lens extraction [78–81]. UBM imaging has also shown the restoration of an open anterior chamber angle after GSL [82]. Although controversial, the success of GSL may be dependent on the duration of the presence of PAS. Existing data from studies which showed efficacy of GSL suggested that it is best performed in cases where PAS has been present for 6 months or less, although when presented with an ACG, it may be difficult to know how long PAS have been present and no data currently exists directly comparing the efficacy of GSL when performed at varying time points of PAS presence. However, given the relatively favorable safety profile of GSL, it may be beneficial to consider performing GSL prior to making the decision to proceed with more invasive and higher-risk filtration surgery, even if it is suspected that the PAS have been present for greater than 6 months.
GSL may be performed with varying techniques, but the author’s preferred technique is under gonioscopic visualization with the use of anterior segment microinstrumentation to precisely grasp the peripheral iris tissue and view the angle structures as the PAS are released (Video 25.11). In cases where the cornea does not permit an adequate view of the angle via a gonio mirror, endoscopic visualization may be utilized to assist in performance of GSL (Video 25.12) [83]. It should be noted that it is common for lens extraction to be performed in conjunction with both ECPL and GSL, as a very useful technique to release PAS, maximize angle space, and minimize risk of PAS recurrences.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


