Examination of the Afferent Visual System
The purpose of the neuro-ophthalmic examination is to detect visual abnormalities (acuity or visual field) and to determine if they are due to neuro-ophthalmic disorders. The neuro-ophthalmic examination should be preceded by a thorough history of the presenting complaint, a detailed past medical history, social history, ocular history, list of medications, and review of systems. These procedures should be followed by a comprehensive ophthalmologic assessment that may identify non-neuroophthalmic causes for the visual disturbance (e.g., microhyphema as a cause of transient visual loss). Only the parts of the examination that are directly relevant to the neuroophthalmic examination will be discussed in this chapter.
VISUAL ACUITY
Patients can have decreased acuity from a variety of causes. The starting point of the neuro-ophthalmologic examination is to determine the best-corrected Snellen acuity in each eye separately. A variety of targets can be used to test visual acuity (VA) at distance (Fig. 1-1). Several methods may be used to determine if the VA can be improved and what is the likely cause of the poor vision.
• Refraction
• Pinhole: a series of pinholes measuring 2 to 2.5 mm are placed before each eye as its fellow is occluded (Fig. 1-2). Improvement in acuity with pinhole indicates a refractive or media (e.g., cataract) cause of decreased vision.
• Bright light near vision. An improved near acuity with appropriate reading glasses and a bright light indicates that the cause of decreased vision is refractive or cataractous.
• Potential acuity devices: a variety of apparati project images (Snellen optotypes or lines) directly on the retina, thus by-passing any refractive or media cause for decreased vision.
Improvement in VA to normal with any of these methods obviates the need to search for a neuro-ophthalmic cause of visual loss. Failure to improve the acuity, on the other hand, means further investigations for other causes, including neuro-ophthalmic diseases, are in order.
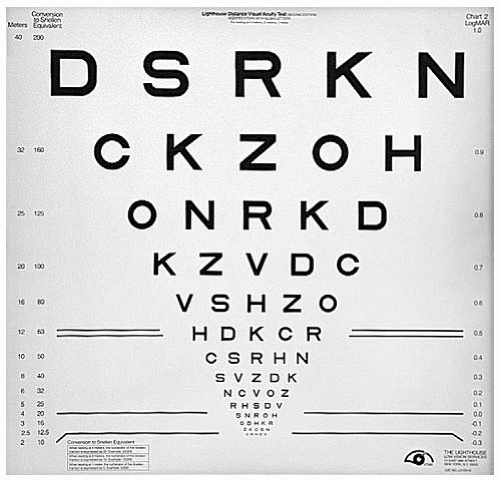 FIGURE 1-1. The retro-illuminated Bailey-Lovie chart is placed at a distance of 4 m from the patient. |
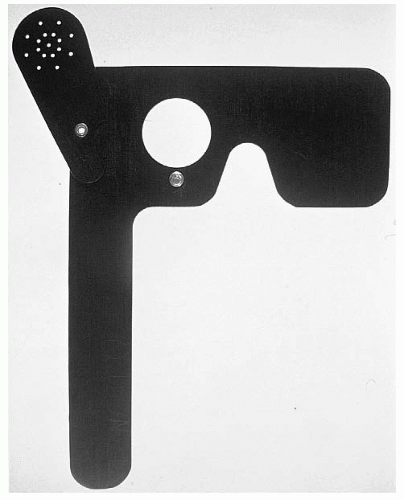 FIGURE 1-2. Occluder with pinholes that can be rotated into position in lieu of performing a refraction. |
COLOR VISION
The purpose of color vision testing is to detect acquired unilateral or bilateral color loss, which occurs with optic neuropathies, disorders of the optic chiasm, and, more infrequently, with some occipital disorders (see Chapter 7). Most optic neuropathies produce marked loss of color perception; whereas in retinal or macular disease, the acuity may be poor but color vision is relatively preserved. Acquired dyschromatopsia is a useful clinical finding to support the presence of an optic nerve disorder.
It is important to remember to test each eye separately and to test color vision prior to testing pupils as the bright light can produce transient color desaturation. Color vision may be tested with the following:
• Ishihara pseudoisochromatic or Hardy-Rand-Rittler (HRR) plates: the patient is asked to identify the numbers displayed using each eye in turn (Fig. 1-3). This tests predominantly red-green color deficiencies. The number of correctly identified plates with each eye is recorded. The control plate can be read if the VA is better than 20/400. If the patient does not see the control plate, it is pointless testing the remainder of the plates. If the patient only sees the control plate then this is recorded as “Control only”.
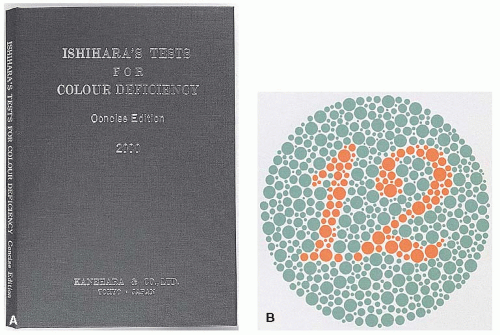 FIGURE 1-3. A. Ishihara pseudoisochromatic color-plate book. B. The first plate (12) is the control plate and is recognizable except with profound visual loss. |
• Farnsworth panel D15: This panel has 15 caps with colors that are to be placed in order, starting with the closest hue to the reference cap, until all 15 are placed in sequence. A number on the back of each cap indicates its correct position in a normal sequence. This test identifies tritan (blue), deutan (green), and protan (red) color anomalies.
• Farnsworth Munsell 100 hue: This tests actually consists of 85 (not 100) caps in four boxes (Fig. 1-4) and is similar in concept to the D15 test. The 100-hue test can determine
the severity as well as the axis of color anomaly. The Farnsworth Munsell 100 most thoroughly assesses color vision, but because it is tedious and cumbersome, it is not usually performed as a first-line color vision test.
the severity as well as the axis of color anomaly. The Farnsworth Munsell 100 most thoroughly assesses color vision, but because it is tedious and cumbersome, it is not usually performed as a first-line color vision test.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


