Sensory: tenderness, itching, visual changes
Motor: ptosis, lagophthalmos
Structural: visible or palpable lesion, change in symmetry
Functional: keratopathy or tearing
Secondary: pigmentation, lymphadenopathy
1.2.2 Rate of Onset
Rapidity and progression help characterize the pathology. Most symptoms from eyelid tumors develop over weeks to months, but associated hemorrhage, infection, and inflammation may be acute. Both benign (e.g., angiomas, papillomas) and malignant (e.g., cutaneous malignancies, metastases) eyelid tumors can produce hemorrhage. Any eyelid tumor that blocks lacrimal outflow or causes diminished cutaneous integrity can result in infection. Several eyelid tumors, such as keratoacanthoma, may be associated with a significant inflammatory reaction.
1.2.3 Past Medical History
Because the majority of eyelid neoplasms are epidermal in origin, the past medical history should focus on risk factors for epidermal malignancy. Information should be obtained regarding family history of cutaneous malignancy, skin type, freckle density, eye color, hair color, and prior history of skin cancer. Patients of Celtic or Scandinavian descent with red hair, blue eyes, and fair skin carry a greater risk for cutaneous malignancy [1, 2]. The history should also include tobacco use, prior radiotherapy, sun exposure, and similar growths elsewhere on the skin.
1.3 Examination
The physical examination of an adult with suspected eyelid neoplasia does not end with direct visualization of the lesion. It should include a comprehensive inspection of the eyelid, ocular adnexa and orbit, eye, and other cutaneous lesions described in the history. Underlying conditions that may make reconstruction more challenging should be noted, including prominent globe, midface ptosis, hypoplastic orbital rim, lack of cutaneous or tissue redundancy, previous scarring from cutaneous malignancy repair or other surgery, lagophthalmos, trichiasis, dry eye syndrome, and blepharitis.
1.3.1 Eyelid Examination
The patient should point out smaller lesions to the examiner using a hand mirror. The entire face should be evaluated to note Fitzpatrick skin type and any other cutaneous lesions. The eyelid examination should describe the appearance of the lesion, any associated anatomical deformities, and the results of palpation. The dimensions should be measured using a ruler or slit lamp beam. The eyelid examination should focus particularly on signs of malignancy, including telangiectasia, nodularity, pearly translucency, ulceration, bleeding, crusting, irregularity of the eyelid margin, meibomian gland effacement, and loss of cilia (Fig.1.1; Box 1.2). Palpation results should describe the mobility of the lesion, as well as any fluctuance or associated tenderness. Color changes and irregularities should be noted.
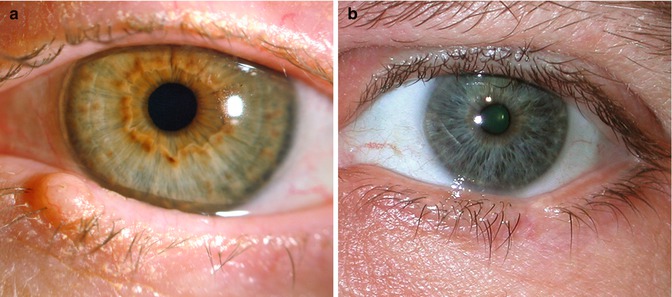
Fig. 1.1
Photograph of lower eyelid shows a benign eyelid nodule without loss of lashes (a) and loss of eyelid tissue with cilia loss secondary to a malignant tumor (b)
Levator excursion, orbicularis function, and corneal sensation should all be tested. Any lagophthalmos should be measured and noted. Horizontal eyelid laxity, blepharoptosis, cutaneous insufficiency, and other preexisting eyelid malpositions and conditions should be noted, as they may challenge repair and will affect the reconstruction design. In addition, patients that relate these preoperative conditions to eyelid tumor surgery in the follow-up period can be reminded of the preoperative findings.
1.3.1.1 Box 1.2: Signs of Malignant Eyelid Tumor
Telangiectasia |
Nodularity, pearly translucency |
Ulceration, bleeding, crusting, margin notch |
Loss of cilia |
Effacement of meibomian gland orifice < div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|