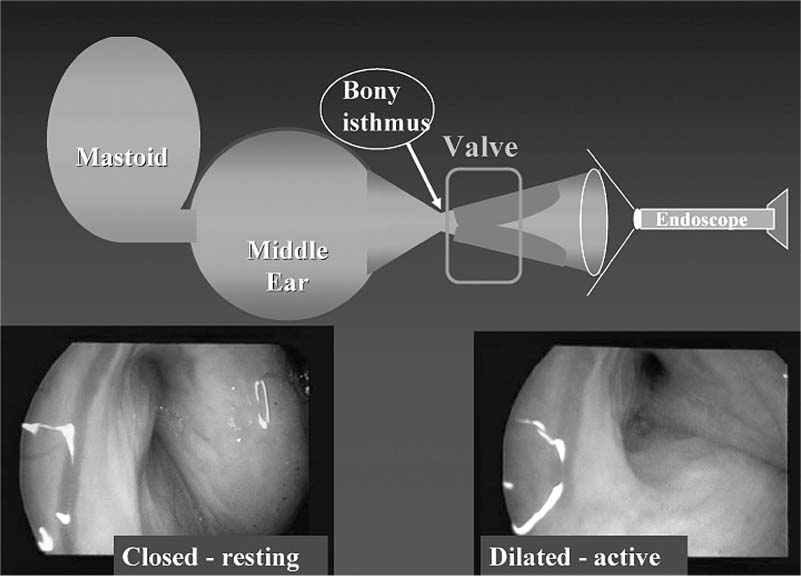
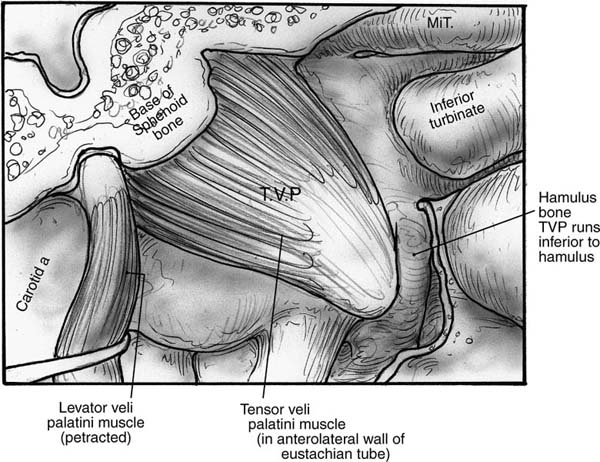
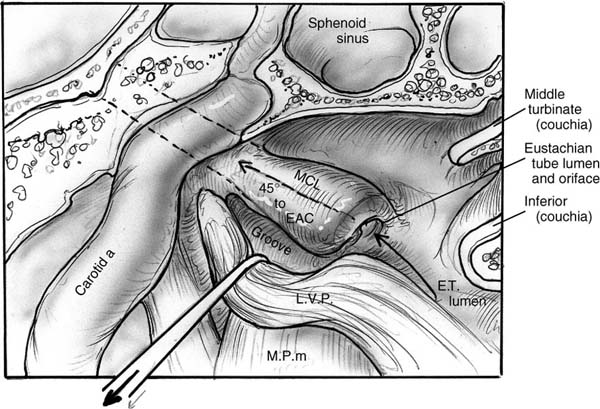
10 Eustachian Tube Function and Dysfunction The eustachian tube is a dynamic conduit that connects the middle ear with the nasopharynx. It contains secretory, ciliary, and dilatory functions. The eustachian tube regulates air pressure within the middle ear and mastoid system, clears material out from the middle ear, and prevents the reflux of material and sound from the nasopharynx into the ear. The tube contains a physiologic valve that is closed in the passive resting position and is dilated open by active muscular exertion. There is no generally accepted definition for eustachian tube dysfunction, but it is commonly taken to imply an inadequate ability to open the tubal valve. When the valve fails to function properly, numerous consequences may occur within the middle ear, with the most common of these being otitis media (Fig. 10–1).1 In the following description of the anatomy of the eustachian tube, the word proximal refers to the nasopharyngeal side of the tube and distal refers to the direction of the middle ear. The cross-sectional diameter of the tubal lumen can be divided into a superior and inferior half and an anterolateral and posteromedial half. The eustachian tube measures about 31 to 38 mm in length in a normal adult, a size that is typically achieved by age 7. The infant eustachian tube measures about 14 to 19 mm.2 The distal one third of the eustachian tube, the bony portion, is roughly funnel shaped. It extends from the middle ear and tapers to the narrowest portion of the entire length of the tube, which is called the isthmus, and lies just distal to the bony–cartilaginous junction. It is lined with a thin layer of cuboidal respiratory epithelium3 and is essentially a bony rigid tube that is normally patent.4 The proximal two thirds of the eustachian tube, the cartilaginous portion, comprise the pharyngeal portion, which consists of a cartilaginous skeleton with attached peritubular musculature that functions to dilate the tube. The lumen is lined with respiratory epithelium that in the superior half is cuboidal and similar to the epithelium in the bony portion. The epithelium in the inferior half is more columnar respiratory epithelium with additional ciliated and secretory elements. The histologic differences suggest that the superior half of the tubal lumen may serve principally a ventilatory function, and the inferior half, with its increased mucosal folds and ciliated cells, is more likely important for mucociliary transport.5 The soft tissue lining within the tubal lumen consists of the mucosa and the submucosa containing lymphatics and fat. In its relaxed state, the tensor veli palatini muscle adds additional bulk to the anterolateral wall. The cartilaginous skeleton of the eustachian tube is a single piece of cartilage rigidly fixed along its superior aspect to the basisphenoid bone. The medial aspect of the cartilage protrudes into the nasopharynx and is referred to as the medial cartilaginous lamina (MCL). It provides the skeleton for the torus tubarius, also known as the posterior cushion or posterior medial wall of the eustachian tube. The medial cartilaginous lamina is broad and thick at the nasopharyngeal and tapers as it progresses distally toward the bony cartilaginous junction part and becomes rigidly fixed. The lamina is quite mobile in its proximal nasopharyngeal end and medially rotates during tubal dilation. The lateral cartilaginous lamina (LCL) is also referred to as the hook or “J” portion due to its small tail that protrudes into the tubal lumen and is visible as a longitudinal ridge along the superior aspect of the tubal lumen. The lateral cartilaginous lamina does not move because it is quite short and fixed to the basisphenoid bone (Fig. 10–2). Figure 10–1 Schematic of the eustachian tube valve. (See Color Plate 10-1) The tensor veli palatini (TVP) muscle originates from the basisphenoid bone and lateral cartilaginous lamina (Fig. 10–3). Dilator tubae muscle fibers are extensions of the TVP that originate along the anterolateral membranous wall of the tube and blend in with the rest of the TVP belly. The TVP is a flat, fan-shaped muscle with broad origins. It runs longitudinally along the length of the cartilaginous eustachian tube and tapers to run under the hamulus of the palatal bone and then inserts into the soft palate. The relaxed bulk of the TVP causes a bulge into the lumen of the eustachian tube and assists in closure of the lumen. Contraction of the TVP puts laterally directed tension on the membranous wall to dilate the tubal valve into the open position. Figure 10–2 Left cartilaginous eustachian tube in a cadaver dissection viewed from the nasopharyngeal orifice. MCL, medial cartilaginous lamina; L, lumen of the eustachian tube; TVP, tensor veli palatini muscle. (From Poe DS, Metson RB, Kujawski OB. Laser eustachian tuboplasty: a preliminary report. Laryngoscope 2003;113:583–591, with permission.) (See Color Plate 10-2) Figure 10–3 The tensor veli palatini (TVP) muscle. The levator veli palatini muscle (LVP) is a round-bellied muscle that looks like a sling extending between the base of the temporal bone at the bony eustachian tube and runs under a groove in the inferior aspect of the medial cartilaginous lamina as well as the membranous floor of the eustachian tube to insert into the palatal musculature (Fig. 10–4). Contraction of the LVP raises the soft palate and medially rotates the medial cartilaginous lamina. The cartilaginous portion of the eustachian tube is normally closed in its resting state. Muscular contractions initiate rotational movements of the cartilaginous framework and generate tension in the anterolateral wall to create active dilation of the lumen and transient opening. The valve refers to the roughly 0.5-cm-long segment of the cartilaginous tube just proximal to the isthmus where the mucosal surfaces contact each other in the closed position.6 There are four peritubular muscles: TVP, LVP, salpingopharyngeus, and tensor tympani. The TVP is thought to be the principal dilator of the tubal lumen based on studies in which the muscle was either stimulated7 or paralyzed with Botox injections in monkeys.8 Endoscopic observations suggest that the LVP muscle may play a more important role in tubal dilation in humans.9,10 The differences between the infant and adult eustachian tubes are summarized in Table 10–1. One of the most important differences is the shorter length of the infant tube. Bluestone11 has pointed out that the physics of a shorter eustachian tube may facilitate reflux of nasopharyngeal material into the middle ear. The eustachian tubes have been shown to be statistically shorter in young children with cleft palate11 and Down syndrome (trisomy 21).12 Additionally, temporal bone histology in children with cleft palates demonstrated the absence of anatomic obstruction and the presence of numerous abnormalities in the TVP muscle and tubal cartilage.11 Neonates with cleft palate have been demonstrated to have small cross-sectional areas of the eustachian tube lumen13 and hypoplastic LVP muscles.14 Figure 10–4 The levator veli palatini (LVP) muscle. EAC, external auditory canal; MCL, medial cartilaginous lamina.
Eustachian Tube Anatomy

Eustachian Tube Development
Infant | Adult |
|---|---|
14 to 19 mm | 31 to 38 mm by age 7 |
10 degrees from horizontal plane | 45 degrees |
TVP–cartilage angle variable | TVP–cartilage angle consistent |
Less cartilage cell density | Increases through puberty |
Thin Ostmann’s fat pad | Fat increases through child hood |
More mucosal folds | Folds decrease in childhood |
Decreased elastin (floppy tube) | Elastin increases in childhood |
TVP, tensor veli palatini.
Adapted from Bluestone CD. Eustachian tube function and dysfunction. In: Rosenfeld RM, Bluestone CD, eds. Evidence-Based Otitis Media. Hamilton, Ontario: BC Decker; 1999, with permission.
Eustachian Tube Function (Physiology)
The eustachian tube has three principal functions: aeration of the middle ear and mastoid system, clearance of material from the middle ear, and prevention of reflux of material or sound from the nasopharynx.
It is believed that intermittent brief tubal dilation is the principal mechanism for equilibration of middle ear pressure with the ambient atmosphere. Unconscious dilation of the tube occurs throughout the day, usually through a swallow or yawn, and it does not accompany every swallow or yawn. Chemical and baroreceptors within the middle ear are thought to provide autonomic nervous system feedback to influence the frequency of involuntary eustachian tube opening.15,16 Tubal dilation has been documented to occur in normal subjects ~1.4 times per minute during the daytime with the duration of opening averaging 0.4 seconds.17 The frequency of tubal opening is substantially reduced during sleep.
Fluid and middle ear secretions are cleared by a combination of muscular pumping action associated with the tubal closing process3 and by mucociliary activity.1 The pumping action drives material proximally from the isthmus toward the nasopharyngeal orifice during tubal closure because the valve closes first adjacent to the isthmus, and mucosal closure propagates proximally. It is believed that the pumping action may be important in aiding expulsion of low viscosity fluids from the middle ear and in preventing reflux during swallowing. High-viscosity fluids are more likely expelled through mucociliary clearance.18
Reflux of nasopharyngeal material and sounds into the middle ear is limited or prevented by the closed valve of the resting pharyngeal eustachian tube and by the trapped volume of gas in the middle ear and mastoid, which creates a “gas cushion.”1
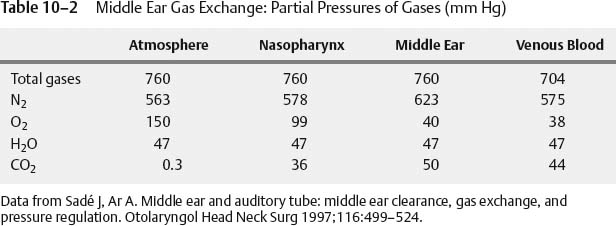
Middle Ear Gas Exchange
Middle ear gas exchange through the mucosa is another mechanism contributing to the composition of middle ear and mastoid gases. There is a steady exchange of gas that depends on diffusion properties, mucosal factors, vascular system factors, and the partial pressures of the gases within the middle ear, tissues, and vascular system (Table 10–2). Upon swallowing with tubal dilation, middle ear pressure should be equal with atmospheric pressure, which would be 760 mm Hg at sea level under standard conditions. Venous blood may average 704 mm Hg, and there is a large gradient between the partial pressure of nitrogen in the middle ear and venous blood. Nitrogen appears to selectively accumulate within the middle ear space, and the availability of nitrogen is dependent on eustachian tube ventilation.19
There will be a steady diffusion of gases from the middle ear and mastoid into the mucosa and surrounding venous blood, creating increasingly negative pressure in the middle ear and mastoid space until the eustachian tube opens again. Failure of the tubal opening results in further increases in negative pressure until some consequence occurs such as development of a serous transu-date, tympanic membrane retraction with atelectasis of the middle ear space, increasing atelectasis with cholesteatoma formation, or tympanic membrane perforation. Ordinarily the middle ear is maintained with a slight negative pressure between 0 and 50 cm H2O using the pressure units employed by tympanometry.
There is a difference between the solubility constants of the various middle ear gases into the mucosa. The relative diffusion rates in humans have been estimated to be 40:2:1 for CO2, O2, and N2, respectively. It is theorized that CO2 and O2 may be responsible for short-term pressure effects and that N2 may be important for long-term atmospheric equilibration.19 Evidence is increasing that an important function of the eustachian tube may be to maintain the N2 pressure gradient and regulate atmospheric equilibration.
The size of the mastoid cavity may be important in the tolerance of rapid or large pressure changes between the middle ear and ambient atmosphere. A larger mastoid cavity provides a reservoir to offset some of the changes, whereas a small mastoid allows for a larger pressure changes with small amounts of air movement. Patients with some eustachian tube compromise during an airplane flight may be more prone to barotrauma if they have small mastoid compared with individuals with a large mastoid.21
Surfactants
Surfactants, which are surface tension–lowering substances, were initially identified in eustachian tube washings in dogs.22 Surfactants occur naturally and are principally composed of phospholipids that reduce the surface tension of a fluid at an air–fluid interface such as in the bronchial tree and eustachian tube. Premature infants born before 28 weeks’ gestation frequently require surfactant supplements for the lungs to expand sufficiently to survive. Surfactants have been identified in the secretions of human eustachian tubes and in the middle ear.23 Surfactants applied to eustachian tubes of rodent models with refractory otitis media with effusion (OME) had significantly reduced passive opening pressures of their eustachian tubes.24,25 A multicenter placebo-controlled study administering oral Ambroxol, an agent to enhance surfactant production, to adults and children found a decrease in the prevalence of OME.26
Intranasal aerosolized surfactants delivered through a metered dose inhaler have been shown to be effective for reducing eustachian tube passive opening pressures in normal rodent models and decreased the duration of effusion in animals with experimentally induced OME. Additionally, animals with experimentally induced acute otitis media (AOM) given these surfactants not only reduced the duration of effusion but also reduced the bacterial load and severity of the infection. It has been proposed that intranasal aerosolized surfactants delivered through a metered dose inhaler may be effective in the treatment of OME and AOM in humans.27
Opening and Closing of the Eustachian Tube
A great deal has been learned about the mechanisms of eustachian tube opening through experimentation with phototubometry, sonotubometry, manometric measurements, contrast radiography, and electrical stimulation of tubal muscles in dogs and monkeys.1,18,28 Contrast radiography in animal models and humans has demonstrated a consistent pattern of opening and closing along the length of the cartilaginous tubal lumen. The osseous eustachian tube remains unchanged and patent throughout the dilatory and closing sequence. The cartilaginous tube is initially closed in the resting position. The dilation begins at the nasopharyngeal orifice and progresses distally toward the bony isthmus. Tubal closure reverses the process progressing from distal to proximal and produces the “pumping action” that has been previously described.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


