Fig. 23.1
Current model of SOLX Shunt, GMS Plus, and the prior model GMS
The initial studies were done with the earlier model, Gold Micro Shunt, GMS, which was a non-valved flat-plate drainage device made from 24-karat medical-grade (99.95 %) gold. The shunt was 3.2 mm wide and 5.2 mm long and weighs 6.2 mg. It had a long rectangular shape, with rounded edges and finlike tabs on the distal end for anchoring the device in the suprachoroidal space. The aqueous entered the shunt at the proximal end, where 60 holes (100 mm in diameter) and one 300-mm through hole were present. The distal end provided drainage through the microchannels of the fluid from the AC into the suprachoroidal space. Nineteen channels were present, of which 10 were closed and 9 were open, with a lumen width of 24 μ and a height of 50 μ. The posterior end of the shunt contained a grid of 117 holes (110 mm in diameter) on each side of the implant to allow a free flow of the fluid from the device. The proximal and the distal ends also contained 12 and 10 additional 50-mm lateral channels, respectively, in order to increase flow [13].
The latest model, GMS Plus, is 3.2 mm wide and 5.5 mm long, weighs 9.2 mg, and has larger channels, which are essentially like posts and add to the tensile strength of the device. This model also has five central fixation holes for easier implantation (Fig. 23.2).
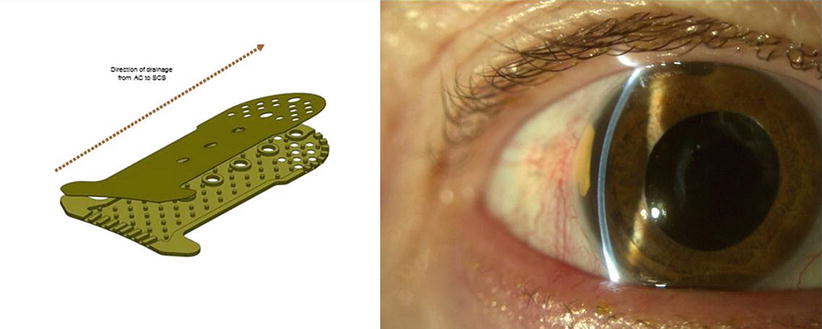
Fig. 23.2
GMS Plus implanted in temporal quadrant of the eye
Indications
Refractory glaucoma
Failure of a previous glaucoma surgical intervention
Mechanism of Action
Enhancement of the aqueous filtration across the sclera may be one of the possible outflow pathways exploited by the shunt. The hypoechogenic space around the device detected by 20-MHz ultrasound and AS-OCT suggests increased flow through the supraciliary and suprachoroidal space [13]. From the suprachoroidal space, the aqueous humor can drain into the choroidal vascular system or permeate through the sclera.
Surgical Technique
Patients can be operated on under local anesthesia using either a sub-Tenon or a peribulbar injection. A bridle suture is placed around the superior rectus muscle; alternatively, a corneal traction suture can be placed at 12 o’clock. The gold shunt can be implanted in any quadrant, but the scleral tissue in the area of surgery should be healthy. Temporal quadrant is the most suitable quadrant. Furthermore, the angle in the area of intended implantation should be open and free of any peripheral anterior synechia.
A fornix-based conjunctival flap is fashioned, followed by meticulous cautery of episcleral vessels. A 4 mm (wide) by 3.5 mm (long) scleral flap about 90 % in depth is created. Dissection is done up to clear cornea and scleral spur is identified. After measuring 1.5 mm posterior from scleral spur, a 3-mm-long mark at both scleral spur and 1.5-mm point is made. These steps should be performed with the eye pressurized to facilitate the scleral dissection.
A full-thickness incision 3 mm wide is made into the suprachoroidal space. A cyclodialysis spatula is used to ensure that wound is 100 % open end to end. This is followed by injection of a small amount of viscoelastic into the suprachoroidal space. Then a superficial ledge incision (approximately 50 μm) is created, and anterior chamber is entered with a 2.85-mm keratome, parallel to the iris.
The device is checked for mobility. Sclera is grasped with a .12 forceps just outside of the flap for countertraction.
The flared distal end of GMS Plus that is inserted into the AC allows for consistent fixation and more reproducible placement in the angle.
“Shoulders” of the device are passed through the incision site one at a time. Using either a cystotome needle or a Sinskey hook, the device is pushed forward out of the inserter using the positioning holes on the gold shunt. Once the tail of the device clears the suprachoroidal space incision site, the lower lip of the wound is grasped and lifted. Then the implant is pulled gently into the suprachoroidal space.
It is better to go hole by hole like climbing a ladder. The shoulders of the device will stop once they get to the angle. It is best to have the device as deep into the angle as possible. The scleral incision is closed with 10-0 nylon sutures and the conjunctiva is closed at the limbus. It is best to have no flow from flap; however, if there is a small amount of egress and a small bleb forms, realize it is only temporary and will resolve. If device is pushed out of the angle during suturing, simply insert a cyclodialysis spatula through the paracentesis port and push it back into the angle.
Advantages
Gold is known to be biocompatible, with no long-term toxicity in the human eye.
No external filtering bleb.
Chances of hypotony less.
Reduced probability of developing endophthalmitis due to the exposure to the implant.
Absence of conjunctival erosion.
Absence of extraocular muscle imbalance.
Disadvantages
Presence of a permanent implant in the anterior chamber and suprachoroidal space
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


