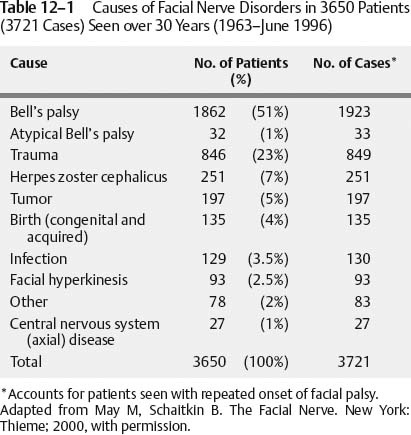
12 Diagnosis and Medical Management of Disorders of the Facial Nerve Although the large majority of cases of nontraumatic, acute onset of facial palsy or paralysis are found to be idiopathic,1 “all that palsies is not Bell’s.”2 It is most important, therefore, that the physician who is called upon to manage such patients be able to rule out other, nonidiopathic causes of facial nerve disorders before any treatment regimen or appropriate referral is considered. The diagnosis of idiopathic (Bell’s) facial palsy requires that all other causes of facial weakness or paralysis have been excluded. Because the management of idiopathic facial palsy is largely expectant and offers a high probability of spontaneous recovery, it is imperative that other, often treatable causes be recognized (Table 12–1).1 In the absence of trauma, the timing and pattern of onset of facial palsy are not particularly helpful in diagnosis because many conditions can begin abruptly or gradually. They are, however, valuable in determining the prognosis for recovery; idiopathic and other presumably viral neuropathies have an excellent prognosis if the palsy never becomes complete paralysis. Regardless of etiology, if sudden onset of palsy does not progress to complete involvement within 14 days, complete or nearly complete recovery of function can be expected in 98% of cases.1 Once complete paralysis occurs within the first 2 weeks after apparent onset, the prognosis for excellent recovery drops to about 75%.1 On the other hand, gradual onset and progression of disease, particularly if no evidence of recovery is noted within 3 to 6 weeks, should raise the suspicion of neoplasm. True onset of idiopathic facial palsy does not necessarily coincide with the first signs of weakness because it is probable that most of these represent viral neuropathies such as herpes simplex or herpes zoster.3 Whether this is true because of direct viral involvement of the nerve4 or indirect inflammatory or pressure changes secondary to edema within the fallopian canal,5 up to 90% of fibers can be affected before clinically evident weakness may be apparent. Although pain can occur in idiopathic (Bell’s) palsy, either preceding the onset of the palsy or concomitant with it, it is more prominent and usually more severe in cases of herpes zoster oticus (Table 12–2). Pain may also be a feature of neoplasm but is more often generalized or headache-like in nature because tumor often produces a gradual loss of feeling in the distribution of the facial nerve. When pain is associated with gradual onset of paralysis, especially if there is a period of twitching or spasmodic activity in the distribution of the facial nerve, neoplasm should be considered the cause until proven otherwise. Pain associated with Bell’s palsy usually subsides spontaneously in up to 14 days, whereas the more severe and almost universal pain with herpes zoster oticus can persist for up to 3 months. Recurrence of facial palsy should suggest a neoplasm, although it can occur in Bell’s palsy and Melkersson-Rosenthal syndrome as well. Pitts et al6 noted a recurrence rate of 13% in a series of over 1000 patients with Bell’s palsy, 38% of these on the same side and 62% on the opposite side. Herpes zoster, on the other hand, has not been associated with recurrent paralysis.1 Alternating recurrent facial paralysis is most often associated with Bell’s palsy, although Melkersson-Rosenthal syndrome typically presents this way. This relatively rare syndrome is characterized by recurrent orofacial edema, cheilitis, and a fissured tongue. These findings, when seen in association with recurrent alternating facial paralysis, are diagnostic.7 Recurrence on the same side is often correlated with tumors involving the facial nerve.1,8
Evaluation
History
Bell’s Palsy |
Acute onset of unilateral facial palsy |
Numbness or pain of ear, face, neck, or tongue (50%) |
Viral prodrome (60%) |
Recurrent palsy (12%) |
Herpes Zoster Oticus |
Same as Bell’s palsy, except pain more common and severe |
Vesicles (transient) on pinna, face, neck, or oral cavity (100%) |
Sensorineural hearing loss and/or vertigo (40%) |
Tumor |
Onset similar to Bell’s palsy or |
Slowly progressive weakness beyond 3 weeks (59%) |
Recurrent same side (17%) |
Adapted from May M, Schaitkin B. The Facial Nerve. New York: Thieme; 2000, with permission.
Bilateral, simultaneous facial palsy is sometimes a medical emergency. Guillain-Barré syndrome, Lyme disease, and acute leukemia have been reported to present this way.1,9 Besides traumatic and congenital causes (which should be apparent to the treating physician), other conditions with simultaneous, bilateral facial palsy include infectious mononucleosis, cytomegalovirus, sarcoidosis, acute porphyria, amyloidosis, and botulism.1
Past medical history may be significant in cases of trauma, pregnancy, or systemic illnesses. Trauma, such as skull fractures, concussions, contracoup injuries, and contusions or lacerations of the face in the distribution of the branches of the facial nerve, can produce palsy or paralysis. Surgical trauma to the facial nerve is most often associated with parotidectomy, but radical neck dissection, submaxillary triangle procedures, repair of mandibular fractures, all procedures involving the temporal bone or the auricle, and skull base and intracranial operations can be implicated.
Pregnancy is associated with a threefold increase in the incidence of idiopathic facial palsy and herpes zoster oticus.10 Peripheral neuropathies occur with some frequency in patients with diabetes,11 alcoholism,12 collagen vascular disorders,13 hypothyroidism,14 amyloidosis,15 and hypertension.16 Isoniazid, used in the treatment of tuberculosis, has been reported to produce peripheral neuropathy in cranial nerves, including the facial nerve.1 Vaccinations against polio, rabies, and influenza have also been implicated in Bell’s palsy, Guillain-Barré syndrome, and bulbar palsies.1,17
Physical Examination
Patients presenting with recent onset of unilateral facial weakness should be evaluated by careful and complete head and neck examination. A thorough cranial nerve evaluation is required, not only to identify the multiple neuropathies that usually accompanies Bell’s palsy, but also because idiopathic facial nerve involvement is often the most prominent complaint in various diseases involving the central nervous system. In many cases, audiometric testing will be essential to this evaluation, and imaging, such as magnetic resonance imaging (MRI) or computed tomography (CT) scanning will also be necessary.
Physical findings in the typical case of idiopathic facial palsy (Bell’s) include the following:
1. Unilateral weakness or paralysis, which does not spare the forehead
2. Tearing from the affected side only
3. Normal corneal sensation (90% of cases)
Facial palsy is evaluated by comparison to the unaffected side. This can best be accomplished by using the examiner’s finger to fix the facial soft tissues in the midline to prevent displacement to the intact side, evaluating each of the facial areas (i.e., forehead, upper lip, etc.) in turn. It must be remembered that patients can present with weakness on one side and paralysis on the other, in which case the lesser affected side may be missed. Central lesions that produce unilateral palsy usually spare the forehead because of the crossed innervation to that area. Because treatment choices and prognosis are both dependent on whether or not paralysis becomes complete, careful observation and, if possible, quantification of involvement of each of the five divisions of the facial nerve should be recorded. The House-Brackmann grading system18 is among the most widely used for this purpose (Table 12–3).
Grade Description Characteristics |
|---|
I. Normal |
Normal facial function in all areas |
II. Mild dysfunction |
Gross: slight weakness noticeable on close inspection; may have very slight synkinesis. |
At rest: normal symmetry and tone. |
Motion: |
Forehead: moderate to good function |
Eye: complete closure with minimum effort |
Mouth: slight asymmetry |
III. Moderate dysfunction |



