Esophageal Disorders
Catherine Rees Lintzenich
Esophageal disorders are commonly encountered in the evaluation of throat pain, dysphagia, reflux, and globus pharyngeus. Knowledge of the motility, inflammatory, and neoplastic disorders is an essential component in the diagnosis and management of these common otolaryngologic complaints.
ESOPHAGITIS
Infectious Esophagitis
Infectious causes of esophageal inflammation include fungal pathogens, viral pathogens and, much less commonly, bacterial pathogens. The most common cause is Candida albicans fungal infection (Fig. 59.1). Risk factors include human immunodeficiency virus (HIV), systemic and inhaled steroids, and antibiotic use. However, esophageal candidiasis is frequently encountered in healthy immunocompetent individuals without risk factors. Pain and dysphagia are the most common presenting symptoms. The appearance of white to yellow plaques on an erythematous base is quite characteristic but may be confirmed with biopsy. It is important to recognize that esophageal candidiasis can be present without findings of candidiasis in the oral cavity or pharynx. Treatment options include topical antifungal solutions or oral antifungals, such as fluconazole.
Viral esophagitis may be caused by herpes simplex virus, cytomegalovirus, or HIV. Typically, multiple shallow ulcerations are seen in the esophageal mucosa. Biopsy is necessary to confirm the diagnosis.
Noninfectious Esophagitis
Pill-Induced Esophagitis
Medications can cause esophageal inflammation and injury via a systemic or local reaction. Systemic medications that relax smooth muscle may increase the incidence of reflux and its sequelae, including esophagitis, dysmotility, and stricture. Examples of drugs causing esophageal effects include alcohol, nicotine, and smooth muscle relaxants.
Alternatively, pills that become lodged in the esophagus can cause direct injury to the mucosa, resulting in stricture, pain, and dysphagia. Large pills, pills taken in the supine position, xerostomia, dehydration, and motility disorders are risk factors for esophageal pill injury (1). Doxycycline, tetracycline, alendronate, and potassium chloride frequently cause such direct esophageal injury. Symptoms include dysphagia, odynophagia, and heartburn. It is important to consider pill-induced esophagitis even when there is no known history of pill becoming lodged in the throat or esophagus. Endoscopic removal of the pill impaction and conversion of medications to liquid forms may be necessary. In severe cases, medications may need to be administered via a nasogastric tube until the esophagus heals. Sequelae of pill-induced esophagitis may include ulceration, stricture, and even perforation of the esophagus.
Eosinophilic Esophagitis
Eosinophilic esophagitis is increasingly diagnosed in both children and adults. This disorder is characterized by eosinophilic infiltration of the esophageal mucosa. Adults typically present with solid food dysphagia, reflux symptoms, and recurrent food impactions (2). Fluoroscopy and endoscopy may reveal a small caliber esophagus with a ringed appearance (trachealization) or esophageal strictures. Small white submucosal lesions may be noted on endoscopy (Fig. 59.2). The mucosa is typically friable and prone to tearing with instrumentation. Alternatively, the esophagus may appear normal. Food and/or inhalant allergies typically coexist with eosinophilic esophagitis. Biopsy confirms the diagnosis, requiring greater than 15 to 20 eosinophils per high power field. Treatments include topical esophageal steroids, allergy treatments, and elimination diets.
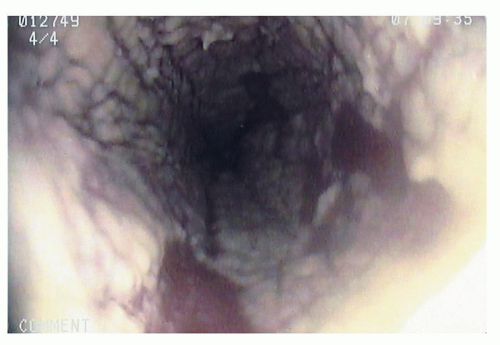 Figure 59.1 Candida esophagitis with white and yellowish plaques. |
GASTROESOPHAGEAL REFLUX DISEASE
Reflux refers to the backflow of gastric contents in a retrograde fashion into the esophagus and sometimes into the pharynx (laryngopharyngeal reflux is discussed in detail in Chapter 66) (3). Gastroesophageal reflux disease (GERD) occurs when reflux is excessive or symptomatic. Refluxate from the duodenum, containing bile acids, may also contribute to esophageal injury. Typical symptoms of GERD include heartburn and regurgitation, with less typical symptoms being cough, globus, and belching.
GERD is probably associated with inappropriate relaxations of the lower esophageal sphincter (LES) and poor esophageal clearance. The endoscopic appearance of the esophagus in GERD may be normal, or esophagitis with erosion and mucosal breaks may be present (Fig. 59.3). The most commonly used classification system for the endoscopic appearance of reflux esophagitis is the L.A. Classification, which takes into account the length, width, and number of mucosal breaks. Strictures can occur with chronic or prolonged esophageal acid exposure. Ambulatory pH monitoring can aid in the diagnosis of pathologic reflux. When reflux esophagitis is present, proton pump inhibitor therapy is initiated to allow healing of the esophageal injury. Endoscopy may be repeated 3 to 6 months after initiation of therapy to confirm healing.
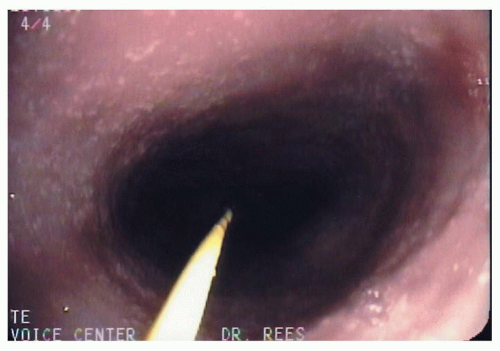 Figure 59.2 Small white lesions sometimes seen in eosinophilic esophagitis (guidewire for dilation is seen in the picture). |
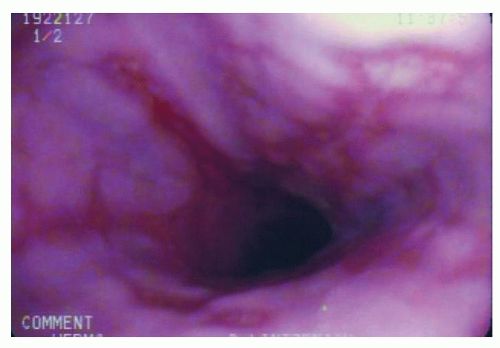 Figure 59.3 Circumferential erosive esophagitis from reflux. |
Reflux is a risk factor for Barrett metaplasia, the presence of which increases the risk of esophageal adenocarcinoma (4). To identify Barrett metaplasia, it is necessary to understand the normal gastroesophageal junction anatomy. The squamous epithelium of the esophagus interfaces with the columnar gastric epithelium at the gastroesophageal junction in the normal setting. This is visualized with a change from a lighter pink to a darker salon-pink in the stomach. Normally, this squamocolumnar junction (SCJ) coincides with the gastroesophageal junction, best identified by the termination of the gastric rugae. When the gastroesophageal junction extends more than 2 cm above the diaphragmatic compression, a hiatal hernia is present. When the SCJ extends proximal to the perceived gastroesophageal junction, Barrett metaplasia is suspected. Suspected areas of Barrett metaplasia must be biopsied to confirm the diagnosis and evaluate for dysplasia. Biopsy-confirmed Barrett metaplasia will include intestinal metaplasia and goblet cells on histopathology. The presence of no dysplasia or low-grade dysplasia indicates low risk for neoplastic transformation. However, high-grade dysplasia represents a significant risk of neoplasm and is usually treated as esophageal adenocarcinoma.
ESOPHAGEAL MOTILITY DISORDERS
Disorders of esophageal motility may be classified as hyperkinetic and hypokinetic. Both classes of motility disorders can lead to dysphagia, globus pharyngeus (feeling of lump in throat), regurgitation, and/or noncardiac chest pain. The mainstay of esophageal function testing is esophageal manometry. The recent advances of high-resolution manometry have allowed for assessment of esophageal pressure along the entire pharynx, upper esophageal
sphincter, esophageal body, and LES (5). High-resolution manometry catheters have pressure sensors at approximately 1-cm intervals. Impedance technology has also added to assessment of esophageal motility. Impedance determines the comparative resistance of air, the bolus, and the esophageal mucosa and therefore indicates bolus transit along the esophagus (6).
sphincter, esophageal body, and LES (5). High-resolution manometry catheters have pressure sensors at approximately 1-cm intervals. Impedance technology has also added to assessment of esophageal motility. Impedance determines the comparative resistance of air, the bolus, and the esophageal mucosa and therefore indicates bolus transit along the esophagus (6).
Hyperkinetic Esophageal Motility Disorders
Nutcracker Esophagus
Nutcracker esophagus is a disorder typically associated with noncardiac chest pain. This condition typically coexists with reflux disease, and there may be a causal relationship between nutcracker esophagus and reflux. Manometric assessment reveals normal peristalsis and high amplitude esophageal contractions during swallowing, with the average distal esophageal amplitude being greater than 180 mm Hg. Bolus transit is typically normal (7), as is fluoroscopy of the esophagus. Treatment for nutcracker esophagus usually involves antireflux treatment and/or pH testing. Surgical esophageal myotomy is generally not effective for this disorder (8). Nitrates and calcium channel blockers may be beneficial in decreasing the intensity of the esophageal contractions.
The etiology of nutcracker esophagus is still unclear, but it may be related to coordination between the longitudinal and circular muscle layers of the esophagus (9). Jung et al. performed high-frequency intraluminal ultrasound in 5 healthy volunteers and 10 subjects with nutcracker esophagus. In the healthy volunteers, the peak contraction of the circular and longitudinal muscles was nearly synchronous. In nutcracker esophagus, there was asynchrony in contraction between these muscle layers in the distal esophagus.
Distal Esophageal Spasm
Distal esophageal spasm (DES) is a nonperistaltic motility disorder, which may or may not be associated with high amplitude esophageal contractions. In manometric terms, greater than 20% but fewer than 100% of wet swallows produce simultaneous contractions, with onset velocity of the peristaltic wave being greater than 8 cm/s. This disorder is also highly associated with reflux disease and is more likely to produce dysphagia and impaired bolus transit. Chest pain is typically associated with higher distal esophageal amplitudes (10). Esophagram may be normal or may show a “corkscrew” pattern during a swallow (Fig. 59.4). The etiology of DES is likely related to alterations in nitric oxide metabolism.
Treatment of DES usually begins with pH testing and/or antireflux therapy. Other treatment modalities are not well supported by controlled studies, but they have shown some possible efficacy in case series. These therapies include phosphodiesterase inhibitors (11), calcium channel blockers (12), peppermint oil (13), visceral analgesics, and botulinum toxin injections (14




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
